
Abstract
Introduction
Across 40 years of the HIV epidemic, research has shifted an HIV diagnosis from a death sentence to a manageable, chronic illness. Perinatally infected youth living with HIV (YLWH), who must maintain lifelong treatment, still experience excess HIV-related morbidity and mortality despite the advent of life-saving antiretroviral therapy.1,2 YLWH have unique needs in both care and research settings, as they transition from childhood to adulthood, navigate the shifting involvement of caregivers in their care, and come to terms with their own HIV infection in contexts that may still include HIV-related stigma and discrimination.3,4 Due to these unique experiences, research involving YLWH is still urgently needed to enhance youth-specific HIV care,5,6 which has been demonstrated to improve care outcomes.6,7
Studies conducted in Kenya demonstrate that HIV-related stigma is omnipresent in the lives of YLWH, demonstrated by reports of stigma in community and school settings, and at home.2,8,9 Anticipated and enacted HIV-related stigma can lead to adverse mental health outcomes.8–10 Experiences with and fear of HIV-related stigma negatively impact HIV care initiation, treatment retention, and medication adherence and introduce significant barriers to the successful treatment of YLWH.11,12 Over time, HIV-related stigma can contribute to the excess morbidity and mortality experienced by this vulnerable group. YLWH employ multiple strategies to avoid HIV-related stigma, including choosing not to disclose their HIV status to family and friends, avoiding taking medications in front of others, and attending clinic appointments discretely or farther from home to avoid being associated with HIV care.8,11,12
Although the impacts of HIV-related stigma on clinical engagement and outcomes are well studied,13–15 it is not fully understood how it affects the ways in which YLWH chooses to participate and engage in research. YLWH must navigate the study's recruitment requirements, caregiver involvement in the process, and assess study-related risks and benefits, all of which may be influenced by experiences of HIV-related stigma and discrimination. Research on the perceived risks and benefits of research participation among YLWH in Kenya has illustrated that risks are not described as being of great concern to participants, despite pervasive fears of stigma and discrimination.8,16–19 Similar stigma-related impacts may lead to barriers to YLWH participating in research or increase the associated risks, placing an even stronger emphasis on protecting the confidentiality of their HIV status.
In order to ethically and successfully involve YLWH in research, it is critical that we understand the ways in which HIV-related stigma impacts engagement in research from recruitment of YLWH, enrollment and consent, and engagement in research activities. This qualitative study aims to explore the impacts of stigma on identifying and recruiting YLWH for research, their needs throughout the research process, and the stigma-related risks and benefits of YLWH participation in research, by eliciting the perspectives of YLWH, their caregivers, and subject matter experts (SMEs).
Methods
Study Setting
This study was conducted within the Academic Model Providing Access to Healthcare (AMPATH), an academic collaboration between Moi University School of Medicine, Moi Teaching and Referral Hospital (MTRH) in Eldoret, Kenya, and a consortium of North American universities led by Indiana University.20,21 AMPATH provides care for more than 7000 children and YLWH and includes the Rafiki Center for Excellence in Adolescent Health, one of the largest adolescent health centers in Africa.
This study is part of a broader, ongoing cohort study (“parent” study). 22 A cohort of YLWH was originally assembled in 2010 to 2013, followed by 2 completed longitudinal studies, and is currently participating in a third study. This series of studies longitudinally follow youth perinatally infected with HIV as they grow into adolescence and young adulthood in western Kenya, examining the associations between ART adherence, treatment failure, and the development of HIV drug resistance (HDR). The studies collected blood samples for viral load and drug resistance testing, which informed some of the interview questions for the present qualitative study. Eligibility for the original parent study was: (1) perinatally infected with HIV, (2) ≤14 years of age at enrollment, (3) on or initiating first-line NNRTI-based ART regimens, and (4) receiving HIV care at an AMPATH clinic. Participants were initially recruited during routine clinic visits, and none refused participation.
Study Design
This study enrolled 4 categories of participants: (1) YLWH who are currently enrolled in the parent study, (2) caregivers of YLWH enrolled in the parent study, (3) YLWH who have not participated in the parent study, and (4) SMEs.
