
Abstract
During public health crises, people living with HIV (PLWH) may become disengaged from care. The goal of this study was to understand the impact of the COVID-19 pandemic and recent flooding disasters on HIV care delivery in western Kenya. We conducted ten individual in-depth interviews with HIV providers across four health facilities. We used an iterative and integrated inductive and deductive data analysis approach to generate four themes. First, increased structural interruptions created exacerbating strain on health facilities. Second, there was increased physical and psychosocial burnout among providers. Third, patient uptake of services along the HIV continuum decreased, particularly among vulnerable patients. Finally, existing community-based programs and teleconsultations could be adapted to provide differentiated HIV care. Community-centric care programs, with an emphasis on overcoming the social, economic, and structural barriers will be crucial to ensure optimal care and limit the impact of public health disruptions on HIV care globally.
Keywords
Introduction
Beginning in 2020, the COVID-19 pandemic brought overall disruptions to essential health service delivery in sub-Saharan Africa (SSA), which bears the highest burden of HIV globally. 1 The accumulating evidence demonstrates that advances in HIV testing and treatment have slowed because of the pandemic, and there is substantial concern that this may have the potential to lead to increased HIV-related morbidity and mortality.1–4 In Kenya, social and physical distancing mandates, including lockdowns, were immediately imposed after its first confirmed COVID-19 case on March 12, 2020. 5 While these mitigation strategies were crucial in curbing the spread of COVID-19, people living with HIV (PLWH) may have been more susceptible to disengaging in HIV care due to both social vulnerabilities and underlying comorbidities.2,6
Additionally, other types of public health crises, such as natural disasters including floods, droughts, or earthquakes, have also been documented to impose major challenges on PLWH due to impacts on physical infrastructure.7–9 For example, in March 2020, Kenya's rainy season intensified unexpectedly through May 2020. Over 233,000 individuals across 75% of the country's counties (primarily in western Kenya) were impacted leading to health emergencies, displacement, flash floods, landslides, and death. 10 The resulting economic and livelihood-related challenges could also have led to adverse consequences related to HIV care access and engagement.11,12 Within the more disadvantaged populations and residents living in these impacted areas, these consequences were experienced in an even greater magnitude. 7 For example, unemployment, food insecurity, financial insecurity, lack of transportation, and inability to afford preventive measures such as physical distancing and protective equipment during this period could have further reduced patient motivation to continue engaging in HIV care.13,14 Even in settings where there was a reasonable effort dedicated to addressing these issues prior to the pandemic, the dual challenges of an unprecedented global pandemic and natural disaster would have adversely impacted healthcare utilization and access. Characterizing these impacts is the first step in developing and disseminating interventions to maintain and improve care access in the future.15,16
Sustaining safe and high-quality HIV care depends critically on frontline healthcare providers.17,18 During times of public health crises, frontline healthcare providers, such as clinicians or nurses, thus provide an essential perspective on the impacts to care delivery and patient engagement. Therefore, understanding their perspectives and insights is critical in ensuring that health systems are prepared to support patients. The goal of this study was to understand the impact of the COVID-19 pandemic and flooding on care delivery through the lens of frontline HIV healthcare providers during the early phase of the COVID-19 pandemic. The objectives were to (1) gain insights about the implications of interruptions in HIV care engagement and viral suppression at the individual-patient level and health system levels and (2) identify mitigation strategies employed to overcome these interruptions. To achieve these two objectives, we examined the impact of COVID-19 and flooding on the delivery of care across the HIV care continuum, from the perspective of healthcare providers, and their perceptions regarding how these events had an impact on patient engagement in HIV care. Additionally, we explored providers’ perspectives on whether mitigation strategies, such as community-based medication delivery and telemedicine, could be leveraged to promote resilient models of HIV care that could withstand unanticipated disruptions in resource-limited settings during public health crises.
