
Abstract
Plain Language Summary
This study explores HIV care provider perceptions of patient-centered care (PCC) by analyzing common themes that arose in interviews. We found that providers perceived PCC to be holistic, individualized care focused on respecting patient comfort and security and actively engaging them as partners in care. Providers discussed a variety of ways in which they practiced PCC at the individual service level through psychosocial and logistical support, through their interpersonal relationships with respectful communication and trust, and through more structured facility level policies and activities such as greater service integration and employing a diverse staff. PCC is rapidly becoming the new standard of care and this study hopes to offer insight into provider perceptions of PCC and examples of practice in the HIV care field.
Background
HIV continues to be a serious health issue globally with 38.4 million people with HIV (PWH) worldwide and 1.5 million new cases in 2021. 1 In the USA, of an estimated 1.2 million PWH, 13% remain undiagnosed. 2 Large gaps of care exist along the HIV care continuum. In 2020, of those diagnosed with HIV, 66% initiated antiretroviral treatment (ART), half were retained in care, and just 65% were virally suppressed. 2 These findings are concerning if the UNAIDS goal of ending AIDS by 2030 is to be achieved.
Patient-centered care (PCC) has been proposed as key to improving HIV care models by improving quality of care, and reducing wasted time, resources, and patient loss to follow up stemming from fragmentation of care processes 3 under current provider-oriented healthcare systems. The World Health Organization (WHO) has formally adopted PCC as a priority and incorporated people-centered care as part of their global strategy with five goals focused on empowering and engaging people, strengthening governance and accountability, reorienting the model of care, coordinating services, and creating an enabling environment. 4 Pertaining to HIV care, UNAIDS has adopted three people-centered targets by 2025 including comprehensive HIV services, people-centered and context-specific service integration, and removal of societal and legal impediments to an enabling environment for HIV services. 5 A consortium of HIV experts from around the world also recently issued a consensus statement of 31 points to guide stakeholders from the subnational to global level in advancing the long-term well-being of PWH through improving health systems response in a patient-centered approach which has been endorsed by 67 organizations worldwide. 6
The Institute of Medicine (IOM) defines PCC as care that is “respectful of and responsive to individual patient preferences, needs, and values, and ensures that patient values guide all clinical decisions.” 7 PCC approaches improve health outcomes 8 and satisfaction with care 9 while reducing costs. 10 A systematic review of 40 PCC interventions in diverse settings around the world found an overall positive relationship with clinical outcomes including improved health behaviors, self-management of chronic disease, follow up rates, lab results (HbA1c, SBP), and better communication and satisfaction. 8 In the context of HIV care, PCC interventions demonstrate improvements in linkage,11,12 retention,12,13 adherence, 14 and viral suppression15,16 while also leading to greater patient satisfaction 17 and patient-provider relationships.14,18,19
Despite clear benefits, a lack of consensus on the conceptualization, ideal framework, measures and implementation strategies for PCC in HIV care settings persists,6,20 impeding the implementation of high-quality PCC practices. For example, in HIV care settings, there is a greater focus on structural components of PCC application, and less emphasis on interpersonal (patient-provider) factors despite their critical role in promoting good care. Moreover, while the evidence base for PCC frameworks and application is more established in the US, studies focused on PCC specifically in HIV care settings tend to concentrate on the sub-Saharan African region where HIV is more prevalent. US-based studies exploring application of PCC to HIV care are necessary given differing sociocultural contexts and patient preferences as well as structural factors like human resources, logistical complexity and cost effectiveness, which may limit generalizability of differentiated service delivery interventions country to country. 21 Additionally, despite large racial and ethnic disparities in HIV care outcomes, little work has been done to explore PCC factors that may mitigate these gaps with implications for diverse populations like South Florida. Exploratory qualitative work among PWH of racial and ethnic minorities suggests PCC approaches are desired by these patients and feeling cared for by one's provider is highly valued, empowering patients to engage in care and manage their HIV. 18 Providers play a critical role in shaping patient behavior and the patient-provider relationship has been shown to have a large impact on patient engagement, adherence and retention in care,22,23 yet surprisingly few studies explore how HIV providers perceive PCC.
Greater efforts to understand PCC as interpreted by HIV providers, as well as through empirical evidence generated through implementation of PCC practices within HIV care settings are critical to fully leveraging its benefits to improve HIV treatment and outcomes. This study aims to characterize the perceptions and practices of PCC among HIV care providers in the Ryan White Program.
Methods
Study Design: This is a qualitative analysis of 20 in-depth, semi-structured interviews with HIV care providers at 13 case management programs funded by the Ryan White Program (RWP) in south Florida. These data were collected as part of a larger study exploring health care provider and women-centered HIV care practices that mitigate the effect of adverse sociocultural factors on adherence and retention. This study was conducted in accordance with the Consolidated Criteria for Reporting Qualitative Research (COREQ) statement and the checklist completed. 24
Study population: In this study, we analyzed the interviews of 20 HIV care provider volunteers including 10 medical case managers (MCMs), seven physicians and nurses, and three RWP administrators. This breakdown was determined beforehand to ensure representation from different provider types and across sites. To be included, participants had to belong to one of the provider types above and have worked with RWP clients for at least two years.
Setting: The RWP is a provider of last resort serving uninsured and underinsured PWH living at or below 400% of the federal poverty level, about 50% of PWH in the US, over half a million people. Part A of RWP provides funding to metropolitan areas such as Miami that are particularly affected by the HIV/AIDS epidemic. 25 The program's funds cover medical and nonmedical support including MCM, legal, food and nutrition, dental, transportation, and mental health services, as well as peer support and substance use therapy. HIV providers in this study were recruited from clinics and programs serving RWP clients in Miami-Dade County, FL.
