
Abstract
Background
People living with human immune deficiency virus (PLHIV) grapple with distinct challenges, including HIV stigma which affects their antiretroviral therapy (ART) adherence self-efficacy. This study investigates the interaction of HIV stigma and perceived social support on ART adherence self-efficacy among adult PLHIV in South Africa.
Methods
This study utilized a cross-sectional design that involved 201 participants selected using time location sampling at a tertiary health facility in Durban.
Results
HIV stigma was significantly and negatively associated with self-efficacy (β = −7.860, t = −4.654, p = .001), with variations across different stigma levels (β = −5.844, t = −4.003, p = .001). Social support was significantly and positively associated with self-efficacy at lower HIV stigma levels (β = 7.440, t = 3.887, p = .001), in contrast to higher levels (β = −2.825, t = 1.400, p = .163).
Conclusion
Social support significantly influences ART adherence self-efficacy, particularly at lower levels of HIV stigma, but the effect of support weakens as stigma intensifies.
Plain Language Summary
The relationship between perceived social support and antiretroviral therapy adherence self-efficacy among adult PLHIV in South Africa: The influence of HIV stigma.
People living with HIV face unique challenges, such as HIV stigma, which impact their ability to adhere to antiretroviral therapy (ART). This study examined how HIV stigma and perceived social support affect the ART adherence self-efficacy of adults living with HIV in South Africa. This survey involved 201 participants who were selected by using time location sampling at a health facility in Durban, South Africa. The study found that HIV stigma had a significant and negative impact on self-efficacy (β = −7.860, t = −4.654, p = .001), with variations depending on the level of stigma (β = −5.844, t = −4.003, p = .001). On the other hand, social support had a significant and positive impact on self-efficacy at lower levels of HIV stigma (β = 7.440, t = 3.887, p = .001), but this effect weakened at higher levels of stigma (β = −2.825, t = 1.400, p = .163). Social support plays an important role in influencing self-efficacy, especially when HIV stigma is lower. However, the significant impact of social support diminishes as HIV stigma becomes more intense.
Background
Globally in 2022, the burden of the human immune deficiency virus (HIV) remained disproportionately high with an estimated 39.0 million people living with HIV (PLHIV) along with 1.3 million new infection cases that were reported. 1 The upsurge in the number of PLHIV was alarming in the Sub-Saharan Africa region, where about two-thirds of the global HIV burden (25.6 million) and slightly over half (51%) of new HIV infections (660,000) were recorded in this region. 1 In addition to these challenges South Africa with a population of 60.6 million encountered its own shortfalls by reporting approximately 7.6 million PLHIV in the year 2022, which translated into an HIV prevalence rate of 12.5%. 1 Nevertheless, it is worth noting the progress that was made in the management of the HIV pandemic in South Africa, as 75% of those living with HIV (5.7 million) were on antiretroviral therapy (ART) program, giving hope in the fight against HIV/AIDS. 1 Despite this substantial progress, the country still grapples with major obstacles related to managing the adverse outcomes of the HIV/AIDS pandemic. One of the major obstacles is the lack of efficacy translating to ART adherence. 11 The comprehensive approach is required in addressing these issues and it is therefore imperative to involve education and support for PLHIV to bolster their confidence in adhering to ART. 47
Self-efficacy, as proposed by Bandura in 1977, refers to the belief that one can succeed in any situation or task, influencing the outcome. 2 Specifically, ART adherence self-efficacy represents a person's belief in their ability to follow prescribed ART, 42 which is essential for achieving positive health outcomes and enabling individuals to take control of their own well-being. Numerous studies have explored self-efficacy in relation to ART adherence among individuals living with HIV.3-7 Researchers have delved into various factors influencing individuals’ self-efficacy in adhering to ART. The literature discusses factors such as social support, 5 coping, alcohol and drug use, 7 self-esteem, 9 HIV stigma, 8 and personal beliefs. 3 The debate within research revolves around how these factors can either positively or negatively impact ART adherence self-efficacy. While individual factors encompass personal beliefs, self-esteem, and attitudes toward ART, contextual factors include but are not limited to social support, HIV stigma, and other factors. However, there is still much to learn about how these factors interact to impact ART adherence self-efficacy.
Moreover, studies have highlighted a positive relationship between ART adherence self-efficacy and actual adherence behavior.6,10,45,46 For instance, a study conducted by Umar et al 46 in Malawi found that individuals with higher ART adherence self-efficacy were more likely to engage in adherence behaviors, given their stronger belief in their capability to execute necessary actions. This finding underscores the importance of enhancing self-efficacy beliefs through tailored interventions. However, much remains to be understood about how personal and contextual factors interact to impact ART adherence self-efficacy in South Africa. Particularly, the interplay between social support and HIV stigma within the South African context requires further exploration. As social support can play a critical role in improving ART adherence self-efficacy, this study hypothesizes that there is a positive relationship between perceived social support and ART adherence self-efficacy among adult PLHIV.