The interviews covered 2 domains: (1) identifying, enrolling, and protecting YLWH in longitudinal clinical research, and (2) collecting, testing, biobanking, and sharing/future use of biological specimens. Domain 1 probed issues related to the age of consent and assent; how research involvement changes from childhood through adolescence and into adulthood; involvement of caregivers in research; protections against accidental disclosure of HIV status; and considerations related to research with a population with low socioeconomic status, high orphanhood, and living with HIV. Domain 2 probed perspectives on consenting for biological sampling; biospecimen storage practices; identifiable information linked to samples; the use of samples for future research studies or for public health surveillance related to HDR testing; responsibilities for providing testing results; and sharing of any potential profits emanating from future work. This paper discusses the stigma-related considerations arising from both domains 1 and 2.
Sampling and Recruitment
Youth participants involved in the parent study were recruited through random sampling from scheduled study and clinic visits for the parent study and were included only if they were (1) between 10 and 24 years of age, (2) aware of their HIV status, and (3) enrolled in the parent study. Caregivers were similarly recruited through random sampling from scheduled visits. Caregiver participants were eligible if they were (1) a caregiver of a YLWH enrolled in the parent study, (2) 18 years of age or older, (3) aware of the youth participants’ HIV status, and (4) knowledgeable about the care and research participation of the YLWH. Youth who were not enrolled in the parent study were randomly sampled from the Rafiki Center of Excellence in Adolescent Health, a local clinic providing HIV care to adolescents. Youth were eligible if they (1) were between 10 and 24 years of age, (2) were aware of their HIV status, (3) receive HIV care at the AMPATH/MTRH Rafiki Center of Excellence for Adolescent Health, and (4) were not enrolled in the parent study. Youth participants were selected purposively for equal gender groups. Subject matter experts were identified by the research team as experts in community leadership, healthcare provision, research, ethics, and policy. SME participants were eligible if they were: (1) 18 years of age or over and (2) determined by the study team to be an SME in one of the following groups: community leaders (village elders and chiefs), members of adolescent or community advisory boards, healthcare providers, members of local or national IRBs, researchers from the AMPATH Research Network and other institutions conducting research with YLWH in Kenya, research laboratory leadership, and government or policy representatives.
Data Collection and Analysis
Two trained Kenyan facilitators (1 male and 1 female) conducted interviews in either Kiswahili or English, depending on the participant's language preference. Facilitators were experienced in qualitative interviewing, trained in study protocols, and had no prior relationships with the participants. Interviews with adolescents, caregivers, and the majority of SMEs were conducted in private rooms in the clinical setting; some SMEs were interviewed in their private offices, and IRB members were interviewed virtually via Zoom. No field notes were collected during interviews and no external observers were present. Interview guides were tailored to probe topics relevant to each participant group. Interviews were audio-recorded, transcribed, and interviews conducted in Kiswahili were translated into English for analysis. Deductive thematic analysis was led by 2 researchers (HK and EG) based on an initial coding framework derived from the interview questions and reviewed by JA and AC. The researchers independently extracted data using the qualitative software program NVivo, version 12. 23 The same investigators (HK and EG) led the inductive analysis and extracted emerging themes independently before comparing results and reaching a consensus on relevant themes.
Definitions
HIV-related stigma is commonly defined as negative attitudes and beliefs about people living with HIV, which reduce an individual from a “whole and usual person to a tainted, discounted one.” 24 Although stigma is associated with attitudes and beliefs, discrimination refers to the behaviors resulting from these beliefs and is often described as an end result of stigmatization, or “enacted stigma.” 25 Stigma is often internalized by people living with HIV, leading to “self-stigma” in which one shares negative beliefs about their own HIV status. 26 Direct impacts of stigma or the anticipation of stigma often include fear of disclosing one's HIV status to others and of taking HIV medications in front of others, often leading to physical and clinical effects. 27 Impacts of stigma may also be indirect, such as increased mental health symptomology. 26
Ethical Approvals
This study was approved by the Icahn School of Medicine at Mount Sinai Institutional Review Board in New York, NY, USA (study number 20-01177), and the Moi University/Moi Teaching and Referral Hospital's Institutional Research and Ethics Committee in Eldoret, Kenya (approval number 0003689). Additional approval was received by the National Commission for Science, Technology and Innovation (NACOSTI), a Kenyan government research regulatory body (reference number NACOSTI/HW/3/1/16). Participants were excluded if they were unable to provide written informed consent, or in the case of those under 18 years of age, the inability to provide assent themselves and caregiver consent. A detailed, standardized informed consent/assent form written in either Kiswahili or English was read aloud with adequate time for questions and clarifications, and written consent/assent was obtained by trained, bilingual research assistants with experience in recruiting children for research.