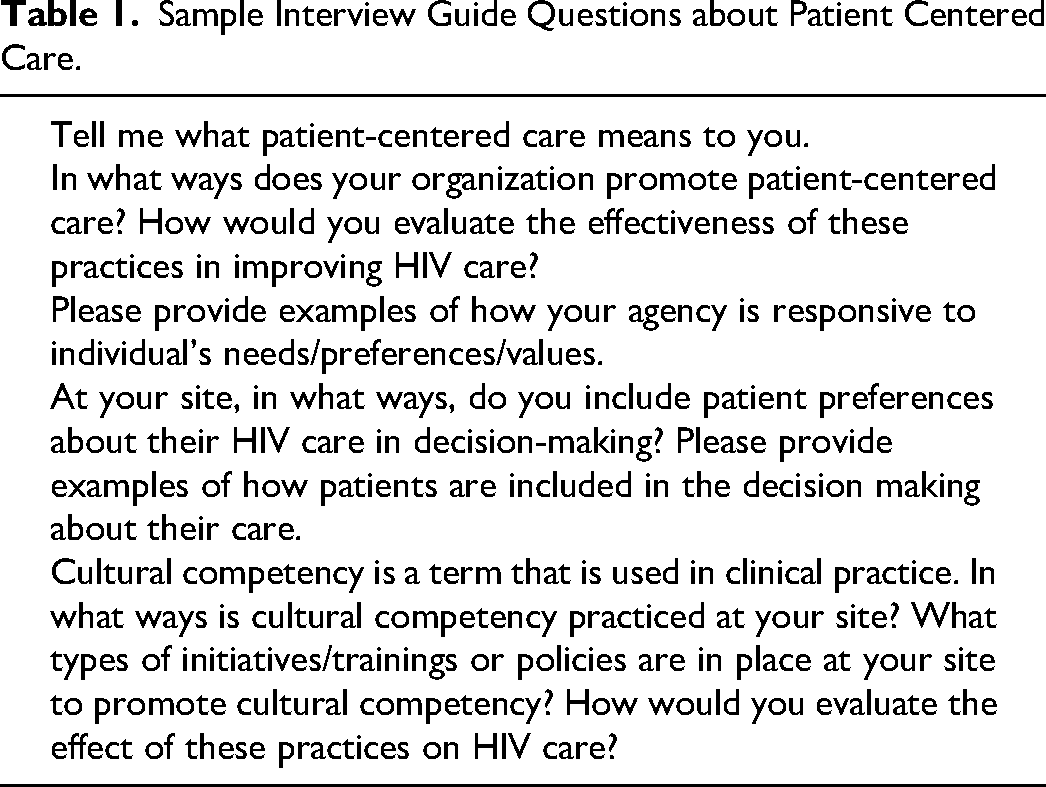
Data Collection: The study's principal investigator and a coinvestigator recruited, consented and interviewed the participants. Interviews took place in a private room on site and participants received a $100 incentive for their time. Interviews followed a semi-structured guide of original questions not previously tested in other settings (example questions in Table 1), were audio-recorded, and lasted approximately 60-90 min. Digital recordings were transcribed verbatim.
Sample Interview Guide Questions about Patient Centered Care.
Ethical Approval and Informed Consent: This study received approval by Florida International University Institutional Review Board (Ref #106958). Privacy and confidentiality were maintained at all times by conducting interviews in private rooms, deidentifying data, and following strict safe data storage protocols. All participants gave written informed consent prior to participation.
Analysis: Transcripts were uploaded into NVivo 12, 26 a text organization software for data organization and management. Data were coded in two stages. First, all interviews were coded using a structured process to enable formation of codes aligning with a priori themes in the interview guide adapted from the IOM's PCC framework 7 and identified core consistencies in the data pertaining to our first objective of exploring provider perceptions of PCC. In a second stage of coding, a multi-level HIV care conceptual model was created, adapted from the socioecological model, 27 to organize the results pertaining to the second objective of understanding the different levels where PCC is practiced. Utilizing this model, current practices that embody PCC were further coded. Two coinvestigators independently reviewed and coded all transcripts, applying thematic analysis to create a preliminary codebook. Coding then followed an iterative process to allow for open coding as additional themes and example components of each type of practice emerged. Coders met regularly for discussion and consensus where discrepancies arose. For example, interdisciplinary collaboration was mentioned by multiple providers who spoke about formal, facility level practices such as standing meetings or messaging protocols to enhance communication between different providers when making decisions about patient care. Discussion and consensus led to creation of a new code at the institutional level of practices in our model.
Results
Participant Characteristics: Table 2 includes sociodemographic characteristics of the 20 study participants. The majority were female (85%), Black or African American (55%), and served as case managers (55%). Most participants had over 10 years of experience working in South Florida (65%), with HIV patients (65%), and RWP clients (60%).
Participant Sociodemographic Characteristics (N = 20).
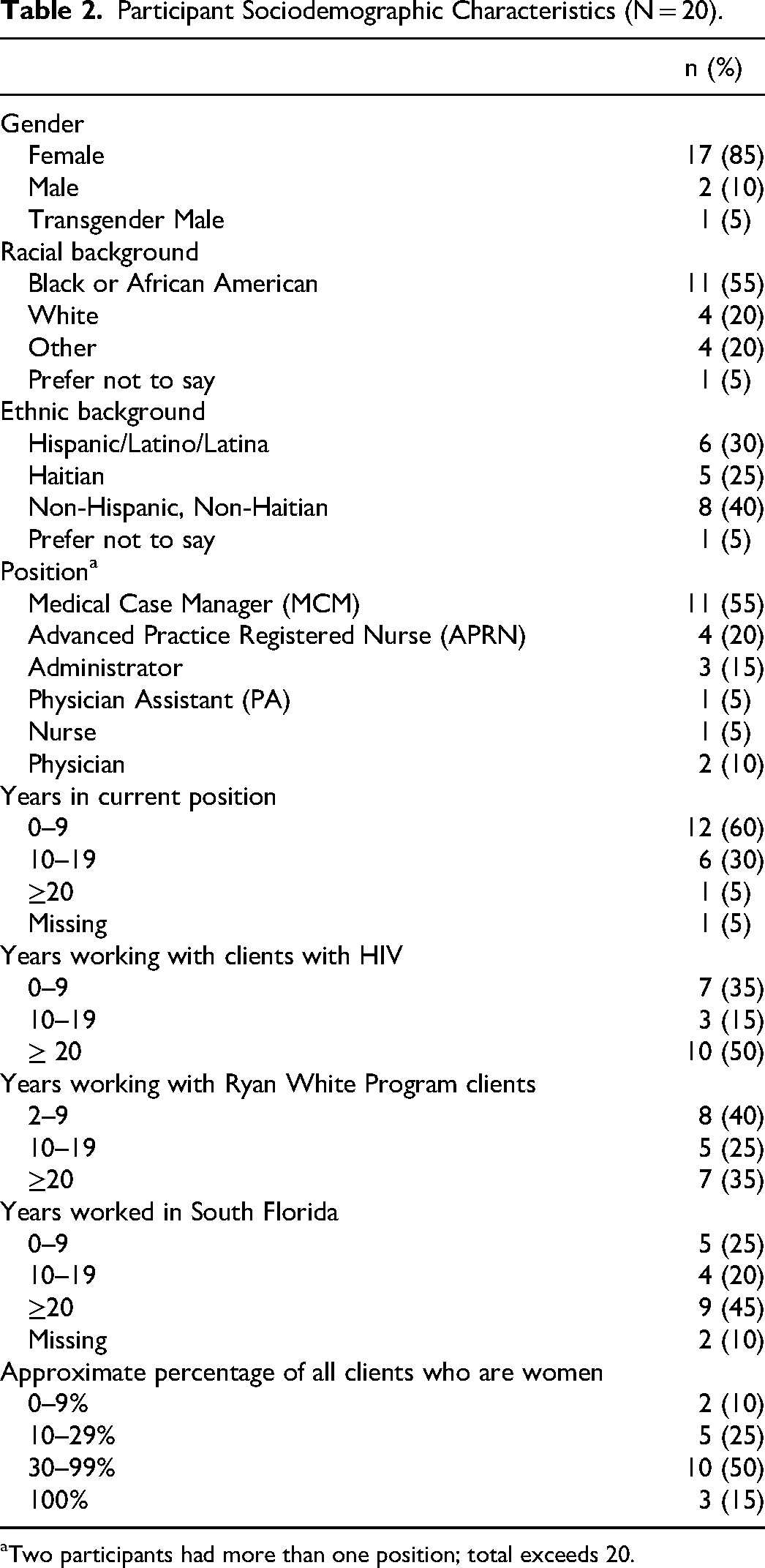
Two participants had more than one position; total exceeds 20.