The importance of understanding how social support influences ART adherence among HIV/AIDS patients has been recognized by many researchers.12,13,16,18 Social support, which refers to the resources, assistance, and emotional connection that individuals receive from their social networks during times of stress, adversity, or need, plays a crucial role in this context.19-21 This support can take different forms, including instrumental support, which involves tangible aids or services; emotional support, providing empathy, understanding, and compassion; and informational support, offering advice, guidance, and relevant information.19,20 On the other hand, HIV stigma can be a major barrier to seeking and receiving social support, which can lead to feelings of low self-efficacy in individuals living with HIV. 15 HIV stigma refers to the negative attitudes, beliefs, and prejudices directed toward individuals living with HIV/AIDS. 22 It encompasses public, internalized, and enacted stigma, each contributing to the complex challenges faced by affected individuals.23,24 The HIV stigma significantly affects the mental health and overall well-being of PLHIV, leading to increased rates of low self-esteem, depression, anxiety, and isolation.17,25,40 The fear of rejection and discrimination can prevent them from seeking support, exacerbating their emotional distress. 26 Thus, stigmatizing attitudes and discriminatory behaviors toward PLHIV may exacerbate the negative effects of HIV, thereby impacting the mental health, self-esteem, and overall well-being of PLHIV. 25 Social identity theory provides a theoretical rationale for HIV stigma as a moderator by explaining how individuals’ identification with a stigmatized group affects their self-concept and emotional responses. 27
Moreover, the social cognitive theory posits that individuals’ beliefs about their capabilities to perform specific actions, 29 such as adhering to ART regimen effectively, are influenced by social support and external factors such as HIV stigma.18,28 HIV stigma can create a hostile environment that hampers the development of self-efficacy and positive self-concept among PLHIV, even in the presence of social support. 30 Several studies have explored the role of HIV stigma on various aspects of the lives of PLHIV.31,33,35,36 Among these studies, Shrestha et al 31 conducted research among 599 PLHIV in Nepal and identified HIV stigma (internalized) as a significant moderator impacting psychological outcomes (coping strategies, quality of life) and social outcomes (perceived social support) in this population. Another study by Li et al 32 in China found that HIV stigma partially mediated the relationship between self-efficacy and medication adherence, and fully mediated the relationship between self-efficacy and quality of life. Additionally, a study conducted in Thailand by Mireles et al 33 revealed a significant positive relationship between social support and ART adherence, indicating that higher levels of social support were associated with optimal levels of ART adherence. Moreover, this study also found a complex three-way interaction between depression, social support, and HIV-related stigma, which jointly influenced ART adherence among Thai participants.
Despite, numerous studies exploring the role of HIV stigma in affecting the overall well-being of PLHIV, 34 there is a notable lack of research investigating the complex interplay between HIV stigma, perceived social support and ART adherence self-efficacy. While Shrestha et al 31 emphasized the importance of HIV stigma as a moderator affecting psychological and social outcomes, but further investigation is necessary to understand the underlying pathways linking HIV stigma to social support and ART adherence self-efficacy. On the same hand, while Li et al 32 found evidence of HIV stigma as a mediator in the relationship between self-efficacy and ART adherence and quality of life, there remains a dearth of research in understanding the mechanisms through which HIV stigma and social support interact to influence ART adherence self-efficacy. Therefore, in light of the preceding discussion, this study hypothesizes that the positive relationship between perceived social support and ART adherence self-efficacy will be negatively moderated by HIV stigma among adult PLHIV.
Additionally, Mireles et al 33 found that the influence of depression on ART adherence was moderated by both social support and HIV stigma. These results warrant further investigation into how the influence of social support on ART adherence self-efficacy depends on the levels of HIV stigma. In the context of the current study, HIV stigma acts as a potential moderator, that weakens the positive influence of social support on ART adherence self-efficacy. Addressing HIV stigma becomes crucial to ensure that social support fully serves its potential role in enhancing self-efficacy and improving the overall well-being of PLHIV. On the other hand, very few studies that have examined the direct or indirect impact of social support on ART adherence self-efficacy. 15 For instance, a study by Tao et al 15 found a positive correlation between greater social support and high levels of ART adherence self-efficacy. Additionally, social support was found to play an indirect role in influencing ART adherence in some studies. For example, Mi et al 14 in China reported that social support acted as a significant mediator in the relationship between family disclosure and ART adherence. Similarly, a recent study by Tao et al 15 revealed a significant indirect effect of HIV-related stigma on HIV self-management through social support. These results suggest that social support can act as a mediator, serving as a protective factor for ART adherence self-efficacy and actual ART adherence. Indeed, existing research shows that social support predicts ART adherence among PLHIV.12,13,16 However, there is dearth of studies that investigate the direct impact of social support on ART adherence self-efficacy and how the relationship between these variables may be influenced by the levels of HIV stigma among adult PLHIV in South Africa. Therefore, this study further posits that the positive relationship between perceived social support and ART adherence self-efficacy among adult PLHIV will vary based on different levels of HIV stigma.
Methods
Study Design, Population, and Sampling
Utilizing a cross-sectional quantitative research design, this study was grounded in the postpositivistic paradigm, acknowledging the significance of social context in knowledge construction. According to this paradigm, knowledge is shaped through human interactions within their surroundings.
The study utilized a nonprobability time location sampling (TLS) method to recruit participants from an antiretroviral (ARV) clinic situated in a tertiary hospital in Durban, KwaZulu-Natal. The TLS is a valuable method for gathering data on hard-to-reach populations, such as men who have sex with men 58 and PLHIV. This method involves selecting specific locations where individuals of interest can be found and then sampling those who attend these locations during predetermined time intervals.58,59 Therefore, TLS was a practical choice with the aim to access populations with diverse and dynamic characteristics given that the data collection occurred during the coronavirus (COVID-19)-led lockdown. This approach allowed for the inclusion of individuals who may not be adequately represented in the conventional sampling frames, thereby improving the external validity of the study. 58 While probabilistic methods are generally preferred for their randomness and potential to produce representative samples, the nonrandom TLS was implemented to address pitfalls related to sample representation, inclusivity, and accessibility. 58 The determination of location was established upon the principle of “social viability,” 59 which ensures the presence of a satisfactory number of individuals from the target population at the designated venue, and provides insights into the optimal time periods for engaging with this population.