Results
Participant Demographics
We enrolled 99 participants in the study in order to ensure saturation; 40 YLWH, 20 caregivers, and 39 SMEs: 5 community advisory board (CAB) members, 10 health care providers, 5 village chiefs, 5 Mtaa leads (community leaders), 5 IRB experts, 5 clinical researchers, 3 social science researchers, and 1 laboratory lead. The majority (52%) of all participants were female; 50% of YLWH were female (median age 17.5), 70% of caregivers were female, and 44% of SMEs were female.
HIV-Related Stigma: Perspectives of YLWH, Caregivers, and SMEs
Participants cited HIV-related stigma as a critical issue impacting YLWH, which subsequently impacts their involvement in research (Table 1). Many participants identified that, in general, YLWH is at a uniquely high risk of experiencing stigma, as they are at a transitionary life stage in which they further develop identities, seek community and peer approval, and navigate disclosure of their HIV status to peers. They described how youth, who are just beginning to establish their identity or careers, do not want to be defined exclusively by their HIV status. Moreover, during the developmental stage of adolescence, youth place high importance on their peers’ opinions and approval, making rejection or discrimination due to HIV status all the more devastating. Participants perceived YLWH under 18 to experience greater compounding effects of stigma due to a greater fear of stigma and developmental challenges associated with this period of adolescence, as they struggle to establish autonomy, particularly in HIV care management, and their own identity. Some also suggested that YLWH under 18 may not have fully accepted their status and are thus more likely to accidentally disclose their status to others, which may lead to increased stigmatizing experiences.
General Perspectives of YLWH, Caregivers, and SMEs on HIV-Related Stigma.

Abbreviations: PLWH, people living with HIV; YLWH, youth living with HIV; SME, subject matter expert.
Participants identified compounding direct and indirect effects of stigma on mental health, such as symptoms of anxiety, depression, or beginning substance use, compounding the discrimination and isolation from peers, family, and community members. Participants also described the physical effects of stigma; fear of anticipated stigma related to one's HIV status leads YLWH to hide and delay medication-taking, and then nonadherence can result in viral nonsuppression and the development of drug resistance. One SME described that the effects of stigma are interrelated with mental health and wellness; the mental health challenges associated with stigma may impact youths’ clinic and school attendance.
Few participants brought up suggestions to address stigma, but those who did suggest broadly that community leaders should help normalize living with HIV, and that research should be conducted with both HIV-positive and HIV-negative youth participants.
Stigma-Related Considerations for Engaging YLWH in Research
Participants recommended that researchers consider the extra sensitivity, care, and support needed by YLWH following lifetime experiences with stigma; YLWH may face barriers to participating in research due to fears of accidental disclosure and stigma that may arise from being associated with HIV research (Table 2). The need for adequate protections against research-related risks such as stigma and discrimination, and protecting the confidentiality of their HIV status were issues identified by YLWH and caregivers. YLWH and SMEs most commonly cited privacy, youth-friendly amenities, and a trusting relationship with researchers as critical needs to help mitigate the impacts and risks of stigma in a research environment. Participants explained that protecting the privacy of YLWH is critical to not accidentally disclosing one's status and the subsequent increased risk of YLWH experiencing stigma. Youth-friendly amenities and rapport with researchers were suggested as needs in response to the stress caused by prior experiences with stigma, and the need for YLWH to feel comfortable sharing personal details.
Stigma-Related Needs and Considerations for Engaging YLWH in Research.