Summary of Main Findings.
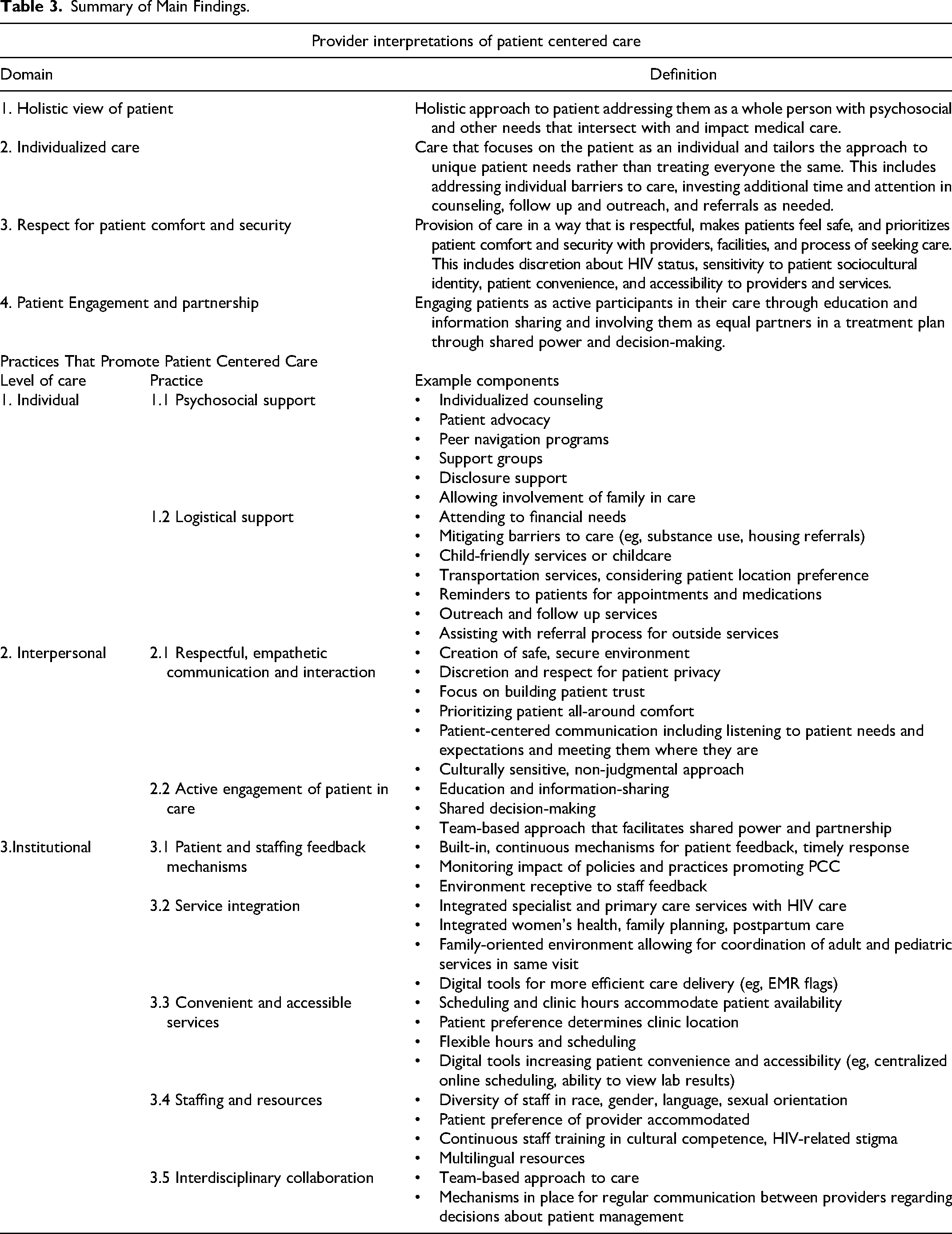
Summary of Main Findings
In line with the first objective of this study, provider perceptions concerning definitions of patient-centered care (PCC) emerged under four main domains (see Table 3): 1) holistic view of patient, 2) individualized care, 3) attention to patient comfort and security, and 4) patient engagement and partnership. Regarding the second objective, practices that providers perceived to foster PCC in their work occurred at multiple levels: 1) individual level support which included direct psychosocial and logistical support, 2) interpersonal support through the patient-provider relationship which included respect for patient comfort and security, and active engagement of the patient in their care, and through 3) institutional policies and practices that promote PCC including patient and staffing feedback mechanisms, service efficiency and integration, patient convenience and access to services, and staffing and resources.