The first step involved determining a key location, which was a tertiary health facility in Durban, for participant recruitment process. The second step focused on sampling periods that were strategically chosen to collect comprehensive and diverse data, given different time slots designated on selected days of the week. For instance, the data collection process involved the allocation of specific time intervals onto four weekdays, considering the operating hours of the health facility. However, the allocation was done randomly, resulting in the following intervals: Mondays (13:00 h-15 00), Tuesdays (09:00-11:00), Wednesdays (11:00-13:00), and Thursdays (07:00-9:00). During these time intervals, potential participants were approached and selected nonrandomly with a purpose to reach individuals who may not be sufficiently represented in traditional sampling frames. This approach helpe d to improve external validity, maximize access to marginalized and stigmatized groups, 59 and reach the target number of participants. This approach also allowed us to gather a variety of responses from participants residing in different urban communities in Durban. Eligible participants meeting the inclusion criteria were selected voluntarily and encompassed PLHIV aged 18 years or older, enrolled in an ART program, and residing in suburban and township communities of Durban, South Africa. Data collection took place between June and October 2020, coinciding with the COVID-19 pandemic in South Africa.
Sample Size Determination
The determination of the sample size took a careful consideration of both financial resources and statistical reliability while ensuring the feasibility of the study. To determine the minimum required sample size, the researchers applied the formula proposed by Lemeshow et al
48
this formula is well-regarded for its ability to ensure the balance between cost-effectiveness and the reliability of statistical inferences.
The missing data is of utmost importance when determining the sample size as it has a direct influence on the statistical power and validity of the findings. 49 To ensure the reliability and accuracy of the results, a standard of 50% was used to determine the acceptability of missing data that has occurred either at completely random, random, or nonrandom. 49 For instance, the number of 222 subjects participated in the study, exceeding the estimated minimum required sample size of 189 subjects. However, 21 subjects were excluded from the analysis due to the presence of incomplete data in their questionnaires, surpassing the permissible threshold of less than 50% missing data. 49
Data Collection Methods
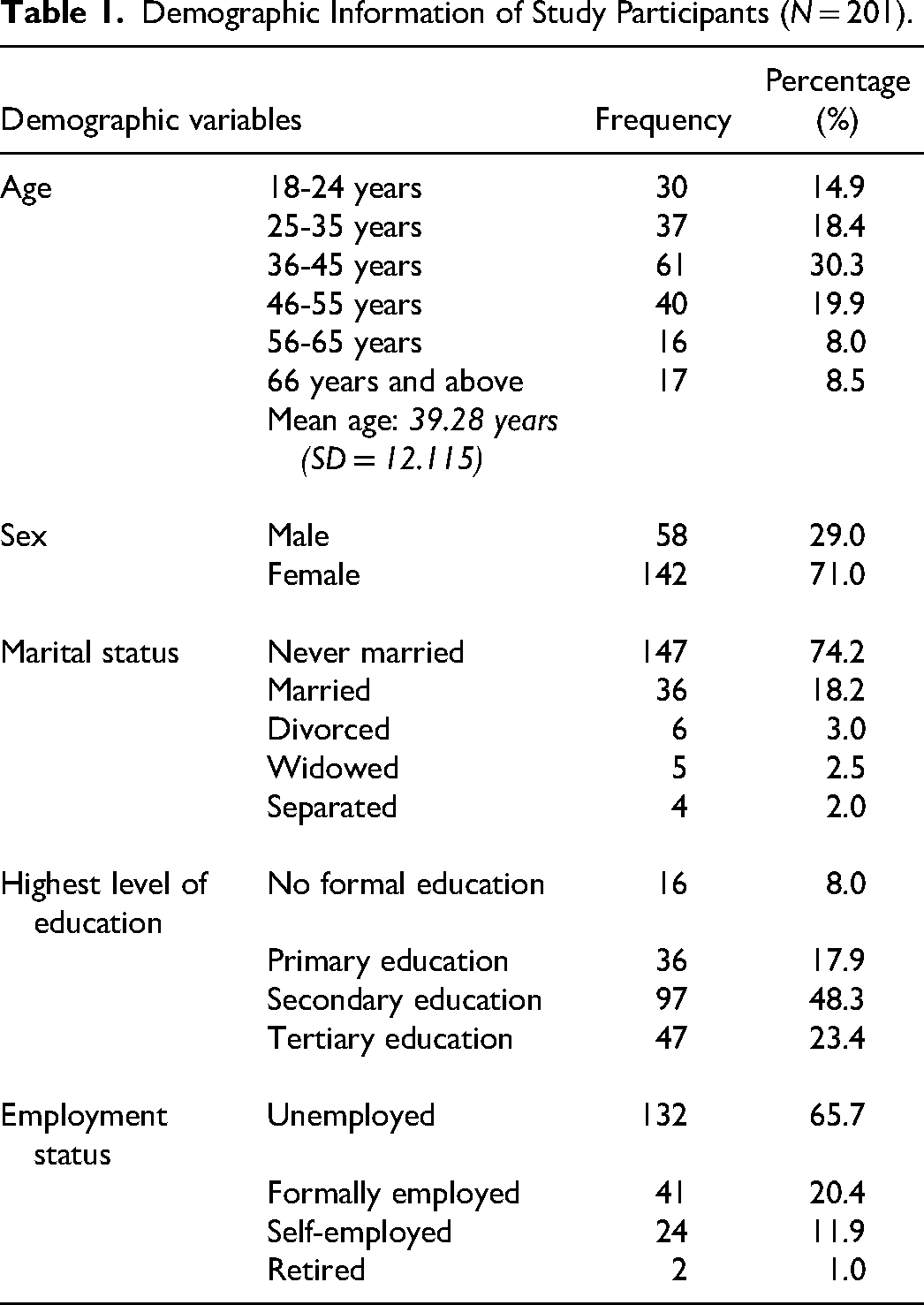
As an integral component of the survey questionnaire, essential sociodemographic information was gathered (Table 1). To ensure unbiased translation, the nominated language experts underwent a blind translation process, where both questionnaire and informed consent were translated into IsiZulu from English and then translate back from Zulu to English. Before engaging in the survey, all participants who volunteered their involvement in the study provided a written consent. The questionnaire itself required approximately 25 minutes to complete.