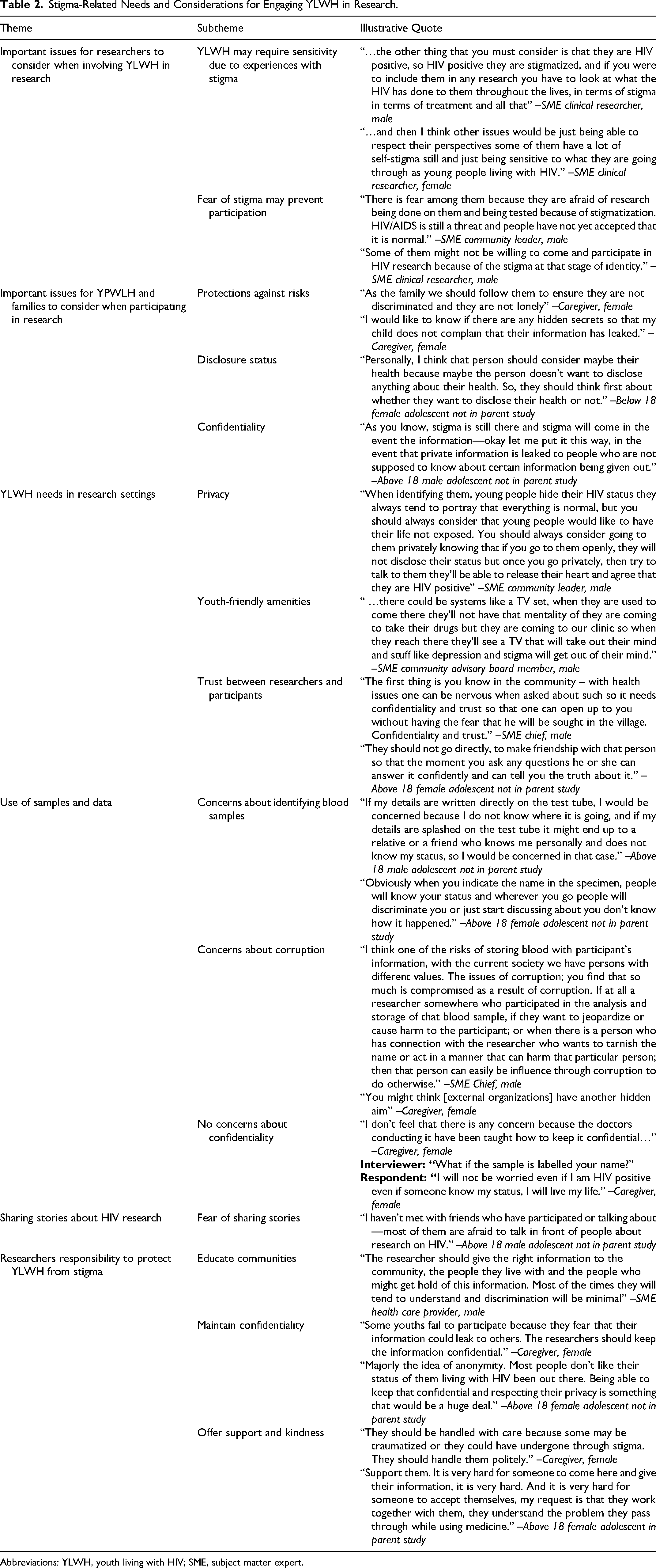
Abbreviations: YLWH, youth living with HIV; SME, subject matter expert.
Regarding the storage and sharing of biological samples for research purposes, participants expressed fears that research staff, other participants, or community members might see a participant's name on a sample and stigmatize them for their HIV status. Some SMEs and caregivers expressed concerns surrounding researchers being corrupt or wanting to cause harm to participants by sharing their HIV status. Others expressed that they had no concerns because research staff know how to maintain confidentiality. YLWH participants were prompted to share stories they had heard from peers participating in research; however, the overwhelming majority reported that they had not heard any, with some suggesting that their peers were afraid to discuss HIV research due to a fear of stigma.
