
Abstract
This study sought to examine the role of providers as health discussants (HD) on interest in preexposure prophylaxis for HIV prevention in a national sample of adult Black cisgender women (N = 315). Health discussant networks, a type of social network, may be influential in HIV prevention efforts. These networks, often composed of individuals’ families, have improved health utilization outcomes in other disciplines. However, health discussants in HIV prevention are understudied, especially when considering providers as network members. We conducted a cross-sectional online survey and collected socio-demographic information, sexual history, HIV concerns, PrEP attitudes, healthcare utilization, mistrust, social support, and HD information. We used descriptive statistics and logistic regression to analyze data. Associations between PrEP interest and variables were examined. We found that older, partnered, who had recent healthcare visits or health insurance were more likely to involve healthcare providers as discussants. Anticipated PrEP stigma decreased provider involvement. Among participants listing providers as discussants, there was a greater likelihood of interest in using PrEP. Our findings indicate that healthcare provider support and social factors are crucial in promoting PrEP engagement among Black women. Integrating social dynamics and positive provider-patient interactions is essential for successful PrEP implementation.
Keywords
Introduction
Health discussion networks (HDN) are a subset of a person's larger social network and can potentially affect HIV prevention behaviors among Black women in the US. HDN relies on social regulation, which is the normative influence of social networks on a person's decision-making process that determines their health behaviors and attitudes. 1 Therefore, health discussants (HD), members of HDN, have the potential to influence attitudes towards healthcare, offer guidance on accessing services, and facilitate service utilization by facilitating initial contact with the treatment system.1-4 Health discussants who have a favorable attitude towards healthcare, are close in relationship with one another, provide social support, and are perceived as knowledgeable about healthcare are most likely to influence healthcare utilization.2,4 While extensively examined in aging and palliative care research, little is known about health discussant networks in HIV prevention.
Health discussant networks have been explored extensively in medical social support research.1,2,4 Evidence shows that family members are often the most reported HD within personal networks, while providers or medical professionals are less likely to be identified as health discussants.5,6 The lack of providers as HD may be further exacerbated around sexual health topics or issues. Evidence shows that primary care providers frequently fail to inquire about and address an individual's sexual health, hoping to avoid “opening a can of worms.”7-10 However, when initiated by the patient, primary care providers tend to address topics around contraception and sexually transmitted infections (STIs). Findings from a 2020 survey show that less than one-third of women of reproductive age say they were asked by a provider about HIV or another STI (26% and 28%, respectively). 11 These data reflect the need to improve sexual health communication among primary care providers and women broadly, specifically Black women who are at increased risk of HIV acquisition.
Most social network and HIV prevention studies use data collected about personal social networks broadly, as opposed to health discussant networks. Personal network data are collected using name generator questions such as, with whom do you discuss important matters? Or with whom have you communicated with recently? Personal network data has been found to be predictive of interest in preexposure prophylaxis (PrEP) for HIV prevention use among women.12-15 PrEP is a biomedical HIV prevention strategy that has the potential to reduce rates of HIV infection. Women comprise 20% of new HIV infections in the U.S., but only 4.7% are prescribed PrEP. Black cisgender women comprise 13% of the female population, but HIV infection among this group accounted for 54% of diagnoses, and in 2021, the rate of HIV diagnoses among Black women was 10.8 times the rate among White females. PrEP scale-up at the provider level is necessary in order to reduce these HIV-related racial disparities. According to the 2021 CDC Guidelines, providers are strongly encouraged to speak to all sexually active adults about PrEP. 16 This is particularly salient because previous studies have demonstrated that HIV risk assessments and the 2019 PrEP eligibility guidelines have failed to properly capture the sexual behaviors that increase HIV vulnerability. 17 Provider and patient communication is integral to PrEP interest as previous studies have shown that Black women are comfortable speaking to their providers about PrEP if given the opportunity. 18 This study seeks to describe the health discussant networks of a sample of sexually active adult Black women and identify the factors associated with providers as health discussants, including interest in oral PrEP for HIV prevention.
