
Abstract
We compared quality improvement (QI) interventions for prevention of mother-to-child transmission in a private hospital and a government hospital (GH). From November 2013 to October 2016, data were extracted retrospectively for HIV-positive mothers and HIV-exposed infants. The overall number of mother–baby pairs (MBPs) was significantly (P < .001) higher at the GH (mean = 294, standard deviation [SD] = 180) than the private hospital (mean = 72, SD = 27). There was a significantly higher number of MBPs receiving care (P < .001) and routine services (P < .001) at the GH. The proportion of MBPs retained in care (P < .001) and receiving the routine service package (P < .001) was significantly higher at the private hospital. Overtime, indicators at the private hospital peaked significantly in year 2 and reduced moderately in the final year. The trend for the GH showed gradual but nonsignificant improvement in 2 indicators. QI showed positive results in the private hospital. If systematically applied in GHs, QI can support improved services for larger patient volumes.
What Do We Already Know about This Topic?
QI has been recognized as a viable method to reduce the gap between existing care delivery processes and the best possible care in resource-limited environments.
How Does Your Research Contribute to the Field?
Comparing the implementation of QI within a FBO and a public hospital highlights the relevance of a specific operating environment to the QI process.
What Are Your Research’s Implications toward Theory, Practice, or Policy?
QI can be well implemented but can be limited by the factors unique to the health system. This is a starting point for further exploration on factors that impact QI implementation.
Introduction
Vertical transmission of HIV is a significant problem in Lesotho. 1 Mother-to-child transmission (MTCT) of HIV is the main source of HIV infection in children. 2 The Joint United Nations Programme on HIV and AIDS estimates that more than 90% of children acquire HIV through MTCT during pregnancy, labor, delivery, or breastfeeding. 3 Since a significant proportion of HIV-infected infants die in the first year of life, prevention of mother-to-child transmission (PMTCT) services provide an opportunity for securing the health of both mothers and children in Lesotho. 3 The Partnership for HIV-Free Survival (PHFS) 4 was implemented in Lesotho to improve PMTCT services by accelerating adoption of World Health Organization (WHO) updated guidelines that emphasize the importance of optimal feeding practices to the survival of HIV-exposed infants (HEI).
In partnership with the Ministry of Health (MoH), the US for International Development (USAID) Applying Science to Strengthen and Improve Systems (ASSIST) Project applied quality improvement (QI) methods to tackle barriers to PMTCT service delivery. Quality of care mediates the inputs of the WHO health systems building blocks (service delivery, health workforce, information, medical products, vaccines and technology, financing, and leadership/governance) to generate outputs that include improved health. 5 Specifically, QI has been recognized as a viable method to reduce the gap between existing care delivery processes and the best possible care in resource-limited environments. 6 Although the QI process can be implemented correctly, success is not always guaranteed and can be moderated by context, including the characteristics of the organizational setting, the environment, individuals, and their roles in the QI project. 7 Contextual factors that impact the technical aspects of QI can vary across health systems such as Lesotho where care delivery is undertaken primarily in government-managed facilities and faith-based organizations (FBOs). Faith-based organizations provide 42% of health services under the coordination of the Christian Health Association of Lesotho (CHAL). 8 The prominence of FBOs in the health system occurred under a World Bank–funded Health Sector Reform Program that encouraged public–private partnerships with significant investments in infrastructure and equipment as well as human resources of CHAL facilities by both the World Bank and the African Development Bank. 9 Differences in contextual factors, including philosophy, organizational structure, leadership, and financing, across the 2 organizations influence the service delivery environment. The philosophy guiding FBOs is to provide compassionate care to people in need, with a commitment to the patient’s dignity along with consistent best practices in providing decent care. Christian Health Association of Lesotho institutions have historically had a strong system for leadership and management that has been committed and accountable, 8 whereas the complicated chain of command and decision-making power at government facilities defeats decentralization initiatives designed to impart more authority (particularly in relation to decision-making) to government departments and facilities. 10,11 Annual financial assistance from the government to FBOs is dependent on the performance of each individual facility, whereas government facilities are supported regardless of performance. 10 Also, there is an observable disparity in staffing patterns with perpetually vacant key positions and lower staff skills and competencies at government facilities. 12 Prior to the introduction of the PHFS in Lesotho, there was no formal QI intervention aimed at the PMTCT program. The PHFS applied QI methods to PMTCT services to learn how to best achieve better outcomes for HEI in both government and FBO facilities. Given the differences in the government and private health sectors in Lesotho, we expected that implementation might be impacted by the different operating environments in the health system.