Stigma-Related Risks and Benefits When Involving YLWH in Research
HIV-related stigma emerged repeatedly in the discussion of risks and benefits when involving YLWH in research. Participants identified accidental disclosure, stigmatization, and discrimination as risks of participating in research (Table 3). Accidental disclosure from the researcher to the YLWH and others was considered risk, as some YLWH was unaware of their status. Some participants cited that YLWH may be undisclosed because caregivers choose not to disclose their or their child's status out of fear of stigma if the child was to accidentally share their status with others. Some SMEs cited stigma among peers or within families as major risk, which could result in feelings of suicidality and isolation, being kicked out of the home, decreased school attendance, and worse medication adherence. YLWH and caregivers expressed concerns about self-stigma and discrimination in schools and among peers. Some caregivers did not see accidental disclosure as a risk because they trust that researchers will maintain confidentiality. Others, from all 3 participant groups, disagreed that stigma and discrimination were a risk of research, citing that stigma and discrimination are no longer concerns in their communities, following increased HIV-related education and sensitization.
Stigma-Related Risks and Benefits of Involving YLWH in Research.
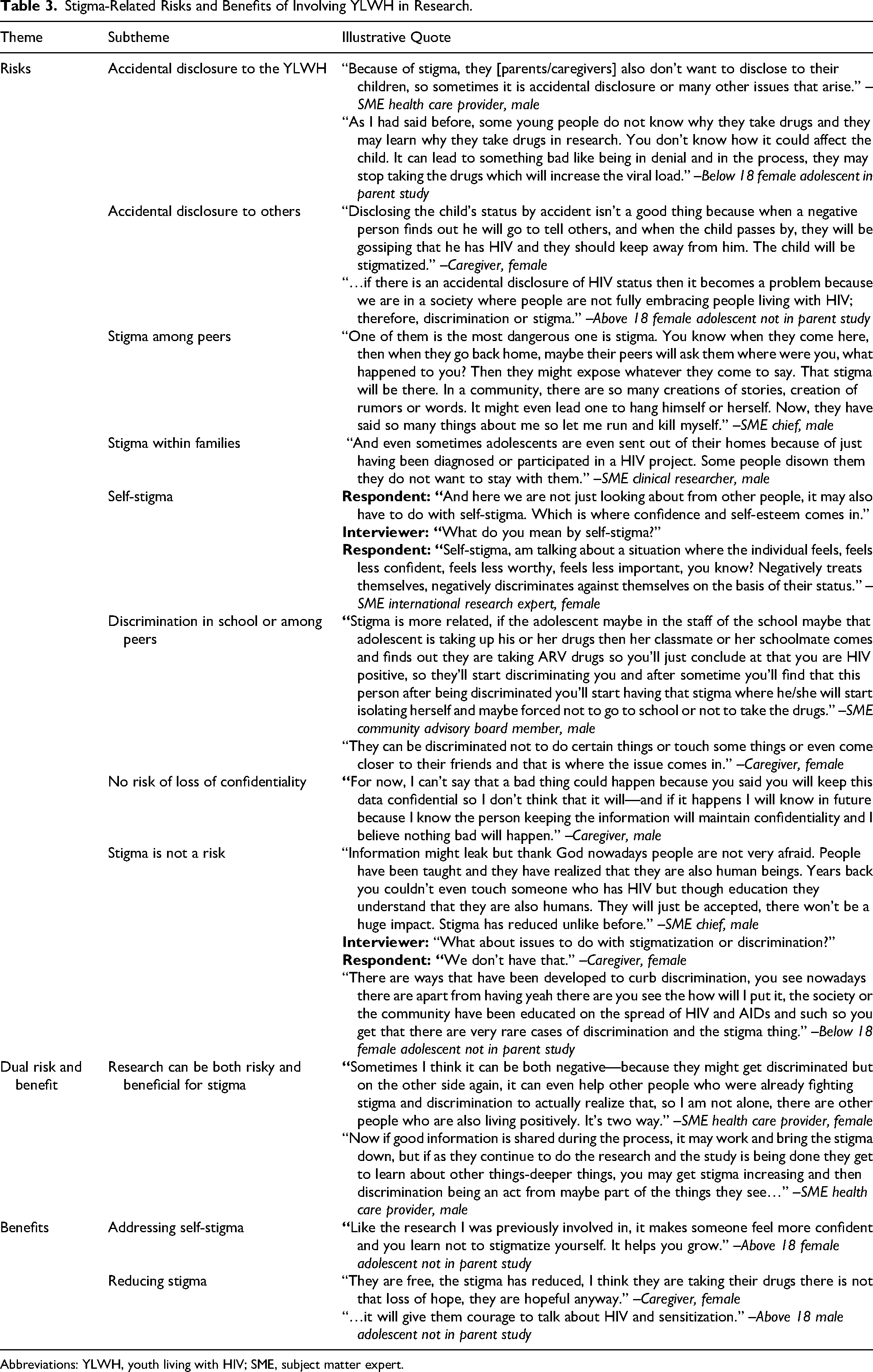
Abbreviations: YLWH, youth living with HIV; SME, subject matter expert.