Domains of Patient-Centered Care as Interpreted by Providers
Holistic View of Patient
Providers described PCC as involving a holistic approach to patients, addressing them as a whole person with mental, spiritual, psychosocial, and emotional needs beyond their HIV treatment. This involved acknowledgment of the multidimensional realities of patients’ lives and incorporation of needs related to these areas in a comprehensive treatment plan. Providers agreed that needs not directly related to their HIV care nonetheless often intersected with and impacted it. Thus, inclusion of these needs as part of the care plan was critical to successful HIV treatment. “Patient-centered care, it's looking at the patient from many facets, you know, mental health issues, socioeconomic issues, their family, support system and social network, and also their health issues.” (Physician/Administrator, ≥20 years’ experience with RWP clients)
Another provider noted that patient wellness and satisfaction was their goal versus a problem-focused approach, “Patient-centered care means to me, it's basically focusing all around the patient's care. From basically their wellness, dealing with their behavioral aspect, dealing with their all-around wellness. Basically, when I provide care to my patients, ensuring that when the patients leave here, they’re satisfied, and dealing with everything that has to do with the patient. And not just problem-focused.” (APRN, 2-9 years’ experience with RWP clients)
Individualized Care
Providers noted that individualized care was another important aspect of being patient centered. This referred to care that focused on the patient as an individual with unique needs and tailoring the approach accordingly rather than treating everyone the same. Some examples included investing additional time in counseling, follow up and outreach, and referrals as needed. “To me it means that, we take the care of the patients individually. It's just not lumped up into one sum, because some patients may need more services than others. If we can give them those services as opposed to just having like a limited, like, you come in here, we just give you a pill, and you go. But some patients may need therapy, you know some sort of therapeutic services, dental services, and you can offer all of those now.” (MCM, 2-9 years’ experience with RWP clients)
Another provider shared an example of creating an individualized care plan incorporating preferences regarding pill size and diet to optimize medication adherence, “So, adherence is like when they don’t like large pills. So if I don’t know you like large pills and I’m giving you the biggest pill, are you going to take your medicine? No. So again, it's to learn about the person you’re serving. It's so they can adhere to it. Again, if they don’t eat, you can’t give them a medicine they take with food. If they eat, you want to give them something they take with food. If they have stomach issues, you don’t want to give them something that's going to give them more acid and more burn cause they’re not going to take it.” (APRN, ≥20 years’ experience with RWP clients)
Respect for Patient Comfort and Security
Provision of care in a way that is respectful and prioritizes patient comfort and security with providers, facilities and the process of seeking treatment was another aspect of PCC described by providers. “It's to let them know that they are, first of all they are safe. They are like, in a place like they can feel comfortable no matter what they have happen around them. In here we can provide all that they’re looking for which is love, very important, compassion.” (MCM, 10-19 years’ experience with RWP clients)
Another aspect of creating a comfortable environment of care included respecting and accommodating patients with diverse backgrounds. “It means having respect for the patient…being sensitive to, you know, their different cultural identities and preferences.” (Administrator, ≥ 20 years’ experience with RWP clients)
Comfortable care also included patient accessibility to providers and services. “To me it means that the patient gets to see me. And gets to have a doctor, all the time. In which they feel comfortable. And they choose who to see…To me ideally, will be that the patient feels comfortable to come and see me all the time.” (Physician, 2-9 years’ experience with RWP clients)
Patient Engagement, Education, and Partnership
Engagement of patients as active participants in their care through education and information sharing was highlighted by many providers as an important component of patient centered care. In a move away from more paternalistic models of care, they noted a PCC approach should involve patients as equal partners in their treatment plan and decisions about their care, including medication preferences, procedures and ancillary services related to their HIV care. “It means…making sure that you involve the patient in decision making about their care…It's making sure you educate them about whether it's the medications or how to take them, or if you’re doing procedures, explaining the procedures so they understand and if they have to make decisions about options, that they know what those are and can make better choices.” (Administrator, ≥20 years’ experience with RWP clients)
Many providers commented that working with patients in a team-based approach was also essential. “I always say, we are a team. I can’t do it without you. You can’t do it without me either, we’re doing it together.” (APRN, ≥ 20 years’ experience with RWP clients)
Patient-Centered Care Practices
Individual Patient Support
Providers described multiple patient centered services that assisted patients directly at the individual level mainly through psychosocial and logistical support.
Psychosocial Support
Psychosocial support took the form of assistance managing psychological, behavioral and social aspects of illness through individualized counseling, patient advocacy, peer counselors and patient navigators, support groups, and support for disclosure. At a basic level, providers shared that just being there for patients and creating a supportive space in which to deal with their condition and related challenges was essential, and this was common across provider types. “I really do think it comes back to knowing that they have us here for support. At the end of the day that's what they really want, to be heard, to know that someone understands them… having access to a peer counselor and having access to that personal touch. That really makes a difference, having someone that they know can relate and someone that can, that understands them… That extra personal touch, the case managers provided that. The Ryan White case managers provided that, and the clients look forward to it. They look forward to seeing their case manager and having that relationship with them.” (APRN, 2-9 years’ experience with RWP clients)
Providers also tried to customize support by connecting patients with staff experienced in unique patient issues where possible. “I have one of my colleagues…who does substance abuse but she's been living with HIV for about 23 years, so she knows. Sometimes I tell them, ‘talk to this lady one-on-one and explain to her what it is that you have to go through, your experience,’ so that they feel that they have a support person. If I’m not here or, somebody is here and you need to have somebody to talk to, she will listen to you, encourage you, to get the services that are available.” (MCM, ≥20 years’ experience with RWP clients)
Taking extra time to counsel and support patients with attention to their individual needs was described as important by providers. “Ok if the patient hasn’t been coming, why? Is it work? Is it family? Is it the bus? Is it money? Is it homelessness? It's centered around, you have to know what's going on with the patient to help them…The extra mile to me makes a big difference. And I think when we take the time to actually really talk to the patient and then the extra mile, that makes a big difference…Just saying no is not enough. ‘Oh well, we don’t do this service’, then what do the patient do? So if we don’t do the service, it's my responsibility to figure out where to send you to get the help, to get the service. That's patient-centered care to me.” (APRN, ≥ 20 years’ experience with RWP clients)