Methods
Selection of Hospitals
To compare QI between government and FBO facilities, we purposively selected 2 hospitals: a privately managed faith-based hospital in Thaba-Tseka district and a government-managed hospital in Mohale’s Hoek district. Both hospitals were in the same improvement collaborative, sharing the same improvement aims, and core indicators, therefore providing an opportunity to assess how similar processes affect the same core measures in different operating environments.
Quality Improvement Implementation
Using QI methods, the PHFS supported existing country-specific PMTCT protocols and nutrition assessment, counseling, and support activities. The contents of the health service packages as presented in Table 1 are based on the 2013 National PMTCT Guidelines. The package includes all routine services that are to be provided to the mother (nutrition assessment, refill of antiretroviral, family planning, etc) and the child (immunization, prophylaxis, nutrition assessment, infant and young child feeding and counseling, etc) at each scheduled monthly appointment. Time-specific critical services for infants (eg, DNA-polymerase chain reaction at 6 weeks) are also provided at the appropriate time as per national guidelines.
Lesotho PMTCT Routine Visit Health Services Packages.

Abbreviation: PMTCT, prevention of mother-to-child transmission.
Quality Improvement Initiation at the District Level
Access to each hospital was facilitated by the respective District Health Management Team (DHMT). This team has oversight responsibility over all health activities in a district. At the request of the DHMT, ASSIST held an initial sensitization meeting to introduce the DHMT to QI principles and approaches. After the initial meeting, a formal QI training was conducted. Participants included staff from the district facilities (health centers and hospitals), DHMT members, and representatives from the private sector. At the end of the training, a district-level coaching team was established, with QI coaches who were nominated to supervise and guide the QI work of individual facility QI teams, acting as mentors. Optimally, the coaches were expected to visit their assigned facilities at least 2 times in a month.
Quality Improvement Processes Within the Hospitals
Following operationalization at the district level, implementation of the QI processes was instituted at the facility level. In November 2013, all staff at the 2 hospitals were trained on the basics of QI, including the rationale of forming the QI teams, by staff of the USAID ASSIST Project and the DHMT. The facility QI teams included staff that work in the relevant areas of service delivery, with knowledge and understanding of the implications from system changes, as well as the ability to effect even the smallest change in their environment. Other than health workers, QI teams also included customer service representatives who interacted consistently with patients on a daily basis. Once the QI teams were formed, a rotational leadership was established, and a team leader was identified by the team members. Subsequently, the roles and responsibilities of the rest of the team were defined.
Facility teams were trained to use the plan-do-study-act (PDSA) cycle to test changes to improve care processes. In this model, a change believed likely to yield improvement is proposed. A plan is developed for testing the change, the plan is implemented, and the effect of that test is studied (by monitoring selected process indicators) to see whether the change did in fact yield the improvement expected. What action is taken next is based on the result of the test. 13 Both hospitals were in the same improvement collaborative, a shared learning system that brings together many teams to work together to rapidly achieve significant improvements in processes, quality, and efficiency of a specific area of care, with the intention of spreading these methods to other sites. All teams in the improvement collaborative shared the same improvement aims and core indicators. Quality improvement teams identified problems and selected an intervention, choosing indicators to monitor the intervention’s effect on the desired process. If the change yielded the desired improvement, it was then instituted as part of the care process. If it did not, the change was either discarded or modified before being tested again. A compendium of changes was tested one by one toward collectively improving the various target indicators. Teams met fortnightly to monitor and record progress on changes being tested. As part of the collaborative approach, quarterly learning and sharing sessions were organized by ASSIST. These brought together QI teams from across multiple districts where different teams reported on their progress, shared changes that worked, and discussed the impact of the changes on selected indicators.