A minority of SMEs described the research as both risky and beneficial in terms of stigma. They explained that while research can lead to stigma and discrimination through accidental disclosure, research can also reduce stigma by demonstrating to YLWH that they are not alone and by teaching communities about HIV. Some YLWH cited that research helped them address their own self-stigma; caregivers and YLWH both described that research gives YLWH the courage to openly discuss HIV, which sensitizes others and works to decrease the prevalence of stigma in their communities.
Stigma Considerations in Identifying and Approaching YLWH for Research
Participants described identifying YLWH for research purposes as difficult due to widespread fear of stigma, and many explained that recruiting and conducting research in private settings was an essential part of easing this fear (Table 4). When asked about their opinions on identifying YLWH through medical charts, many participants cited concerns that this method breaches confidentiality, and that by doing so, breaks the trust between YLWH and researchers. Participants expressed concerns about feeling that their privacy was violated, and that the medical chart interface could be managed incorrectly and result in their identity and HIV status being leaked, posing a risk of further stigma and discrimination. A minority reported having no concerns because the information remains within the hospital and the doctors maintain confidentiality.
Stigma considerations for identifying, approaching and enrolling YLWH in research.

Participants identified school settings, peer and social groups, the clinic, home settings, community health workers (CHWs), peer navigators, church, and community outreach as locations for which YLWH should be approached and recruited for research (Table 4). The majority of participants felt that recruiting at school would lead to accidental disclosure and discrimination by peers and teachers; however, some suggested that speaking generally about studies and inviting YLWH to come to the clinic to participate may be a way to safely recruit from schools. Participants were supportive of recruiting YLWH through social gatherings and peer groups, citing that YLWH are often more comfortable in these settings, and there is less fear of stigma in groups for YLWH. Similarly, there was support among participants for recruiting through peers living with HIV because YLWH are uniquely situated to be able to reach other YLWH and instill trust in research.
The clinic was commonly cited as the most appropriate place for recruitment because it is private, they have the support of the medical staff, and there is reduced fear of stigma at clinics that cater only to people living with HIV. Participants expressed concerns about recruitment through CHWs, citing that CHWs are known in the community to be involved in HIV testing and research, and being associated with a CHW could lead to accidental disclosure and stigmatization in the community. Some participants expressed concerns about recruitment in church settings due to the lack of privacy and youths’ fear of HIV stigma if identified as someone living with HIV. One participant mentioned that some churches teach more positively about HIV, and children and their parents may be receptive to advertising for studies at church. Participants suggested that village elders and chiefs are influential in promoting youth HIV testing, and therefore, may be a feasible resource in the recruitment process.