Methods
Study Setting
This study was conducted within the Academic Model Providing Access to Healthcare (AMPATH) in western Kenya. AMPATH is an academic partnership between Moi University, Moi Teaching and Referral Hospital, and a consortium of academic institutions led by Indiana University. 19 Since 2001, AMPATH has been a key partner of the Kenya Ministry of Health (MOH) and the National AIDS and STI Control Program to create and implement prevention and treatment programs to support HIV patients. To date, the program has provided HIV care services for approximately 110,000 + active patients living with HIV across 300 + MOH-supported clinics in western Kenya. 20 AMPATH also provides primary- to tertiary-level care services at health facilities, and community-based care programs including community-based medication deliveries through community-ART groups (CAGs), community-based care delivery for non-communicable diseases and maternal and child health, and economic programs to address social determinants of health through group-based microfinance, agricultural, and income generation activities.21–26 For HIV care, established and stable HIV patients within the AMPATH program are routinely seen by HIV-trained clinicians with a 3–6 month return-to-clinic (RTC) date for follow-ups. 17 The clinician-to-patient ratio is estimated to be 1:1300–1550. 27 All HIV clinical visits, labs, and medications are provided at no cost to patients. Antiretroviral therapies (ART) are given for a duration of 3 months, after which a patient may come back to the health facility to receive a refill. Eligible patients are enrolled in CAGs where they receive ART delivered to them in the community every 3 months, with an in-person clinical visit at the facility every 6 months. Viral loads for virally suppressed patients are ordered and taken at the facility laboratory every 12 months. For patients who are not virally suppressed, a repeat viral load test is typically ordered after 3 months in combination with enhanced adherence counseling. All viral load testing procedures comply with recommendations from the National AIDS and STI Control Program, MOH in Kenya. 28
Study Sites
The study was conducted at four health facilities in two counties, Busia and Trans Nzoia, within the AMPATH catchment area. Selection of the counties was based on their long-standing HIV care infrastructure through facility-based and differentiated community-based care via CAGs.21,25 Additionally, at the time of the study, the counties were sites for our clinical trial in which a community-based HIV intervention would be deployed (ClinicalTrials.gov Identifier: NCT04417127). Selection of the health facilities within the two counties was informed by two main factors; one was the presence/absence of flooding events (Busia County was severely affected by floods), and the other was the level of site-specific and locally imposed COVID-19 restrictions (while the government issued safety recommendations, how these recommendations were implemented may vary between and within counties based on the local administration, COVID infection severity, and available resources at each site. In Trans Nzoia county, one study site had a stricter implementation of COVID safety recommendations than the other.)
Study Design
Between October and December 2020, we conducted 10 telephone-based individual in-depth interviews with HIV providers to explore the impact of COVID-19 on HIV care delivery, the impact of COVID-19 on providers and patients, and mitigation strategies employed to alleviate the downstream impact on HIV treatment outcomes, including ART delivery and telemedicine. A semistructured interview guide was designed to elicit information in these specific areas from HIV providers who continued to provide care for HIV patients during the early phases of the COVID-19 pandemic and in the aftermath of the flooding. Trained researchers identified, contacted, and obtained informed consent from participants. Each interview lasted approximately one hour and was conducted on the telephone in English and/or Swahili. At the end of each interview, participants were compensated with 500 Kenyan shillings (approximately 5 US dollars) in appreciation for their time.
Study Participants
We invited 10 HIV care providers from four different health facilities in the two specified counties. Participants were chosen because they were frontline clinicians or nurses providing care to HIV patients during the COVID-19 pandemic. All participants directly provided care for patients at the health facilities, and some played leadership roles within facilities. Selection of the providers was also based on the number of years that they had been providing HIV care and number of years on staff at AMPATH. In addition, providers holding various clinical and administrative positions were invited to ensure different types of responsibilities were captured. The number of interviews was based on our consensus that interviews would not disrupt providers’ care responsibilities while ensuring that content saturation would be reached. Verbal consent was obtained from all participants prior to commencing the interviews.