Demographic Information of Study Participants (N = 201).
Measures
HIV-Stigma: Short Version of HIV Stigma Scale
The Short Version of the HIV stigma scale (HSS-12) was employed in this study to evaluate the presence of HIV stigma, comprising four distinct subscales: internalized stigma (consisting of three items), disclosure concerns (with three items), concerns about public attitudes (also with three items), and negative self-image (comprising three items). 43 Each subscale item exemplifies different aspects of HIV stigma. For instance, an item representing internalized stigma is, “People I care about stopped calling after learning I have HIV,” while a disclosure concerns item is phrased as “I work hard to keep my HIV a secret.” Additionally, concerns about public attitudes are reflected in an item stating, “People with HIV are treated like outcasts,” and negative self-image is represented by the item “I feel I'm not a good person as others because I have HIV.”
Participants responded to these items on a 4-point Likert scale, ranging from 1 (strongly disagree) to 4 (strongly agree). 43 The total score range for each subscale of the HSS-12 is 3 to 12, with scoring determined by summing the ratings of the individual items of each subscale. 43 Additionally, individual scores were added together across all subscales to obtain the total HSS-12 score for each participant. Afterward, the median score for the total HSS-12 scores across the entire group of participants was calculated. The possible scores for the overall HSS-12 ranged from 12 to 48. The median score was used to perform a median split on the total HSS-12 scores. Therefore, participants with scores higher than the median were classified as having experienced high levels of HIV stigma, while those with scores lower than the median were identified as having experienced low levels of HIV stigma. Previous studies have shown a good to excellent internal consistency for the HSS-12, with Cronbach's alpha coefficients ranging from .75 to .96.43,51-54 In the context of the present study, the internal reliability for the HSS-12 was established, showing Cronbach's alpha coefficients of .87 which indicates an excellent internal consistency.
Social Support: The Multidimensional Scale of Perceived Social Support
The Multidimensional Scale of Perceived Social Support (MSPSS-12) was employed as an instrument to assess the perceived social support, comprising 12 self-report items. The MSPSS segregates these items into three distinct factor groups, corresponding to the sources of perceived social support: family (four items), friends (four items), and significant others (four items). 44 Respondents rated their agreement with each item on a 7-point Likert scale, ranging from 1 (very strongly disagree) to 7 (very strongly agree), where higher scores across all dimensions signified greater levels of perceived social support. The MSPSS-12 has demonstrated excellent internal consistency, with reported overall Cronbach's alpha coefficients ranging from .80 to .95.44,55,56 In the current study, Cronbach's alpha coefficient was calculated to be .85, indicating a high level of internal consistency.
ART Adherence Self-Efficacy: HIV Adherence Self-Efficacy Scale
The assessment of ART adherence self-efficacy was carried out using the HIV adherence self-efficacy (HIV-ASES-12) scale, comprising 12 self-report items. 42 These items are measured on a 4-point Likert scale, ranging from 0 (indicating no confidence) to 3 (representing complete confidence), with higher scores denoting high levels of ART adherence self-efficacy. Johnson et al 42 originally demonstrated the scale's strong internal reliability by reporting a robust coefficient of .90. In the present study, our analysis yielded a slightly lower but still favorable Cronbach's alpha of .88. An illustrative item from the HIV-ASES scale reads as follows: “How confident have you been in the past month that you can adhere to your treatment plan even when side effects begin to interfere with daily activities?.” 42 Respondents had to select one of the four response options for an individual item: 0 (not at all confident), 1 (moderately confident), 2 (confident), or 3 (totally confident) based on their level of self-efficacy in handling these specific situations. 42
Statistical Analyses
A normality test was conducted for all continuous variables, while frequencies and percentages were reported for categorical variables. The association between HIV stigma, perceived social support, and ART adherence self-efficacy was examined using the Pearson correlation test. Furthermore, tolerance and variance inflation factor (VIF) 57 tests were performed to identify any collinearity issues among predictor variables. The VIF values were all less than 5, indicating less issues of multicollinearity among predictor variables which was indicative of no further corrective measures needed to be applied (Perceived Social Support, Tolerance = .701, VIF = 1.426; HIV stigma, Tolerance = .546, VIF = 1.830; HIV Stigma × Perceived Social Support, Tolerance = .731, VIF = 1.368). The simultaneous multiple regression was performed, and moderation analysis was conducted using Statistical Package for the Social Sciences (SPSS) Version 27 to test the moderation effect of HIV stigma on perceived social support and ART adherence self-efficacy. A significance level of p < .05 was used to determine statistical significance.