Methods
Study Population
We conducted a cross-sectional online, self-administered survey using the Qualtrics online platform (Qualtrics, Provo, UT). Eligible women included self-identified Black/African American cisgender women aged 18 to 44 years, with no prior HIV diagnosis, who had sexual intercourse with a male partner 12 months before survey administration. Sampling and survey design methods have been described and referenced in the previous publication.18
Key Measures
The survey included self-reported sociodemographic information, including age, relationship status, education level, and household income. Sexual history was assessed by asking respondents about consistent condom use and history of STIs. One item assessed worry about acquiring HIV infection. Healthcare utilization was assessed by asking respondents about insurance status and barriers to care. We asked respondents their level of agreement with whether they had been personally treated poorly or unfairly by doctors or healthcare workers due to their race. Perceived social support was assessed using the Women's Social Support Scale. 19 PrEP education was provided via a brief statement defining PrEP and an infographic describing the FDA approval and efficacy of oral PrEP for women. We assessed interest in PrEP by asking, “Would you be interested in taking PrEP for HIV prevention? [yes/no]”. PrEP stigma was assessed via two subscales from the PrEP anticipated stigma scale. 20 PrEP subjective norms were assessed via an adapted measure from the AIDS Preventative Behavior subjective norms scales to focus specifically on PrEP. 21
HD members were listed in response to a prompt stating, “From time to time, most people discuss important matters with other people. Think about all the people in your life with whom you have discussed your health. How many people do you discuss your health with?” Participants could select a number up to 10. Participants were then asked to list the individual's initials and answer questions about each person listed, including the nature of their relationship (eg, family, friend, partner, co-worker, health care provider). In addition to listing individuals as part of their HDNs, each individual respondent reported the frequency of communication and rated the importance of each individual's opinions.
PrEP support was assessed by asking respondents their level of agreement with the following statements for each person in their HDN: “This person would be supportive if you used PrEP to prevent HIV infection; This person would go with you to get PrEP; You feel comfortable discussing PrEP for HIV prevention with this person; This person would react positively towards me if I mentioned PrEthatP for HIV prevention.”
Statistical Analyses
Descriptive statistics and logistic regression were used to characterize the study population (N = 315) and a subsample of participants who listed a healthcare provider as an HD (n = 194). Unadjusted logistic regression was used to compare participants who listed a provider as an HD to those who did not. We examined the following variables: sociodemographic characteristics, sexual history, worry about acquiring HIV, PrEP disapproval score, PrEP-user stereotypes score, PrEP subjective norms score, perceived social support score, health care utilization, and medical mistrust.
Among participants who listed a provider as an HD, unadjusted logistic regression was used to compare participants who were interested in PrEP to those who were not interested in PrEP. We stepped the above-listed variables and the three HD variables into six hierarchical logistic regression models. If participants listed multiple providers, the maximum communication frequency, opinion importance, and PrEP support score were used for analysis.
Ethical Approval and Informed Consent
All procedures performed in this study were in accordance with the ethical standards of the Institutional Review Board at Washington University in St. Louis, Missouri and with the 1964 Helsinki Declaration and its later amendments. Informed consent was obtained from all individual participants included in the study.
Results
Our sample included a national sample of 315 Black cisgender women. Descriptive characteristics are presented in Table 1. The median age was 29 years (IQR = 22-35). The geographic distribution of respondents was similar to that of Black Americans across the U.S.; most respondents (55.2%) resided in the South at the time of survey administration. Most respondents had at least some college education (50.5%), were employed (78.1.%), and had health insurance (88.6%), and 34.6% had an annual income of $40,000 or higher. In the past 12 months, 88.3% had visited a healthcare provider and 26.3% did not receive healthcare because of concerns about cost. More than half of respondents (52.7%) were in a relationship and 12.4% reported both inconsistent or no condom use and 2 or more sexual partnerships. Overall, more than half (57.8%) reported being worried about acquiring HIV infection. The subsample of participants who listed a provider as an HD is described in Table 2.