Measuring QI
Monthly aggregate data on HIV-positive mothers and HEI were extracted retrospectively from the month of the first coaching visit in Lesotho (November 2013) over a 3-year period until October 2016. The first time period is characterized by a lack of available data in both hospitals across all the indicators, particularly indicators 2 and 3. The indicators (including the numerators and denominators) are defined in Table 2. Indicator 1 is the percentage of MBPs who were retained in care for 24 months postnatally, representing the MBPs who consistently sought care over the 24 months, out of the number of all HEIs extracted from the under-5 register. From the denominator, we excluded MBPs who had transferred out, were lost to follow up (3 consecutive months of nonattendance), or who had died. Indicator 2 is the percentage of MBPs who received the complete routine service package. These are the MBPs who received the complete standard package of routine services (as defined in Table 1) out of those MBPs who were retained in care at the facility in the reporting month. Indicator 3 is the percentage of MBPs with complete and accurate medical records. This indicator has the same denominator as indicator 2, and the numerator is the number of MBPs with records that are complete and accurate. If all records for a given patient (the entire patient card and the corresponding entries in the registers) had all necessary information and were fully and correctly filled out, the record was considered complete and accurate. The records were reviewed daily for accuracy by a designated staff member as part of the QI process.
Comparison of Indicators and Patients (HIV-Positive Mothers and HIV-Exposed Infants) at the Hospitals (November 2013 to October 2016).

Abbreviations: ART, antiretroviral therapy.
ns P > 0.05; *P ≤ 0.05; **P ≤ 0.01; ***P ≤ 0.001.
We compared the indicators overtime for the entire 3-year period for each of the 2 facilities as well as between the private and the government facility. A t test was used to assess the significance of the difference in mean for the selected indicators and the patient volume (numerators and the denominators) for the 36 monthly observations.
To examine the trend, we charted the indicators together with the numerators and the denominators overtime, for each hospital. The implementation period was divided into three 1-year periods: year 1 (November 2013 to October 2014), year 2 (November 2014 to October 2015), and year 3 (November 2015 to October 2016). We used the nonparametric Wilcoxon signed-rank test to determine the statistical significance of a difference in the medians from 1 year to the next. The Wilcoxon signed-rank test is a nonparametric test that determined the differences between the periods based on the order in which the observations fall within each period. Unlike the parametric t test, there is no assumption of normal distribution, and the test is more appropriate for the small number of repeated observations overtime in the same hospital. 14 -16
Ethical Approval and Informed Consent
Data used for this analysis were collected during routine service delivery at the hospitals and did not include private patient information that required institutional review board approval.
Results
Comparison of QI Implementation at the Hospitals
Table 3 compares the QI implementation processes across the facilities. Although QI teams were formed in both hospitals with support from the respective DHMT, the team at the government hospital (GH) was not functional. Ownership for the QI process was limited at the GH, whereas the private facility team demonstrated ownership of the identification of gaps and formulation of improvement aims. Testing of changes, progress monitoring, documentation, and institutionalization of changes were done consistently at the private facility but did not occur at the government facility. Both hospitals engaged in learning and sharing. Overall, the QI processes were more successful at the private hospital than at the GH.
Comparison of QI Implementation Processes at the 2 Hospitals (September 2013 to October 2016).