Ethical Approval and Informed Consent
Ethical clearance was obtained from the Institutional review board of the University of KwaZulu-Natal (approval number: HSSREC/00000607/2019). A formal support letter was produced and sent to the designated health facility namely King Edward VIII tertiary Hospital. All patients provided written informed consent prior to their enrollment in the study. The consent included a brief description of the study, the use of the information to be collected, benefits and risks associated with participation, and the confidentiality and handling of the gathered data. The consent form was carefully composed using plain and easily understandable language to ensure that participants fully comprehended its contents. Furthermore, the rights of the participants were duly respected throughout the entire duration of the study.
Results
Table 1 depicts the sociodemographic characteristics of the study participants. The study sample was predominanted by females, consisting of (71.0%, n = 142), with a mean age of 39.28 years (SD = 12.115). Most of the study participants had never been married (74.2%, n = 147), and a significant proportion had completed secondary school education (48.3%, n = 97). Pertaining to the employment status about two-thirds of the sample (65.7%, n = 132) reported being unemployed (Table 1).
The Person's Correlation analysis supported the first hypothesis, revealing a significant and positive correlation between perceived social support and ART adherence self-efficacy (r = .267, p < .01). On the other hand, a significant and negative correlation was found between HIV stigma and ART adherence self-efficacy (r = −.315, p < .01). Moreover, perceived social support and HIV stigma demonstrated a significant and negative association (r = −0.545, p < .01) (Table 2).
The estimates from Table 3 show the results of the full regression model, examining the main effects and interaction between HIV stigma and perceived social support on ART adherence self-efficacy. The perceived social support did not show a significant association with ART adherence self-efficacy (β = 2.307, t = 1.54, p = .123), whereas HIV stigma was significantly associated with ART adherence self-efficacy (β = −7.860, t = −4.654, p = .001). Interestingly, the interaction term (HIV Stigma × perceived social support) indicated that the relationship between perceived social support and ART adherence self-efficacy varied by levels of HIV stigma (β = −5.844, t = −4.003, p = .001).
In Table 3, we further examined the association between perceived social support and ART adherence self-efficacy based on conditions of HIV stigma using estimated simple slope models and the theoretical moderation model shown in Figure 1. The results revealed a significant relationship between perceived social support and ART adherence self-efficacy at lower levels of HIV stigma (β = 7.440, t = 3.887, p = .001). However, at high levels of HIV stigma, perceived social support was not significantly influencing ART adherence self-efficacy (β = −2.825, t = 1.400, p = .163). The test for differences between the simple slopes confirmed a statistically significant difference (t = 3.692, p = .001).
To visualize these findings, Figure 2 presents the plotted simple slopes graph, regressing ART adherence self-efficacy on perceived social support at high (+1SD) and low (−1SD) levels of HIV stigma. The graph clearly illustrates that the positive relationship between perceived social support and ART adherence self-efficacy was stronger at lower levels of HIV stigma compared to higher levels, with the slope of the relationship for low HIV stigma being greater than for high HIV stigma.
In summary, the analysis of the interaction term and the test for differences in the simple slopes both indicated statistical significance, highlighting the moderating role of HIV stigma on the relationship between perceived social support and ART adherence self-efficacy.
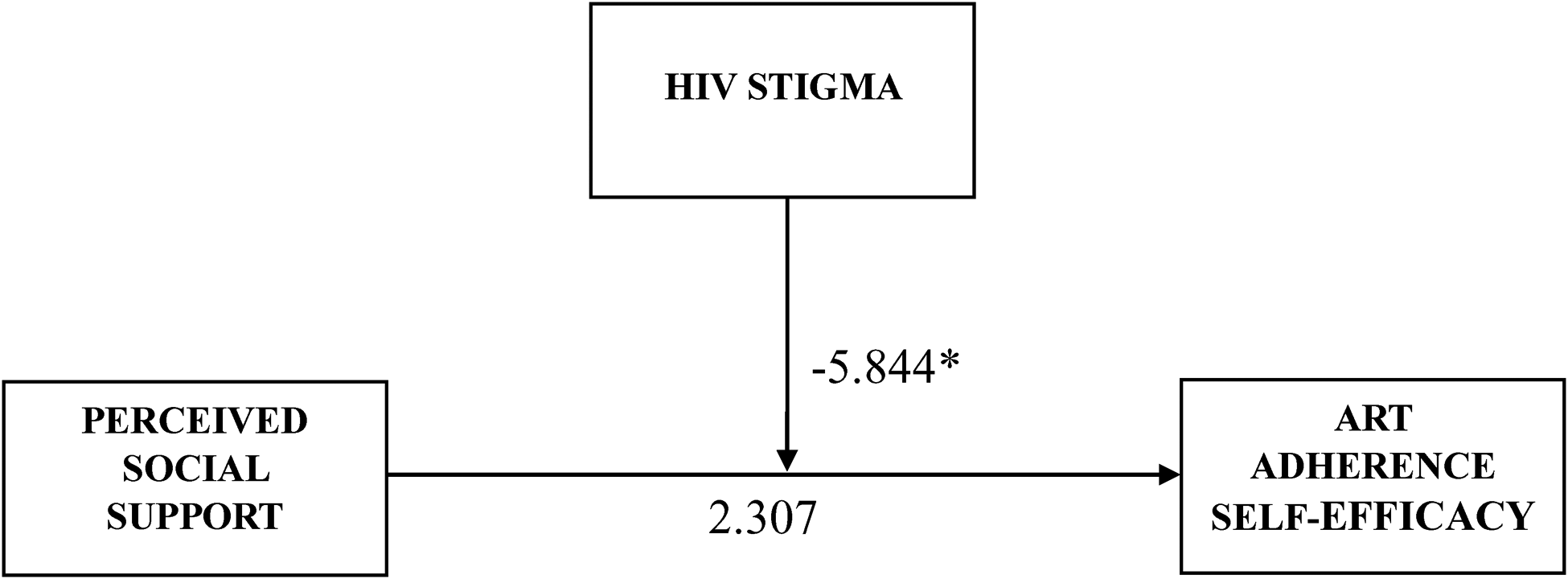
The specific paths of the association between perceived social support, ART adherence self-efficacy, and moderating effect. *p < .05.