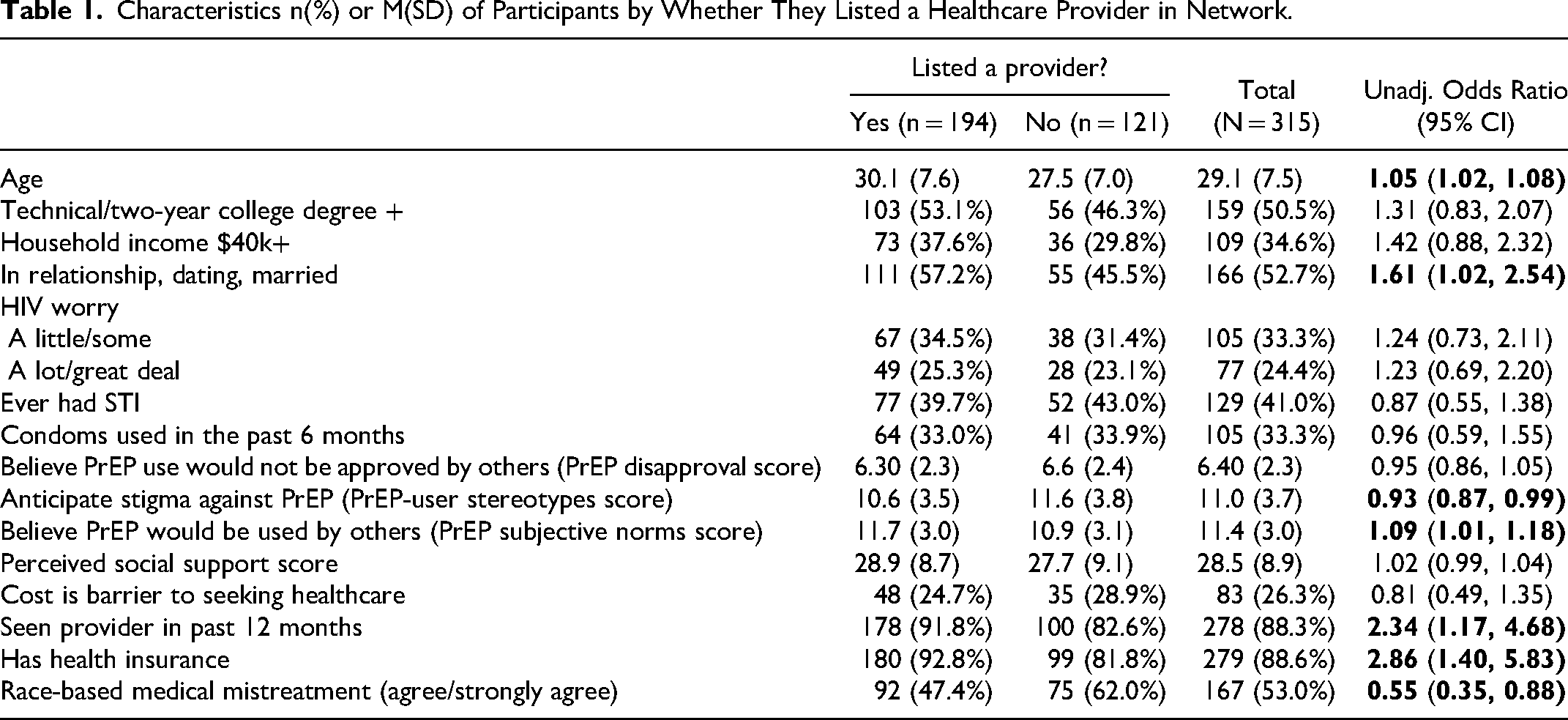
Characteristics n(%) or M(SD) of Participants by Whether They Listed a Healthcare Provider in Network.
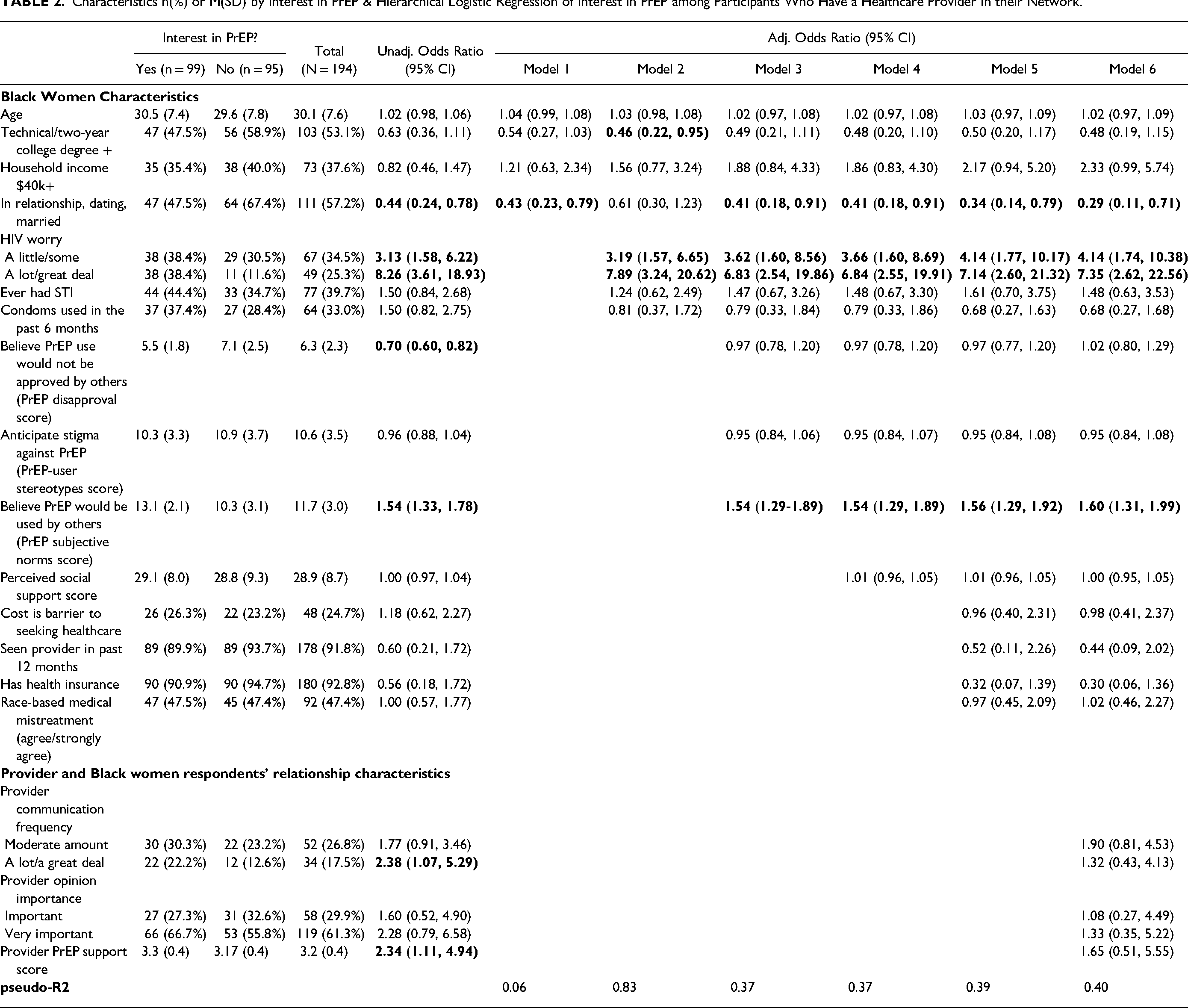
Characteristics n(%) or M(SD) by Interest in PrEP & Hierarchical Logistic Regression of Interest in PrEP among Participants Who Have a Healthcare Provider in their Network.
Provider as Health Discussant
According to unadjusted odds ratios (OR) and confidence intervals (CI), participants who are older (OR = 1.05; CI = 1.02, 1.08), believe PrEP would be used or accepted by others (ie, higher PrEP subjective norms scores; OR = 1.09; CI = 1.01, 1.18), have seen a provider in the past 12 months (OR = 2.34; CI = 1.17, 4.68), or have health insurance (OR = 2.86; CI = 1.40, 5.83) are more likely to list a provider as a discussant. However, participants who anticipate stigma against PrEP use based on cultural associations (ie, higher PrEP stereotypes score; OR = 0.93; CI = 0.87, 0.99) or have been treated poorly or unfairly by healthcare professionals based on their race (OR = 0.55; CI = 0.35, 0.88) are less likely to list a provider as a discussant (Table 1).
Interest in PrEP Among Participants Who List their Provider as Health Discussant
According to unadjusted ORs, interest in PrEP is significantly associated with the following variables: relationship status (OR = 0.44; CI = 0.24, 0.78), worry about acquiring HIV a little/some and a lot/great deal (ORs = 3.13 and 8.26; CIs = 1.58, 6.22 and 3.61, 18.93), PrEP disapproval score (OR = 0.70; CI = 0.60, 0.82), PrEP subjective norms score (OR = 1.54; CI = 1.33, 1.78), communication frequency of a lot/a great deal (OR = 2.38; CI = 1.07, 5.29), and PrEP support (OR = 2.34; CI = 1.11, 4.94). Participants who worry about acquiring HIV, believe PrEP would be used or accepted by others (ie, higher PrEP subjective norms score), communicate with their provider a lot or a great deal, or believe their provider(s) would be supportive of PrEP use (ie, higher provider PrEP support score) are more likely to report interest in PrEP. However, participants who are in a relationship or believe PrEP use would not be approved by others (ie, higher PrEP disapproval score) are less likely to report interest in PrEP (Table 2).
Three of these six variables remain significantly associated with interest in PrEP in the full model – relationship status (OR = 0.29; CI = 0.11, 0.71), worry about acquiring HIV a little/some and a lot/great deal (ORs = 4.14 and 7.35; CIs = 1.74, 10.38 and 2.62, 22.56), and PrEP subjective norms score (OR = 1.60; CI = 1.31, 1.99). Participants who are in a relationship are 71% less likely to report interest in PrEP than participants who are single. Participants who worry a little/some or a lot/great deal about contracting HIV are more likely (4.1 times and 7.4 times, respectively) to report interest in PrEP than participants who do not worry about contracting HIV. Each unit increase in a participant's PrEP subjective norms score corresponds to a 60% increase in the likelihood of interest in PrEP (Table 2).