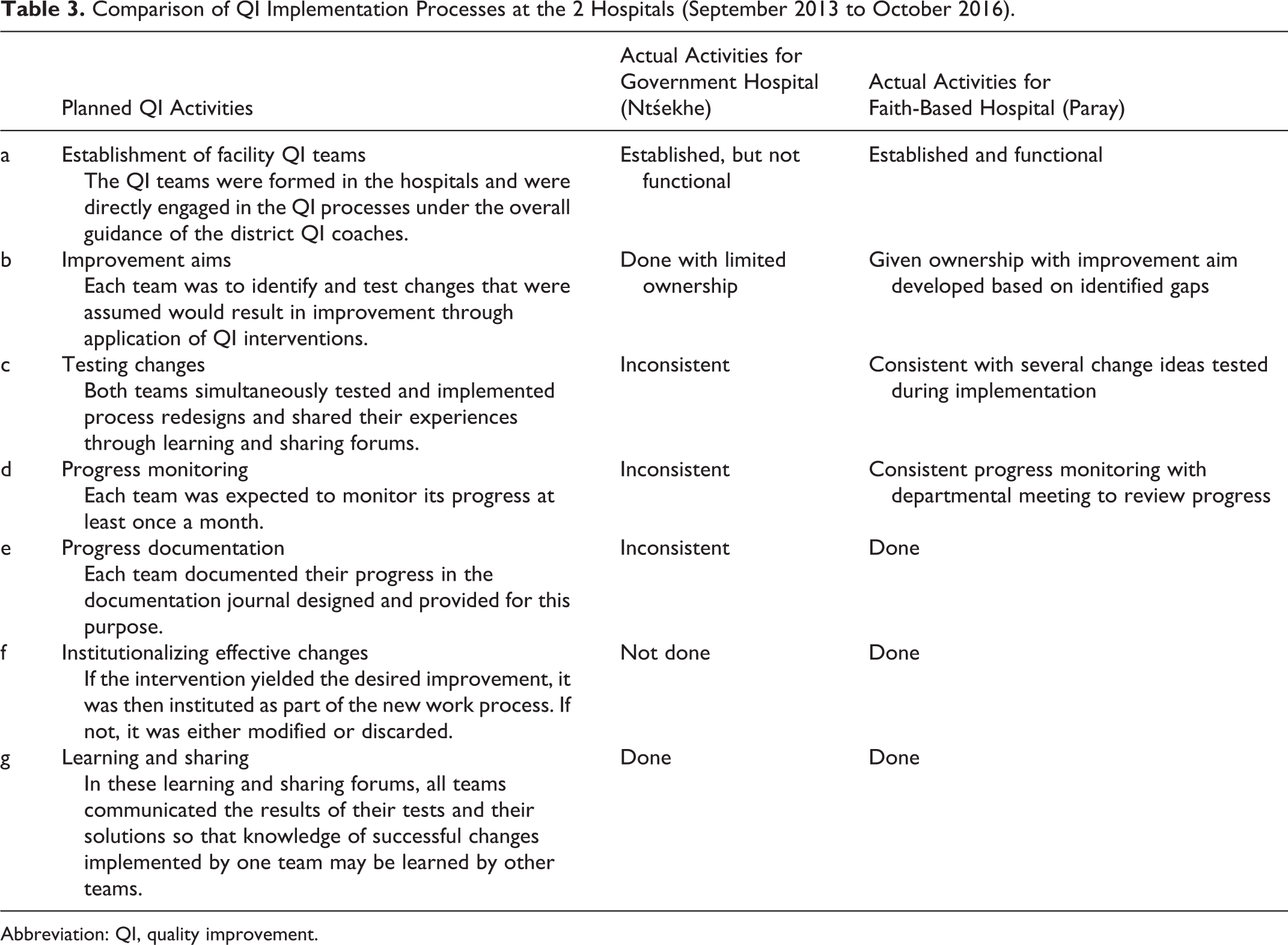
Abbreviation: QI, quality improvement.
Comparison of Patient Volume and Indicators between Hospitals
As shown in Table 2, the results from the t test for the overall 36 months show significant differences in mean for the 2 hospitals. The monthly average number of MBPs at the GH was 294 (standard deviation [SD] = 180.2) compared to 72 (SD = 27.3) at the private hospital; the difference was statistically significant (222.5, P ≤ .001). Given the higher patient volume, it is expected that a significantly (P ≤ .001) higher number of MBPs received antiretroviral therapy and under-5 care at the GH (mean = 79.04, SD = 54.70) than at the private hospital (mean = 42.37, SD = 22.80).