Peer counselors who spoke with patients and helped them navigate the healthcare system and myriad of services involved, especially when first diagnosed, was mentioned as a critical part of psychosocial support. They also helped ease the referral process and provided hope for patients by serving as living proof that they too could live a healthy life regardless of their HIV diagnosis. “They kind of stopped bringing them directly from the Department of Health. I always send them with [the peer navigator] first day, and that seemed to help a lot. Like I can tell you, the referral to behavioral was a little easier, having her here. Because they cannot feel like, oh my God it's not that bad. She looks great, so yeah.” (Physician, 2-9 years’ experience with RWP clients)
Encouraging patients through the process of disclosure of their HIV status was another powerful way to deliver psychosocial support and was seen as mutually rewarding. “As a case manager I experienced that and it was very powerful to see that, to have you know, someone be newly diagnosed who wants to disclose to their partner and doesn’t know how to do it and wants that emotional support from us. And that was very touching, not only for her but for me.” (APRN, 2-9 years’ experience with RWP clients)
Support groups were mentioned by many providers as a conduit for the delivery of direct psychosocial support to patients. Many explained that being able to connect with other individuals also struggling with a new HIV diagnosis was helpful and made patients feel less alone. Where possible, providers described efforts to personalize care by offering support groups for particular subgroups of patients including transgender patients, patients dealing with substance use issues, and women with HIV. “We even have a transgender working here and the clients when they come, they love her. It's like, ‘Oh my God! This is great! I feel I can have someone to talk to.’ And you know the support groups…I have about 7 transgender in my caseload and they are all happy, ecstatic. I think it's the least supported group and it's tough, I get choked up because you know it's hard for them to not only disclose, to live, to feel supported, so that knowing that they have a place where they can come and have that support is priceless.” (MCM, 10-19 years’ experience working with RWP clients)
Logistical Support
Logistical support included assistance mitigating many of the barriers that commonly contribute to suboptimal care such as provision of transportation services, childcare options, referrals for substance use and housing assistance, connecting patients to financial resources and incentives, care coordination and assistance with the referral process for outside services, reminding patients for appointments and medications, and outreach services. Providers shared that care coordination comprised a big part of their job, helping to reduce patient loss to follow up and expedite access to prescribed treatment. “The coordination has helped with retention in care tremendously…being able to transition women who don’t have a primary care provider into some place that's onsite, that their patients are familiar with. We are able to retain them better in care because otherwise you know, sometimes they go back to their provider and sometimes they get lost.” (Administrator, ≥ 20 years’ experience with RWP clients)
Providers noted that care coordination also helped facilitate complex referral processes for specialist or outside services. Assistance with the logistics and paperwork involved greatly impacted whether or not patients successfully connected to those services. “Sometimes if the client needs to see a gastroenterologist, or any other specialist…we have to print and e-fax the referral…and when we get the authorization, sometimes we call the client to tell them to come in, pick it up. Some of my clients that I know they are able to schedule an appointment, but some that I know are not gonna do it. If I cannot do it, I have my peer counsellor help them schedule their appointment. We fax over the referral and the authorization to the particular place that they are gonna go. Sometimes if they need transportation, we provide transportation for them.” (MCM, ≥ 20 years’ experience with RWP clients)
Many providers commented on the importance of taking the time to individually remind patients to follow up with their appointments and take their medications and the impact of this investment on adherence and retention. “I have several individuals text me every night to make sure that they are taking their medication. So, that's one extra thing that me, that I personally do with the clients to ensure that they’re doing what they need to do for themselves… They text me to let me know that they take their meds… And it's just simple, the thumbs up with the ‘Ok,’ as in, ‘Ok I got your text’… just applauding them in their own effort, congratulating them for doing what they need to do. Just letting them know that life is so much bigger than what they’ve been told.” (MCM, 10-19 years’ experience working with RWP clients)
Another provider shared experiences utilizing different adherence strategies with patients depending on their unique challenges to taking their medications. “One of the pharmacies…they would do what's called like, I think it's bubble packing. But they would basically put the medication for each day in little capsules, and all you had to do was pop and take them. So, we actually have a patient that's on multiple medications. She's pregnant. She has a history of seizures. So that's one thing that we’re doing for her because there's just so much medication, it's hard for her to manage…I encourage them mainly to set alarms too. if they haven’t disclosed to their partner, to get a pill box. Like different things, and we work closely with the pharmacist, like I said, and our case manager here and social worker to try to encourage them to take the medication.” (APRN, 2-9 10 years ‘experience with RWP clients)
Providers also helped patients navigate financial barriers to care by taking time to connect them with the right resources or strategically schedule their appointments to avoid unnecessary costs and reduce the financial strain. “So, let's say they don’t qualify for the Ryan White program. We look at patient assistance programs or certain types of sliding scale fees. We have created policies just based on patient needs that are HIV positive. Just to better assist them because the goal is for them to remain in care.” (MCM, 10-19 years’ experience with RWP clients)
Financial incentives, free meals, food vouchers, and provision of material resources were also noted as ways to make care more patient centered. “We really try. We have baby clothes, we have gifts bags for the moms that are delivered, pink and blue. I mean, we really, really try…Because we want these women to stay in care.” (APRN, 10-19 years’ experience with RWP clients)
Accommodating patients with transportation and childcare needs was also described as a helpful form of support by many providers. “If they don’t have transportation, we arrange transportation for pick up drop off. Just make sure that they stay in care.” (MCM, 10-19 years’ experience with RWP clients) “We try to tell them that they can bring the kids to the office. Its ok, we’re a family friendly office so…sometimes it can be where childcare can be a challenge for them.” (APRN, 2-9 years’ experience with RWP clients)
Interpersonal Support
PCC practices at the interpersonal level focused on optimizing the patient-provider relationship in ways that were patient centered, through focusing on respect for patient comfort and security, and active engagement of the patient in care.