Data Collection and Analysis
Data collection was conducted by experienced researchers from the AMPATH Social-Behavioral Team. All interviews were audio-recorded. Recorded interviews were transcribed in full and then translated into English. De-identified text data were imported to NVivo (Copyright © 1999-2021
Ethical Approval and Informed Consent
This study was approved by the Moi Teaching and Referral Hospital/Moi University Institutional Research and Ethics Committee, Eldoret, Kenya, under Reference IREC/2020/120, Approval Number 0003659. Verbal consent was obtained from all participants prior to commencing the interviews. The study investigators provided verbal informed consent, instead of written informed consent, for the following reasons. First, the study period occurred between October and December 2020, before the availability of any COVID-19 vaccines and during a time when social and physical distancing was advised in Kenya. Limiting physical interactions whenever possible to avoid the unnecessary spread of COVID-19 to participants was a safety priority of our research team. All interviews and informed consent were conducted via the telephone. During the consent process, the interviewer provided a description of the study (ie, introduction, purpose, procedures, reimbursement, confidentiality, risks, and benefits) to participants. Participants were free to ask follow-up questions about the study. Finally, participants were asked to verbally state if they would be willing to take part in the interview. No identifiable information was recorded at any time during the interview.
Results
Participant Characteristics
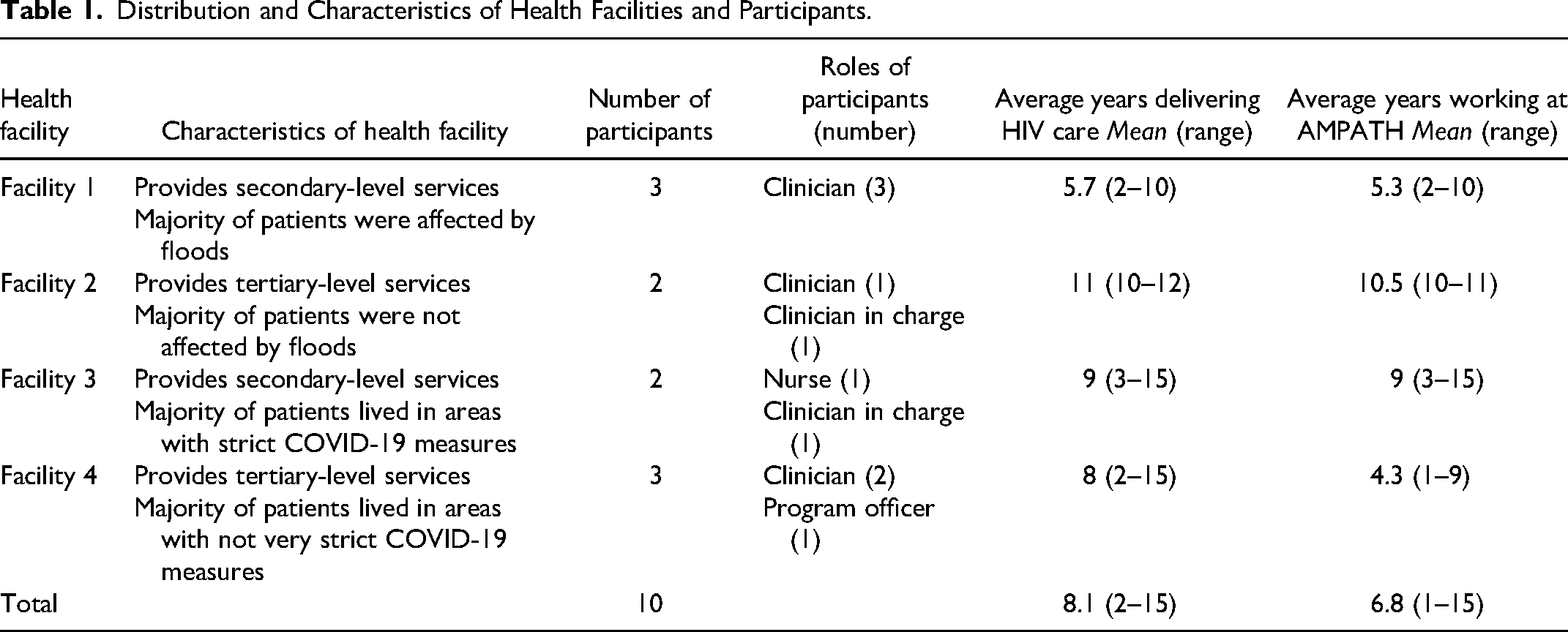
The distribution and characteristics of health facilities and participants are shown in Table 1.