According to model statistics, there is a marked increase in the variability accounted for by models 2 (pseudo-R2 = 0.18) and 3 (pseudo-R2 = 0.37) (Table 2).
Discussion
Consistent with the literature on HDNs, healthcare-engaged women, as indicated by having seen a provider in the past 12 months and having health insurance, are more likely to list a provider as a health discussant network member. In addition, older Black women and Black women who are in a relationship are also more likely to do so. This suggests that this subset of the sample has positive ties to healthcare providers and is consistent with healthcare utilization statistics that suggest as individuals age, they are more likely to have health insurance and see a healthcare provider. 22 Further, this finding is consistent with robust evidence of increased PrEP use among insured populations 23 including Black women. 22
We found that Black women who had a provider in their HDN and had frequent communication with them or believed that their provider would support PrEP use resulted in an increased likelihood of being interested in PrEP. Although future studies may consider whether outcomes are instead the result of cisgender Black women's engagement in care as a driver for PrEP interest. This highlights the crucial role of healthcare provider support in PrEP engagement for Black women, echoing previous research emphasizing the importance of trustful relationships and provider awareness of specific health needs for Black and Latino women's interest and uptake of PrEP. 24
Our findings show that even among those with a provider in their HDN, interest in PrEP was less likely if Black women anticipated disapproval from those close to them. This underscores the significance of social support, norms, and approval as determining factors in PrEP engagement for Black women. The fear of stigma or disapproval from others, including family members, can deter Black women from considering PrEP despite having a supportive healthcare provider.25,26 Similar studies have highlighted how societal stigma, misconceptions about PrEP's effectiveness, and HIV-related stereotypes can influence Black women's decisions regarding PrEP use.20,27 Furthermore, providers may be hesitant to address sexual health topics with women, leading to a lack of discussion around these issues.7-10 Surveys have revealed that a low proportion of US women are asked about HIV or other STIs by their healthcare providers. 11
Despite the slow uptake of PrEP among Black women to date, our findings suggest that discussions with healthcare providers about PrEP, as part of comprehensive HIV prevention strategies, can improve PrEP uptake and reduce the risk of HIV infection. 28 The presence of providers in the HDNs of Black women indicates trust, accessibility, and a valuable source of information, which are crucial attributes for effective PrEP communication and initiation.18,24 However, provider support alone is not sufficient, as social factors such as stigma, approval, and support from close contacts significantly influence PrEP use among Black women.29-31 Therefore, a comprehensive approach to PrEP scale-up is necessary, integrating social factors operating at the peer, partner, provider, and familial levels.
While robust knowledge demonstrates provider trust as a key factor in PrEP engagement, our findings further emphasize the importance of healthcare provider support and the influence of social factors on PrEP engagement. Distinctly, our findings posit that the depth of patient–provider relationship, to the extent that cisgender Black women consider their providers a member of their health discussant network, may yield increased utilization of HIV preventative care. These results may indicate opportunities for health professionals to decrease encounters with stigma and shame for Black women when discussing PrEP, instead enhancing patient experiences and equitable access to PrEP care through trustful relationships. This study is among the first investigating the implications of health discussant networks in HIV prevention for women. As such, future research may consider the importance of multifaceted approaches, specifically the roles of social dynamics alongside provider–patient interactions, for successful PrEP implementation and uptake among Black women.
Footnotes
Authors’ Contributions
Material preparation, data collection, manuscript conceptualization, drafting, data analysis plan and analysis were performed by WCI. MAC contributed to the data analysis plan, manuscript conceptualization, review, and editing. AM contributed to the conceptualization, drafting, review and editing of the manuscript. All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author, WCI, upon reasonable request.
Declaration of Conflicting Interests
WCI receives funds to develop and deliver medical education related to PrEP from ViiV Healthcare. AM and MAC declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Statement and Approval
All procedures performed in this study were in accordance with the ethical standards of the Institutional Review Board at Washington University in St. Louis. (IRB201902109) and with the 1964 Helsinki declaration and its later amendments.
Funding
This publication was made possible by Grant Numbers T32 AI007433 from the National Institute of Allergy and Infectious Diseases, T32 DA15035 from the National Institute on Drug Abuse.
Grant Number
WCI: T32 AI007433 and T32 DA15035
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Trial registration number/date
Not applicable