Respectful, Empathetic Communication and Interaction
Providers built relationships based on respect and empathy by creating an environment where patients felt safe, comfortable, and understood. This was achieved by focusing on building patient trust, exercising discretion and respect for patient privacy, utilizing patient-centered communication, and taking a culturally sensitive, non-judgmental approach to care. Providers shared that patient centered care depended a great deal on the relationship built between the patient and provider, the foundation of which consisted of making patients feel comfortable by building rapport and gaining their trust. “When a patient comes here, they go through us first…Of course, we do an assessment, and it's basically the whole life of the patient. And you know, somebody sit there the first time, they don’t know me, they have to try to get empathy with the patient about the disease, number one. Then, they now start asking personal questions. Once they get in confidence with me, then they start talking to me…they open to me and are more comfortable about their personal issues.” (MCM, ≥20 years’ experience with RWP clients)
Many times, this trust was dependent on patients understanding that providers would not disclose their HIV status. “They’re not scared to look for healthcare. They scared that you going to tell their business to other people… So once they get to know you more…Yeah, they open, so you get more into them. Let's say they come with one thing. They tell you that one thing, and then when they see, ‘Oh she's nice! I can tell her more.’ And then they tell you more and more. They open and then they get more help.” (MCM, ≥ 20 years’ experience with RWP clients)
Providers shared that treating patients without judgment improved patient-provider relationships. “All of us come and we all help you, so I think they see that we’re caring enough, we’re all trying to help you out. So they feel like, ‘hey, you treat me like I’m a human being, like a person,’ not because you have HIV but because you’re a human being. We know HIV is part of you, but we don’t look at, ‘Oh, you have HIV!’ I think that makes many of them feel that we care about them.” (MCM, ≥ 20 years’ experience with RWP clients)
Taking a patient centered approach to communication and understanding patient perspectives and priorities was described as key to mitigating barriers to care and strengthening relationships. “I think for us as far as an agency trying to understand not just the needs of somebody with HIV but bring it to understand the needs of a woman. For example, if we have a woman that's married that's HIV positive, and there's a family that she takes care of, as an agency we need to understand that more than likely her priority isn’t going to be taking a pill every day. And her forgetting or maybe not thinking that's a priority [because] taking care of her family is a priority for her…we need to understand and keep that in mind as we’re going through, ‘hey, ok we see your viral load is up and why is it up?’ Well, the question should be, ‘What is going on? Is it other things that are happening? Why you’re not taking this? Are there problems at home that make it a barrier? How can we assist?’” (MCM, 2-9 years’ experience with RWP clients)
Active Engagement of Patients in Care
Providers considered involving patients in their treatment decisions and taking the time to educate and inform them about HIV and its treatment as equal partners was an important aspect of providing PCC. Including patients in choices surrounding their antiretroviral medication regimen was a big part of incorporating their preferences in the treatment plan. “Sometimes they ask for a regimen simplification, which is an option…we’re definitely open to anything they have to say.” (Physician Assistant, 2-9 years’ experience with RWP clients)
Several providers commented that encouraging patients to advocate for themselves in encounters with other healthcare providers was another way to engage patients in care. “One of the things that we try to do on our end is try to empower our clients to talk to the doctor, whenever they’re in, say, ‘Hey look, how comfortable are you in asking this question?’ A lot of the times we’ll hear, ‘Well, I don’t really ask questions.’ You’re sitting there saying why not? This is about you. You know if you don’t tell that doctor what's going on…That doctor is not a mind reader.’ So we try to empower our patients and clients to ask questions. There's not a dumb question. And if you feel rushed, stop the doctor and say ‘hey look, I feel rushed. I have some questions that I need some answers for,’” (MCM, 2-9 years’ experience with RWP clients)
Providers explained that tailoring the counseling and education to patients with different backgrounds and health literacy levels was key to effectively imparting information and enabling patients to take ownership of their health and care. “Education is the key. If you educate them, they know what they have and they are more liable to taking care of themselves. You meet at the person's level, because every one of us have a different background, different education. So you already know what level you can go to with the patient in order for the patient to understand. Because you’re here for them. You’re not going to throw words at them that they don’t understand, and then they leave and don’t even know what they were here for.” (MCM, ≥ 20 years’ experience with RWP clients)
Institutional Policies and Practices Promoting Patient Centered Care
At the institutional level, providers noted policies and practices that fostered an environment of PCC.
Patient and Staffing Feedback Mechanisms
Some providers noted that their sites had built-in patient and staff feedback mechanisms and continually monitored the impact of PCC practices to improve on them. “The surveys. During the assessments, every 6 months we have to do an assessment with them and ask them questions. We ask for their feedback or input on anything that they feel that was lacking, or you know even positive feedback…like, ‘hey do you have any concerns? What would you like to see improve? And what have you seen that we’ve improved that has helped you?” (MCM, 10-19 years’ experience with RWP clients)
Providers also noted that when facilities were responsive to patient feedback, their input was helpful in creating new initiatives and improving care practices to better accommodate patient needs and overcome barriers to care, especially scheduling availability. “We have a suggestion box. We have advisory boards. One thing we do is we see clients’ needs. Things are being developed on a regular basis. For example, as of last month we have extended our hours to 9 o’clock. So now, we have on call hours we work. We open up till 7 o’clock and we have on call hours from 7 to 9.” (MCM, 10-19 years’ experience with RWP clients)
When patient feedback suggested an unmet need for transgender patients, creation of new services was met with improved satisfaction and outcomes. “Support groups, yes because we did like a survey and we asked the community what we were lacking, what we can improve and it was like the biggest thing discussed…[the response is] fabulous. One of the biggest things we’ve seen is improvement in adherence because they have that support that was lacking.” (MCM, 10-19 years’ experience with RWP clients)
Providers shared that at the facility level, monitoring quality of care and prioritizing PCC contributed to improvements in patient outcomes. “We have a score card. So we look at the patient health outcomes from their initial visit: CD4, viral load, how many visits they had, if they are receiving mental health, dental care …we have seen the changes, we keep the patients engaged at all aspects of the appointment. Let's say, even before the appointment, we do a pre-call, so we check the system and see what's needed. And after the call, you know after the visit we do post visit calls, and then we actually see the data. Our retention rate is at 87% right now. Because it's a score card, every staff name has been evaluated so there's transparency. It pushes everyone to fully evaluate the patient and follow up, make sure within the organization everyone is pushing for viral suppression.” (MCM, 10-19 years’ experience with RWP clients)
Service Integration
Integration of services to increase efficiency of patient care pathways was a major component of PCC mentioned by all providers including care coordination, offering services in one location and visit, and the use of digital tools for more efficient care delivery. “We try to offer many services under one roof. In our big sites, we have our own pharmacy, our case managers are here, the providers are here, of course. We do our labs here, so we try make it as much as possible one-stop shopping.” (Physician/Administrator, ≥ 20 years’ experience with RWP clients)
Integration of services for families by coordinating pediatric and adult appointments in order to avoid multiple visits was another way to make services for efficient. “If they’re coming for their own kids, sometimes the organization has pediatric care, so sometimes they come here and then they make the same appointment with their kids.” (MCM, 2-9 years’ experience with RWP clients)
Providers noted the utility of digital features in electronic medical record (EMR) platforms and other data management tools in facilitating the process of monitoring patient labs and adherence. “Sometimes as the case manager, we look at the lab results, we notice that they are not undetectable. We say, ‘hey there's something going on because what we do is that every month we print from the SDIS system…the clients’ labs, the clients who have high viral load. So we target those clients and find out what's going on. ‘Why your viral load high? What's going on? You taking your medication?’ Even if it's coming to do labs, you need to see the doctor. We call ADAP to see if they’re picking up and all of that.” (MCM, ≥ 20 years’ experience with RWP clients)
Convenient and Accessible Services