Distribution and Characteristics of Health Facilities and Participants.
Our study objectives were (1) to gain insights from providers about the implications of interruptions in HIV care engagement and viral suppression at the health facility and individual patient levels and (2) to identify mitigation strategies employed to overcome these interruptions. Under objective 1, we identified three themes at the system, provider, and patient levels related to increased structural constraints, increased provider physical and psychological burnout, and decreased patient uptake of HIV services along the HIV care continuum. Under objective 2, we uncovered one theme related to strategies to mitigate the negative impact of the identified interruptions.
Theme 1: Increased Structural Constraints Created Exacerbating Strain on the Health Facilities and Healthcare Providers
First, providers discussed structural constraints for care delivery and how they led to changes in care provision to patients during the pandemic. These changes included, but are not limited to, limited discussions of sensitive health issues. Due to already-existing space limitations within the clinic area, it was even more difficult to maintain social distancing as congestion from the sheer number of patients passing through the triaging area and waiting area became a heightened concern. Perceived congestion was largely due to healthcare provider/staffing shortages (ie, less clinicians and staff were available to take care of the same number of patients). Healthcare providers and staff shortages were caused by: COVID exposure and clinicians going into quarantine, fear of COVID exposure and transmission and some staff members took early leave, and some clinicians had to take on additional responsibilities such as telephone and physical tracing of defaulters. Due to social distancing between patients and providers, patient privacy could not be protected during one-on-one consultations, especially during discussions of confidential health issues, resulting in patients potentially withholding information from clinicians.
Remember with the distance we also had issues to do with privacy because the client is far and the way you communicate to a client, clients around could hear most of your discussions so some of the clients would be very shy to disclose most of their real issues.
Second, the presence of severe flooding in Busia added additional burdens to clinicians on top of the responsibilities due to the existing COVID pandemic. During this time, multiple local clinics were forced to close because of flooding and patients from these clinics attended clinics that remained open. This meant an increased number of patients for some clinics during the concurrent pandemic and natural disaster.
I don’t think it is related so much to COVID but you know these sides [Busia County] we had COVID and floods. So, when we had floods, some clinics had to be closed, so the clients came to our clinic for care, so it is like we had more clients but same number of providers.
Third, providers also discussed how supply chain shortages had an impact on the quality of care they were able to provide to their patients. Besides the lack of reagents for basic patient-care laboratory investigations, inadequate and inconsistent availability of PPE for providers remained the most significant problem. As a result, clinicians had to avoid performing physical examinations to reduce COVID-19 infection risk during patient encounters, which impacted the quality of care they perceived they provided.
We don't know which patient for example has COVID or don't have COVID. We don't have protective gears or PPEs in our facilities. So, we may handle a patient and maybe one of the patients we handled had COVID-19. So it has forced us not to take BP [blood pressure] for patients because we want to minimize physical contact now that we don't have protective gears to handle them.
Finally, during the pandemic, providers expressed their perceptions regarding the lack of consistent protection of workers across systems of care. Some discussed differential risk compensation, allowances, and resource availability across different programs. As a result, providers discussed a lack of morale and that they felt undervalued by the care program.
We have been wondering why we were not given the COVID allowance, yet we have been working and risking our lives … that should have been taken into consideration to motivate us but we have never been given.