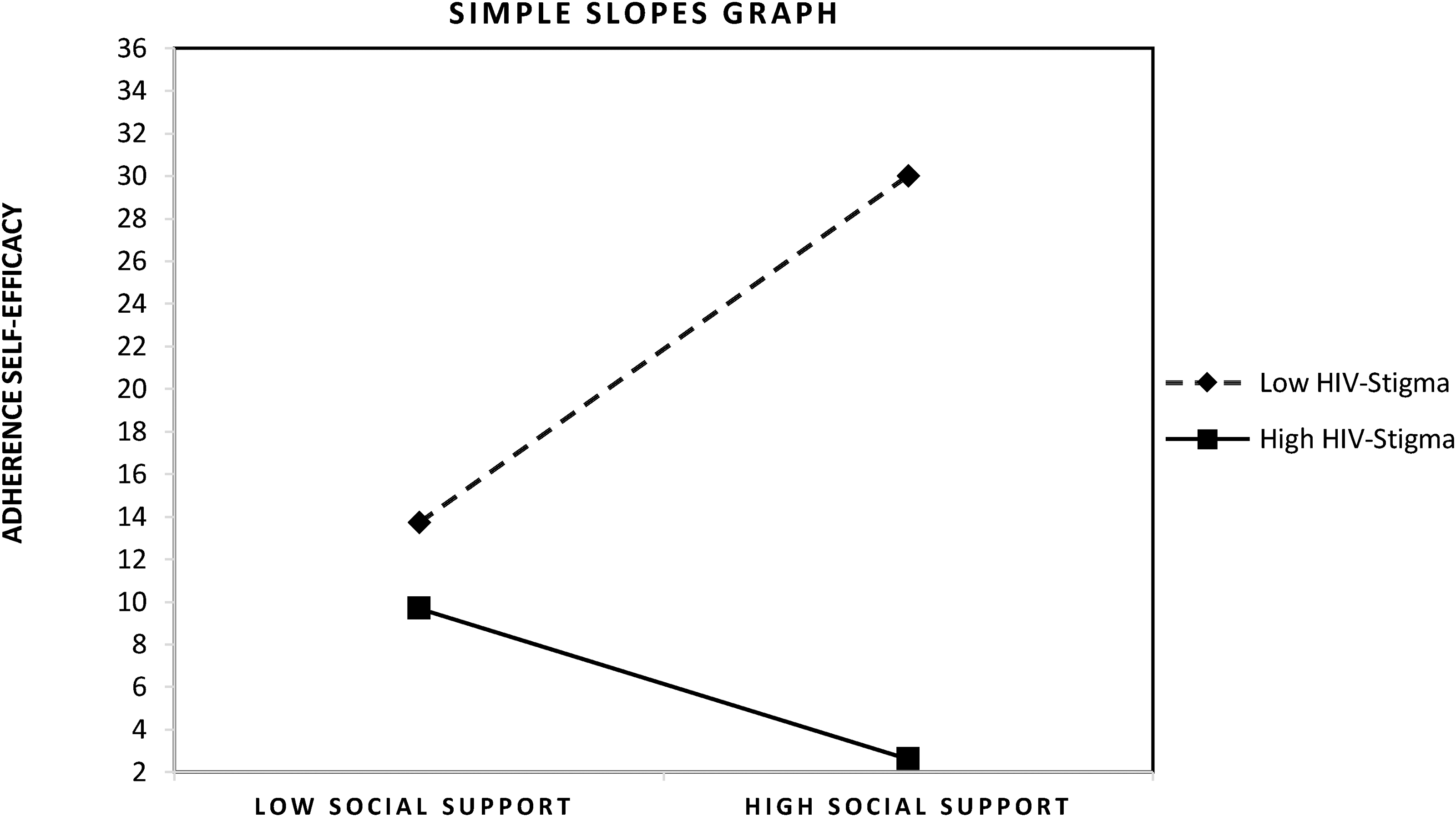
Simple slopes plot graph.
Correlations among Central Study Variables.