Providers emphasized that practices supporting patient convenience and access to services were key to optimal PCC including accommodating patient availability through flexible hours and scheduling, allowing patients to choose their clinic location, being flexible to change based on the patients’ needs, and use of digital platforms to allow patients to schedule their own appointments and view labs. “I like our organization because we do have sites that have extended hours. And that offers people flexibility. Like they can come early to do their labs, we’re open at 8. They can come in after work to see the doctor because we’re open till 7 on Tuesdays and Thursdays, and we’re here on Saturdays. So, we have the flexibility.” (MCM, 2-9 years’ experience with RWP clients)
At some facilities, providers explained that patients were able to schedule their own appointments through centralized systems and online. “I don’t know what it is, a 1-800 or 1-954 number that when patients call after hours or whatever something goes to centralized booking. Patients can also make their appointments online.” (Physician/Administrator, ≥20 years’ experience with RWP clients)
Providers also considered patient home address and location preferences in decisions about where to receive care to foster greater convenience. “We try to find them [Ryan White providers] close to their home, so that we won’t have someone in [the north] having to go all the way [south] to see a provider cause that's a huge inconvenience. Especially you know, we don’t know if they have money to travel that far. So we try to use their address as a key indicator for where to send them.” (MCM, 2-9 years’ experience with RWP clients)
Staffing and Resources
Availability of a well-trained, diverse group of providers to care for patients, in terms of language, gender, sexual orientation, race and ethnicity, and allowing patients to choose providers according to their preference and comfort level, was noted by many providers to be a strong component of PCC. “Our nurse practitioners, we have Creole speaking, Spanish speaking, and we have someone who just speaks English. All the support staff are bilingual. So we try to work with patients and see if they have a preference, one that speaks their language or someone who has the same cultural identity. We try to make that happen.” (Administrator, ≥20 years’ experience with RWP clients)
Providers noted that being able to work with staff that they identified with helped patients feel more connected, contributing to greater patient satisfaction and quality care. “I am gay, so when I meet those patients, they feel comfortable talking about their preferences. So because I am gay they prefer talking to me more…and like, we can share all of the thoughts.” (MCM, 10-19 years’ experience with RWP clients)
Institutional implementation of staff education and training in cultural competence and HIV-related stigma was also noted by providers as helpful in promoting PCC. “We’re required every year to complete cultural competency training…It's pretty effective because company wide, we have about 30 countries represented…So we’re able to discuss that and pass the information along, and it's really really effective. And it also allows us to use each other as a resource. We have a Haitian person here who speaks Creole, and I can call upon her and be like ‘Hey, in your culture….?’, cause see I have this patient and I’m confused, and we’re able to have those discussions.” (MCM, 2-9 years’ experience with RWP clients)
Interdisciplinary Collaboration
Providers shared that taking a team-based approach to care and prioritizing clear communication with other providers for decisions about the patient helped the team overall provide PCC. “Creating that collaboration…it's either we’re going to work as a team or that patient is going to fall through the cracks somewhere…if everybody is on the same page and knows where that client is at each step, then internally we can assist our client with what they need.” (MCM, 2-9 years’ experience with RWP clients)
Providers described multiple ways in which they communicated on a regular basis to discuss particular patients, such as through in-person meetings, monthly calls, or through the EM.These spaces for regular inter-provider communication allowed for an interdisciplinary approach to care and for different providers to share different aspects of the patients’ health and treatment. “In each division, the clinic, the doctors meet with us, the case managers. Mental health meets with us as well. That way everybody is on the same page and knows where that client is, as far as in their health, their life, as far as what's going on. If they come in and they see the doctor, and if the doctor sees something that maybe we can help them as far as medical case management, they’ll let us know. So it becomes a collaboration, which is great because I know where the client is at all times.” (MCM, 2-9 years’ experience with RWP clients)
Discussion
The main findings of this study demonstrate that HIV care providers perceive PCC to consist of taking a holistic view of the patient, providing individualized care, respecting patient comfort and security, and treating patients as partners through education and engagement in care. PCC practices occurred at multiple levels with the individual level consisting of psychosocial and logistical support, the interpersonal level focusing on respectful and empathetic communication, and patient education and information sharing, and the institutional level involving patient and staffing feedback mechanisms, service integration, convenient and accessible services, and staffing and resources.
Our findings regarding how providers define PCC are consistent with themes in previously proposed frameworks8,28–43 and align with priorities outlined by the IOM and WHO. Though our findings coalesced under four main domains, themes in other conceptual models also appeared throughout our results, including those in a recent scoping review outlining nine common elements in PCC: empathy, respect, engagement, relationship, communication, shared decision-making, holistic focus, individualized focus, and coordinated care. 30 Holistic, whole person approaches to care with incorporation of the biological, psychological and social context has been found to be a core component of PCC,28,42,44 emphasizing wellness encompassing medical, personal, cognitive, emotional and spiritual needs. Consistent with our findings, individualized care has also been highlighted as an important component of PCC in the literature3,36 manifested through personalized treatment goals, 45 flexibility in adapting to patient needs,46,47 and willingness to deviate from standardized processes and established norms to customize care for unique patient interests. 48 Active engagement of patients in their care and approaching the patient-provider relationship as one of partnership rather than paternalism is a core tenet of many PCC frameworks3,20 and our findings support this.
Of note, the importance of making patients feel comfortable and safe was emphasized by providers in our study and emerged as a separate domain. While overlapping slightly with themes of respect49,50 and empathy, 30 this stood out as a much more basic need focused on security and trust, especially as it related to protection of confidentiality regarding HIV status and disclosure. Fear of disclosure as a major aspect of the patient experience when dealing with an HIV diagnosis has been well documented. 51 Thus, PCC applications to HIV care settings may need to dedicate attention to ensuring environments of security. Notably where this was addressed, focus was largely on nonjudgmental and destigmatizing communication strategies to guide counseling, though lacked examples of more concrete practices to bring forth this important element of PCC. More specific and structured action points would be helpful for optimal implementation and operationalization of PCC in HIV care, especially on a larger scale. Also highlighted in our study, providers defined PCC in part by patient satisfaction and how patients felt about their care. Increasingly, patient perceptions52,53 and incorporation of their needs and expectations into the design of care delivery systems54,55 is becoming standard practice.
We present our findings of PCC-promoting practices in a multilevel framework. Interventions focused on direct services to the individual miss opportunities to address larger macrolevel factors impacting care. A multilevel approach ensures PCC is implemented at all levels of care and responds to global calls4–6 for shifting the entire paradigm toward a culture of PCC. Within the individual level, the significance of psychosocial56–58 and logistical support to PCC models has been recognized in other studies.3,20 HIV MCMs are particularly well-suited to address these factors with a holistic approach that targets an individual's clinical and non-clinical needs including psychosocial, emotional, financial and spiritual aspects and has been shown to improve adherence, retention 59 and quality of life by comprehensively helping patients navigate barriers to care. Barriers identified in this study including lack of transportation and childcare, competing responsibilities, food and housing insecurity are common in this patient population and helping patients navigate these challenges is key to effective PCC. 20 At the interpersonal level, our findings highlighting the importance of the patient-provider relationship22,23,60 built on a foundation of trust,61,62 respect and strong communication 28 to make patients comfortable is consistent with other studies. Patient centered communication was the most common component in a recent review of PCC models. 28 Prioritizing patient education and information-sharing as a strategy to promote shared decision-making and actively engage patients to take ownership over care is also not a new concept and is found in many other care models suggesting its critical role in PCC. 63 Transforming the patient-provider relationship into a partnership built on principles of equality and teamwork with shared power and decision-making is particularly important in the context of an HIV epidemic evolving towards a more chronic condition. Navigating ART regimens among a rise of patients with multiple comorbidities and the medication complications this entails will require providers to rely more on patients to alert them to side effects from drug interactions. Thus, its incorporation into PCC models is critical to HIV care settings.