The mean percentage of MBPs retained (indicator 1) was significantly higher (P ≤ .00001) and about double at the private FBO (65.5%) in comparison to the GH (32.91%). The average percentage of MBPs receiving the standard package of care (indicator 2) was significantly higher (P = .0005) at the private FBO (87.10%) than at the government facility (65.76%). The difference in mean for data accuracy (indicator 3) between the hospitals was not significant.
Comparison of Indicator Trends
The trends for the 3 indicators were compared from the first month of coaching visits in Lesotho in November 2013 until October 2016. There was a gap in reporting at both the FBO (August 2014 to October 2014) and the GH (March 2014 to December 2014). Figures 1A and B, 2A and B, and 3A and B show a side-by-side comparison of performance of the 3 indicators overtime at the 2 hospitals.

A, Private hospital: retention of mother–baby pairs (November 2013 to October 2016). B, Government hospital: retention of mother–baby pairs (November 2013 to October 2016).

A, Private hospital: mother–baby pairs receiving standard package of care (November 2013 to October 2016). B, Government hospital: mother–baby pairs receiving standard package of care (November 2013 to October 2016).

A, Private hospital: data accuracy and completion (November 2013 to October 2016). B, Government hospital: data accuracy and completion (November 2013 to October 2016).
For the retention of MBPs in care for 24 months (indicator 1), the trend at the private hospital remained consistently higher despite an initial poor start in the first 4 months. The private hospital reached a high of 100% after 2 years of implementation (November 2015 and December 2015). Between year 1 (November 2013 to October 2014) and year 2 (November 2014 to October 2015), the gain in the median at the private hospital was very significant (48.6 percentage points, P ≤ .01) and double that at the government facility (24 percentage points). The decrease in the median between year 2 and year 3 was significant at the private hospital (16%, P ≤ .05). The GH demonstrated a lower but consistent improvement in the median each year, but the gains were not statistically significant.
Performance on the provision of the standard package of services (indicator 2) was higher at the private hospital than at the GH. At the GH, 75% of MBPs received the complete routine package in the initial month of January 2014. But the indicator was unstable, attaining 100% in 5 months of the 36-month period, first in July 2016 with several declines and improvements in between, dropping as low as 48% in May 2016, and then back up to 100% by July 2016. The private hospital also experienced fluctuations with poor documentation in the initial year of implementation. The year 1 median (82.3%) was not an accurate representation of the situation at the private hospital because only 1 data point was available. Similar to the retention indicator, the median for year 2 (November 2014 to October 2015) reached 100% with a significant decrease in year 3 to 80.3% (P ≤ .01). Despite the lower yearly median at the government facility, it increased gradually by 2.3 and 3.9 percentage points, respectively, in year 2 and year 3, yet the improvements were not significant.
Performance on the accuracy of data on MBPs (indicator 3) showed pronounced fluctuations at the GH, starting from 87% in November 2013, dropping very low to 17% in March 2015 and even lower to 5% in August 2016, only to increase again to 49% in September 2016. At the private hospital, this indicator was scored at 0% (due to the lack of data) in the 6 months of the first year when it was recorded. At the start of the second year (October 2014), it was 94%, reaching and remaining at 100% from January 2015 to August 2015. It declined again to 71% in September 2015, then remained at 100% from October to December 2015, after which performance stagnated at approximately 74%. In year 2, the private hospital was able to confirm accuracy and completeness of almost all records with a median of 100% (P ≤ .01) in year 1. The median decreased significantly by year 3 to 74.3% (P ≤ .01). At the GH, the median decreased consistently overtime from 69.2% to 63.4%, then to 53.4%, but the decrease was not statistically significant.