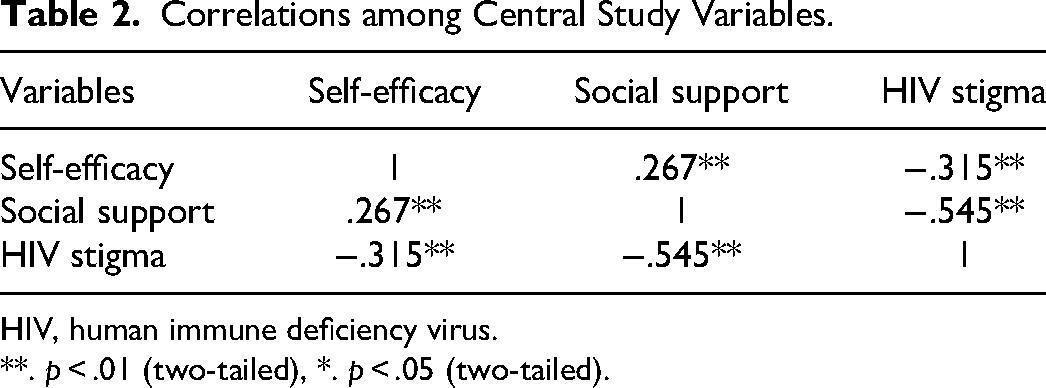
HIV, human immune deficiency virus.
**. p < .01 (two-tailed), *. p < .05 (two-tailed).
Full Regression and Simple Slopes Models of HIV Stigma, Perceived Social Support, and ART Adherence Self-Efficacy.
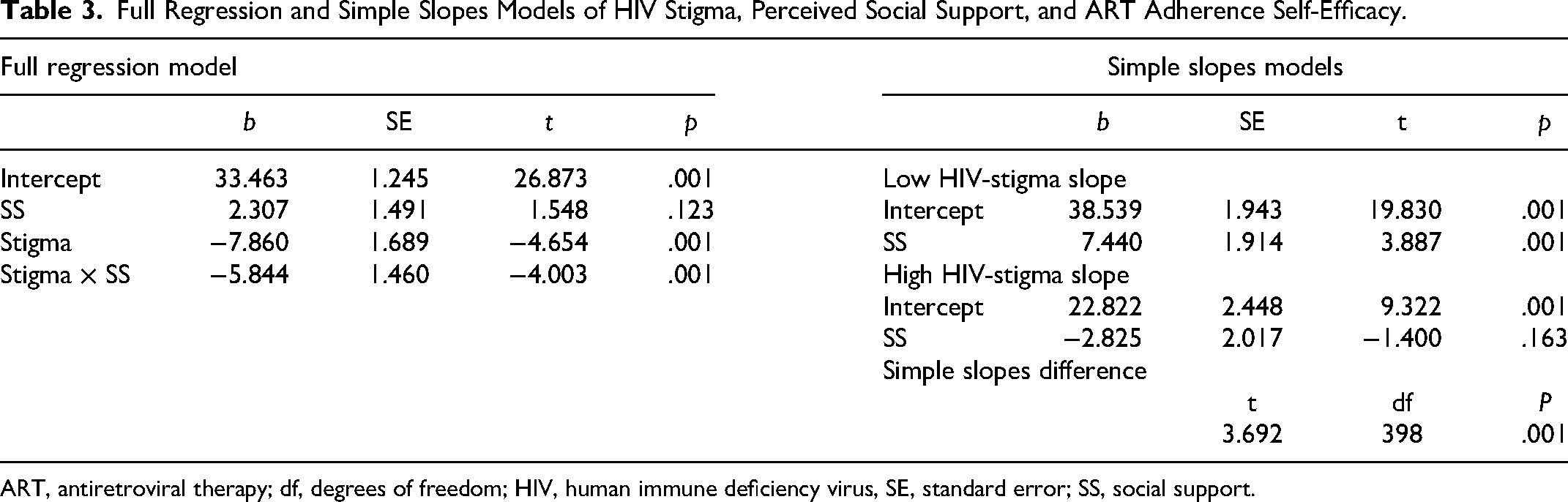
ART, antiretroviral therapy; df, degrees of freedom; HIV, human immune deficiency virus, SE, standard error; SS, social support.
Discussion
This study aimed to investigate the relationship between perceived social support and ART adherence self-efficacy and to determine whether this relationship is moderated by HIV stigma among adult PLHIV. The results from this study highlight the relationship between perceived social support, ART adherence self-efficacy, and the moderating role of HIV stigma.
The bivariate results revealed the significant relationships between perceived social support, ART adherence self-efficacy, and HIV stigma. The perceived social support was positively correlated with ART adherence self-efficacy, supporting our first hypothesis. This result suggests that individuals with higher perceived social support also had greater confidence in adhering to their ART and this finding aligns with the results found by Tao et al 15 and Wang et al 39 among PLHIV in China. On the other hand, HIV stigma was found to be negatively correlated with ART adherence self-efficacy. This result suggests that individuals with higher levels of HIV stigma tend to have lower ART adherence self-efficacy. This result was in line with that of Kamitani et al 37 among Asian PLHIV in California and Wang et al 39 among Chinese PLHIV. Additionally, perceived social support was found to be negatively correlated with HIV stigma. This result was suggestive of that individuals with higher perceived social support would tend to have lower levels of HIV stigma. This result was consistent with the recent study by Wang et al 39 conducted across three provinces in China. These findings provided a foundational understanding of the interplay between perceived social support, HIV stigma, and ART adherence self-efficacy among adult PLHIV.