At the institutional level, greater integration of services was a major element of PCC according to providers in this study, consistent with other studies. This is especially relevant to HIV care given the many clinical and wrap-around services coordinated under RWP, which serves half of all PWH in the USA. RWP facilities were among the first to implement multidisciplinary, coordinated, team-based approaches to meet the multidimensional needs of HIV patients beyond specialist care and thus unintentionally were early adopters of the patient-centered medical home PCMH.64,65 The PCMH model applies a holistic lens to the continuum of care at the system level and is an optimal foundation for increasing efficiency, integration and coordination of service delivery. 30 Expansion of PCMH principles of integration within RWP facilities may also help meet the evolving needs of PWH in managing the complexities of multimorbidity requiring comprehensive chronic disease care in addition to HIV treatment. 66 Offering services that are convenient with flexible scheduling, minimal wait times and accessible was also found to promote PCC, consistent with the literature.45,52,57,58,67,68 Hiring practices that facilitate diverse, culturally competent staff and multilingual resources reflective of the patient population is another key institutional feature of PCC. 23 Being able to identify with one's provider allows for improved relationships, in turn facilitating partnership, connectedness and better outcomes.23,69–74 This is critical given that provider cultural competence scores have been found to impact adherence and viral suppression75,76 among patients, with low scores being associated with greater racial disparities in these outcomes. Thus, our findings suggest continuous cultural competence training in places with large racial and ethnic minority populations like South Florida is particularly important for successful PCC implementation and is one way to mitigate disparities since HIV/AIDS disproportionately impacts racial and ethnic minorities. 77 Lastly, interdisciplinary collaboration between multiple providers for individual patients was a key finding aligning with other PCC models. 3 Pharmacists in particular may represent missed opportunities for patient centered approaches. A study exploring a pilot pharmacist-based medication management program serving 7018 HIV/AIDS patients in California found more patients remained adherent and on single ART therapy compared to programs without community pharmacists, and were less likely to use contraindicated regimens or have excess medication refills. 78 Pharmacy-based interventions have thus been associated with decreased viral load79,80 and increased CD4 count. 79 Given the key role of ART in HIV, leveraging the pharmacist role as part of the care team beyond dispensing drugs may have potential to improve outcomes. 81
This study has some limitations. Providers were RWP employees who volunteered to complete interviews outside of work hours. Thus, our findings may not be representative of RWP providers in South Florida more broadly. Social desirability and self-report bias may also have impacted participant responses, though research assistants were well trained to help mitigate these effects. Our sample was also 85% female, which may limit generalizability though findings are not meant to be generalizable, in line with qualitative research goals and study design. Barriers to implementation of PCC were also not directly addressed in this study and did not arise as a point of focus among participant responses, thus real-world implementation context to guide future efforts was minimal in this regard.
Notable strengths of this study include sampling a group of seasoned providers with a majority having over a decade of experience working with HIV patients and RWP clients. Inclusion of a variety of provider types allowing for analysis of PCC at multiple levels beyond direct client care through case management where previous work has focused is another strength. Inclusion of program administrators allowed for additional perspective given their broader responsibilities enabling them to address higher level PCC practices at the institutional level. For example, administrators brought up formal cross-facility efforts to integrate HIV services under one roof, protocols to improve convenience and access to services, and programs targeting improved retention; whereas case managers tended to focus on individual level practices such as tailored counseling, wrap around services to mitigate individual barriers to care, and other forms of psychosocial support. Thus, providers may have differing priorities when practicing PCC depending on their specific role and scope of practice, and this should be factored into future implementation efforts given that certain provider types may be more well-suited and better equipped than others to focus on practices at a given level.
Future studies could focus on patient perspectives, especially because utilizing patient feedback and patient reported outcomes to create PCC measures and assessment tools ensures care meets the needs and expectations of patients3,82–84 and aligns with global HIV expert recommendations. 6 We explore patient perspectives of PCC in another paper. 85 RWP facilities currently evaluate patient survey feedback regarding treatment and interaction with MCMs as part of quality management. 86 Further qualitative work specifically addressing barriers to implementation of PCC is also needed to improve our understanding and guide translation into practice. While our findings offer insight into provider perspectives of PCC, this work is exploratory in nature and quantitative data investigating ideal measures and outcomes is necessary, preferably in the context of a multilevel approach. Targets of PCC interventions focus mostly on gaps in the continuum of care including linkage, retention and viral suppression, 20 but these end outcomes do not capture important factors contributing to such gaps. Further quantitative and qualitative work exploring multilevel approaches, particularly addressing the system and community levels, would offer insight into optimal PCC frameworks for HIV care. It is now timelier than ever for PCC models to be adapted for HIV care settings given major leaps in efficiency and integration of healthcare systems afforded by investments in EMR and data sharing infrastructure. 3 As the HIV epidemic continues to evolve into a chronic condition, there is an increased need to look beyond ensuring universal access to ART to more longitudinal, patient-centered approaches focused on long-term quality of life. 6
Conclusion
HIV providers, in line with existing models, perceive the central tenets of PCC to include holistic, individualized care that is respectful of patient preferences and engages them as partners. Greater attention to creating environments of trust and security are necessary when implementing PCC in HIV care settings in particular to meet the unique needs of this population. We offer a multilevel HIV-adapted framework to guide conceptualization of PCC as a multilevel construct with practices at the individual, interpersonal and institutional level. Intervention and evaluation at all levels is key to adopting global calls for PCC as the new standard of care.
Footnotes
Acknowledgments
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. We also wish to gratefully acknowledge Cynthia Ibarra's assistance in coding and the support of Carla Valle-Schwenk, Ryan White Program Administrator, and the entire Ryan White Part A Program in the Miami-Dade County Office of Management and Budget, for their support in the study implementation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the National Institute on Minority Health & Health Disparities (NIMHD), National Institutes of Health under Award Number R01MD013563, and partially supported by NIMHD under Award Number U54MD012393.
Ethical Approval and Consent
The Florida International University Social Behavioral Institutional Review Board approved the study (#106958). Informed consent was obtained from each participant prior to participation.