Discussion
The implementation of QI was more successful at the private faith-based hospital. The GH QI team showed difficulty in their ability to fully implement and operationalize each step of the QI process. Retaining MBPs is a prerequisite to delivering required PMTCT services and improving quality of care for the HIV-positive mothers and HEI. 17,18 Although patient volume was higher at the GH, the GH was unable to capitalize on this advantage and offer more routine services or more accurate records for MBPs. Data accuracy and completeness is critical because it impacts all indicators and can reflect actual processes of care within the facility if done properly. Also, the PDSA cycle hinges on accurate data. Data help determine whether the tested change has merit and should be sustained. 19
The stronger QI implementation and subsequently the higher performance on all 3 indicators at the private hospital could be because of various interdependent factors across the system, organizational, and QI team levels that provided a viable environment for the operationalization of the QI process. At the system level, the introduction of QI in Lesotho coincided with a period of serious political instability in the country 20 that impacted the implementation process in 2014. From April 2014 to November 2014, there was no project counterpart in the government sector to facilitate access to senior management, the district health management teams, and facilities in the crucial early stages of the PHFS implementation. There was a moratorium that prevented implementing partners engaged with PHFS from accessing district teams and facilities. There were also multiple changes in the senior management of the MoH. The political instability took a greater toll on the public hospital, with the public management structure being directly impacted by the changes at the MoH; so although there was a break in QI implementation at both hospitals, the private hospital recovered within a month compared to the government facility, which was inactive for 8 months, as shown by lack of data during these months.
Recognized differences across the service delivery environment between the government and private hospitals included facility infrastructure, organizational structure, leadership principles, financing strategy, and staffing. Investment at the private hospital improved the infrastructure and equipment, which are linked to improvement in clinical processes and subsequently improvement in health quality indicators. 21 Performance-based financing, which was implemented at the private hospital, is generally designed to improve both quantity and quality of care, 22 with some studies demonstrating improved quality from performance-based financing interventions. 23,24 Strong leadership is important to QI, as the leadership directly influences QI culture and controls resources, including staff time, needed for the improvement. 25 The government facility was more likely to be hindered by the pseudo-decentralization and the complicated chain of command that neither encourages autonomous leadership nor ownership on the part of leaders and staff within the hospital. The less complicated organizational structure of the private hospital, guided by a mission of benevolence at the FBO, was likely to support the viability of QI work.
Staffing can have a major impact on the QI teams and a direct impact on the ability to carry out the technical aspects of QI. Staffing for maternal, newborn, and child health (MNCH) services at the private hospital was approximately 1.5 times higher in comparison to the GH. 26 This resulted in a higher caseload at the GH, where staff cited lack of time and a shortage of staff as a main barrier to their performance. Faith-based organizations attract better skilled staff, and turnover is limited, so the QI teams were better prepared to institutionalize changes, and minimal resources were allocated to orienting new team members. Shorter rotation periods at GHs (quarterly) translated to a higher frequency of rotations at this facility compared to the private hospital, where rotations occurred biannually. Consequently, team members at the GH had a shorter time to understand and internalize the QI process. Overall, the shorter rotation period at the GH adversely affected the continuity of service provision, and staff that rotated into PHFS-related positions from non-PHFS sites were not familiar with the basic tenets of the improvement activity. At the private hospital, 2 staff members were selected as the focal points to ensure data accuracy and completeness daily. However, the private hospital also encountered a disruption resulting from staff absence, as the decline in the data accuracy indicator in September 2015 (71%) was directly attributed to the absence of the PHFS focal person in the facility that month due to annual leave. District QI coaches did not conduct quarterly coaching visits as scheduled, so supervisory support to the facilities was not optimal.
Despite general instability and inability to sustain performance on the indicators at both hospitals, the private hospital performed relatively better, improved faster, and was able to sustain improvement longer on the indicators compared to the GH, a possible advantage resulting from the better contextual factors noted at the private hospital.