The results from the full regression model confirmed the moderating role of HIV stigma on the relationship between perceived social support and ART adherence self-efficacy and this was also supportive of our second hypothesis. Additionally, the multiple regression model displayed a negative direct effect of HIV stigma on ART adherence self-efficacy which also implied that higher levels of HIV stigma were associated with lower ART adherence self-efficacy levels. This result was consistent with the previous works that highlight the adverse effect of HIV stigma on various facets of HIV care for PLHIV.30,31,38,39,41 The profound understanding of the influence of HIV stigma on an individual's confidence to adhere to ART is crucial, essentially for the formulation of interventions that aim to improve adherence behaviors and overall well-being of PLHIV. It is also noteworthy that this study is the first to our knowledge to investigate the role of HIV stigma as a moderator of the relationship between perceived social support and ART adherence self-efficacy among adult PLHIV in South Africa.
The study also hypothesized that the positive influence of perceived social support on ART adherence self-efficacy varies with different levels of HIV stigma among adult PLHIV. The results from the simple slope models confirmed this hypothesis, given that at lower levels of HIV stigma, ART adherence self-efficacy was influenced significantly by perceived social support. This result suggests that social support may become crucial, essentially in situations where individuals are experiencing less HIV stigma. On the contrary, the simple slope model indicated that at higher HIV stigma levels, ART adherence self-efficacy was not significantly influenced by perceived social support. This finding suggests that HIV stigma overshadows the key role of social support in fostering ART adherence self-efficacy among adult PLHIV. These results contrast with that of the study done by Wang et al 39 where they found that perceived social support had a significant impact on depression when HIV stigma was high, suggesting that different populations may respond differently on the basis of their perceptions of social support. Therefore, our results have shed light on how HIV stigma moderates the relationship between perceived social support and ART adherence self-efficacy, and this underscores the need to address a stigma related to HIV to improve confidence and adherence behaviors of PLHIV.
These results have significant implications for interventions targeting HIV stigma, social support, and ART adherence self-efficacy among adult PLHIV. Healthcare providers and support organizations should recognize the complexity of adherence behaviors and consider both social support and HIV stigma when developing interventions. The development of HIV stigma reduction strategies and interventions aimed at enhancing social support networks are essential for an effective improvement of ART adherence self-efficacy and treatment outcomes of PLHIV. Future research should build upon these results and address the key limitations highlighted by this study to advance our understanding of this complex interplay between HIV stigma, perceived social support, and ART adherence self-efficacy.
Limitations
This study makes a significant contribution by examining the interplay between HIV stigma, perceived social support, and ART adherence self-efficacy. However, several limitations warrant a cautious interpretation of the results. Firstly, a cross-sectional design of the study hinders the establishment of causal relationships between the variables under investigation. While significant associations are observed, definitive cause-and-effect conclusions cannot be drawn. Secondly, the reliance on self-reported measures introduces subjectivity to the study, emanating from social desirability, social norms, and recall bias which significantly and collectively contribute to the lack of internal validity. Thirdly, the use of nonprobability time location sampling may limit external validity by excluding individuals with immediate challenges associated with ART adherence provided that the study recruited participants from those attending follow-up appointments for HIV treatment. These limitations underscore the need to interpret the results with care and emphasize the necessity of future research using longitudinal designs to explore temporal dynamics of adherence behaviour.
Despite the limitations, this study paves the way for future investigations by highlighting HIV stigma as a potential psychosocial mechanism underlying the relationship between perceived social support and ART adherence self-efficacy. Thus, researchers can expand their understanding of this intricate relationship by building on these insights. Future studies should explore additional confounding variables, such as sociodemographic factors, cultural variations, and mental health aspects, that might have an influence between perceived social support and ART adherence self-efficacy. Longitudinal designs would be instrumental in untangling the temporal complexities and potential causal links among these variables. Thus, this study serves as a stepping stone in the ongoing quest to comprehend the multifaceted experiences of PLHIV and informs the need for comprehensive and rigorous research to address the complexities of their lives.
Conclusions
This study provided valuable insights into the psychosocial dynamics experienced by adult PLHIV. The results revealed a positive relationship between perceived social support and ART adherence self-efficacy. Higher levels of perceived social support were significantly associated with higher ART adherence self-efficacy in this population. In addition, HIV stigma moderated the relationship between perceived social support and ART adherence self-efficacy. This result suggested that the impact of perceived social support on ART adherence self-efficacy was influenced by the levels of HIV stigma experienced by PLHIV. Notably, at lower levels of HIV stigma, perceived social support demonstrated a stronger positive association with ART adherence self-efficacy compared to higher levels. These findings underscore the importance of tailored interventions addressing HIV stigma and enhancing social support to improve ART adherence self-efficacy and overall well-being for PLHIV in South Africa.
Footnotes
Acknowledgments
Our heartfelt thanks go to the adult patients at Philani ARV Clinic, King Edward VIII Tertiary Hospital, for their invaluable participation. Gratitude also to King Edward VIII Tertiary Hospital and KwaZulu-Natal Department of Health for their unwavering support.
Authors’ Contributions
M.Q.L contributed to study conception, design, data acquisition, analysis, manuscript drafting, and refinement of the final manuscript. J.J.L contributed to study conception, design, data interpretation, manuscript review, and refinement of the final manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Research Foundation (Grant No. MND190703452772).