Discussion
HIV-related stigma continues to play a significant role in the lives of YLWH through anticipated and actual experiences; fear of stigma leads to changes in medication-taking behavior, disruptions in clinical HIV management, and even negative mental health. The results presented in this study demonstrate that beyond impacting youth clinical management, HIV-related stigma plays a significant role in how YLWH chooses to participate and engage in research. Participants described that anticipated stigma affects whether and how YLWH participates in research, where it is appropriate to recruit participants, the unique needs of this group in research settings, and the risks and benefits they perceive as part of research participation. These results support other findings that YLWH may see their HIV status as something that contributes to a sense of “difference” or isolation from their peers and that makes it challenging to relate to and form relationships with peers.28–30
In discussing research participation, YLWH participants repeatedly emphasized the potential role and impact of HIV stigma, including fear of their HIV status being exposed through research participation and anticipating stigmatizing experiences if their status were exposed. Participants cited fears of accidental disclosure in the research process as YLWH are recruited or identified for studies, by being seen at the clinic for study visits, and through others seeing their names on research-related blood samples. These concerns are shared by YLWH in other work in Kenya, who have expressed fear of sharing their HIV status, whether purposefully or accidentally, due to experienced, anticipated, and internalized stigma.8,9,27,31–33 It is well-documented that HIV-related stigma impacts care-seeking and other behaviors among YLWH, and this study's findings demonstrate that fear of stigma also affects how YLWH engages in research.27,34 Globally, studies have shown that HIV disclosure can be associated with feelings of isolation, anxiety, depression, negative self-image, and internalized blame.35–39 It is, therefore, critical to ensure that adequate protections are in place to protect the confidentiality of research participants’ HIV status and minimize the risk of accidental disclosure and associated negative outcomes.
The majority of participants cited the clinic as the most appropriate location for identifying and recruiting research participants because stigma and discrimination are highly prevalent in other settings, including schools, churches, and communities; these findings align with previous research in Kenya which demonstrates that YLWH experience and anticipate stigma in a variety of settings.8,27,32,40,41 Participants were most concerned about research recruitment in the school setting, as YLWH experiences stigma and discrimination from both peers and teachers. Research in Kenya, South Africa, Zambia, and Ghana has demonstrated that stigma is highly prevalent in school settings and is enacted by both students and teachers, suggesting that school-based stigma interventions may need to be prioritized.32,42–45
Participants identified accidental disclosure, stigma, and discrimination as major risks of research participation; however, a minority of participants suggested that these were not risks because stigma and discrimination no longer exist in their communities. Although recent literature suggests that levels of knowledge about HIV are increasing in Kenya, few other studies have reported decreasing levels of HIV-related stigma or discrimination.8,9,31 This may improve in the future; however, some participants believed that research was beneficial because it addresses and reduces stigma.
This study has a number of strengths. Using qualitative methodology allowed for an in-depth understanding of participants’ perspectives and experiences, and enrolling participants from a variety of backgrounds provided a broad spectrum of views on the involvement of YLWH in research. Particularly, involving YLWH who have participated in research for multiple years provided unique and highly relevant insights. Having 2 sets of independent analysts, both with 1 Kenyan and 1 American investigator, mitigated the risk of bias introduced by personal reflexivity and cultural backgrounds. This study also has a number of limitations. The study was conducted in a single country, and may not be generalizable to many other contexts, but is likely applicable to other African countries considering the significant research and care for YLWH conducted in Kenya. The number of participants was relatively small but adequate for achieving thematic saturation in the relevant topic areas. Additionally, we included YLWH who were uniquely experienced in research and highly studied, and we mitigated this bias by purposively sampling YLWH who had not participated in the research.
Conclusion
YLWH, their caregivers, and SMEs across multiple disciplines observe and experience HIV-related stigma, which impacts not only clinical management but also the ways in which YLWH participates in research critical to the improvement of youth HIV management. These results suggest that researchers should address the role of stigma in research with YLWH by recruiting participants discreetly in private, comfortable locations, being gentle and developing trusting relationships with YLWH participants, and protecting participants’ privacy and confidentiality throughout the research process. These findings align with other studies in sub-Saharan Africa which suggests that people living with HIV strongly consider when deciding to participate in research is whether they trust the researchers and study staff, and one of the main characteristics YLWH looks for in youth-friendly services and research is the friendly staff.46,47
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a grant (3R01AI147333-02S1) awarded to Drs. Rami Kantor and Rachel Vreeman through the National Institutes for Health and partially funded by K24AI134359 and P30AI042853.