Strengths and Limitations
The strength of this pilot project lies in the ability to demonstrate how differences in the service delivery environment between a private hospital and a public hospital in Lesotho can impact QI in a resource-constrained environment. Findings from this implementation provide an opportunity to tease out the relevance of contextual factors to the success of a QI project in the health service environment. In addition, the lessons learned can inform implementation strategies that consider the strengths as well as limitations of health-care facilities.
The receptivity of QI in Lesotho by the government stakeholder was important to the overall success of the program, and early ownership by the government occurred when the MoH leadership adopted a unique name for PHFS, “Acceleration of PMTCT.” Ownership by the government is important to the success as well as sustainability of donor-funded development initiatives. 27 -30
Yet, there are existing issues within the Lesotho hospitals that limited the success of QI implementation. Documentation is particularly poor. Health workers are either not trained or are unable to use the formal registers. This leads to intermittent use of registers, improvised registers, and incomplete records. Also, the hospitals had inexperienced staff who lacked orientation on the workflow of the hospitals, thereby complicating the QI processes. There were problems with the definition, quantification, and reporting of selected indicators. For both facilities, nutrition supplements were out of stock for the first 18 months of the project, which meant that malnourished patients did not receive treatment.
The findings from this project are not generalizable to other hospitals in the country or region. Rather, it serves as a snapshot of implementation activities and lessons learned in the service delivery environment that can impact PMTCT and overall MNCH health services in Lesotho.
Conclusion and Recommendations
The aim of PHFS was to accelerate the improvement of PMTCT services in Lesotho using QI methods. Given the differences across the service delivery environment for the 2 major stakeholders in health service delivery in Lesotho—CHAL and the Government of Lesotho—we compared QI implementation at hospitals managed by each one of the stakeholders. Our findings show that the private hospital performed better than the GH. The faith-based hospital was characterized by better contextual factors (leadership, organizational structure, performance-based financing, higher skilled staff, recent investments in infrastructure) that were likely to support successful implementation of QI and subsequently performed better on the PMTCT indicators.
Preceding QI implementation, it is helpful to engage in an exercise that identifies the contextual factors in the health service delivery environment and rank these factors on their strength and relevance to the health delivery environment under improvement. This will help the leadership and QI team to develop and test changes that are likely to lead to success, by tackling those contextual factors within their immediate control.
Factors that are not within the immediate control of the QI team or organization should be addressed by overall health system strengthening activities. Better-functioning health systems can ultimately lead to better success of attempts to improve clinical processes and subsequently health outcomes. 31 Investing in infrastructure at the GHs, strengthening the public–private partnership with the CHAL, and continued investment in health systems strengthening can support improvement in quality of care and ultimately improve HIV and MNCH indicators. The Government of Lesotho stands to benefit by adopting some of the more successful factors at the FBO such as improving leadership and management, ultimately elevating autonomy as well as ownership at the district level and the facilities.
Footnotes
Acknowledgments
The implementation of PHFS in Lesotho was a collaborative process among several stakeholders.The authors acknowledge the leadership and support of Dr ‘Nyane Letsie, the Director General of Health Services in the Ministry of Health as well as the QI coaches and QI teams in the hospitals who implemented the PHFS in Lesotho. We also recognize the invaluable support provided by Ms Lisemelo Seheri, senior nutrition officer in the Family Health Division. Her tireless and selfless support was a critical factor in ensuring the success of the project. The authors also appreciate the technical support and guidance provided by Amy Stern, Anisa Ismail, and Edward Broughton of URC.
Authors’ Note
Kelello L. M. Lerotholi and Aurora O. Amoah equally contributed to the writing of this manuscipt.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by USAID and PEPFAR. Funding for this work was provided by the US President’s Emergency Plan for AIDS Relief (PEPFAR) through the US for International Development (USAID) and its Applying Science to Strengthen and Improve Systems (ASSIST) Project, implemented by University Research Co, LLC (URC), through Cooperative Agreement number AID-OAA-A-12-00101.