Theme 2: Increased Physical and Psychosocial Burnout among Healthcare Providers
Healthcare providers described the impacts of the pandemic on their physical and mental well-being. First, given the space constraints, providers expressed fears and anxiety about contracting COVID-19 from continuous interactions with patients in the crowded clinical setting. This anxiety was heightened especially when they interacted with patients who displayed signs of respiratory illnesses as they were not sure whether such patients had COVID, tuberculosis, or other respiratory illnesses. These providers had to overcome their fears to maintain care delivery to patients, fully knowing that their fear and anxiety may be impacting their performance.
Then personally, fear of unknown. You don't know what will happen because you are seeing so many patients, then the cases of Covid-19 has been increasing since the beginning. So, for my part personally you realize you fear, you don't know what will happen next, yeah, and that affects your outcome generally as a practitioner.
Second, providers also expressed suffering from physical exhaustion and burnout due to increased clinical responsibilities—some duties were previously not within their site of practice. For example, AMPATH HIV clinicians were trained to provide care for patients in the outpatient setting. If patients were admitted to the hospitals, they would be tended for by inpatient clinicians and staff. During COVID-19, some AMPATH HIV clinicians also went to the inpatient side of the hospital units to provide additional clinical care for hospitalized HIV patients. Altogether, a decrease in clinical staff and an increase in patient numbers, coupled with exhaustion as providers were not able to take a break, added physical strain on providers.
… you can imagine the strain that was there with the little we have especially the human resource to take care of that number because the hospital wants us and the ward to assist the MCH [maternal and child health] but then staff from the ward most of them had very little knowledge on HIV and the management of HIV … We were able to do that, by that time the clinic was extremely exhausted, extremely busy…”
Finally, providers also described experiencing additional emotional distress as they were often placed in dire patient situations in which they felt obligated to use personal resources to support patients with their social, economic, and transportation needs. While it had been normal for providers to encounter patients who needed material support prior to the pandemic, socioeconomic needs of HIV patients increased significantly during COVID-19.
As also providers, because there was even a nurse who came to me telling me that there is a client who does not have fare to go back [home]. So, we had to raise money for her, 20, 50, 100 here and there, because you can't just give them fare, you add her 100 or 200 for the family. I mean, it has really affected us in that sense.
Theme 3: Decreased Patient Uptake of HIV Services Along the HIV Care Continuum, with Most Salient Impact among Vulnerable Patients
Patient care interruptions cut across the entire HIV care continuum including diagnosis, linkage, treatment, retention, and viral suppression, as summarized in Figure 1.

Interruptions to the HIV care continuum.
Providers perceived decreases in testing activities for the identification of new cases during the initial phase of the pandemic. This was attributed to social and physical distancing mandates in the community where previous home-based and community-based testing efforts had successfully occurred. Providers also reported reductions in facility-based testing through voluntary counseling and testing services.
On the same HTS [HIV Testing Services], we used to have what we call moonlight hot spot testing, and you see these are gatherings. And with the pandemic, gathering were banned. So, you realize these are things that were affected when it comes to the first 90 [UNAIDS goal of 90% of PLWH knowing their diagnosis].
As seen with a decline in testing, providers believed linkage to care for newly diagnosed HIV cases was also negatively impacted due to patients’ fear of potential COVID-19 exposure and infection at the health facility.
Linkage was also affected in a way because when you say you link a client to a certain facility, maybe when he hears that someone tested positive for COVID-19 in that health facility … that client will not go to that facility again, so it will be a missed opportunity.
From a medication access standpoint, structural barriers such as mobility restrictions prevented patients from accessing health facilities to pick up ART. Specifically, providers noted that patients who had already been away in other areas of Kenya, or across the border in a neighboring country such as Uganda, were unable to come to their usual health facility for their medications.
Yes, adherence it has been affected because those who are locked down especially in Nairobi, and Mombasa and Uganda, … some of them never went to access other health facilities, so they never took drugs.
A number of health facilities in Busia County were uniquely impacted by severe flooding. Multiple interruptions due to these flooding events, in combination with COVID-19, resulted in housing displacement and exacerbated food insecurity, impacting patients’ ability to access and adhere to ART.
There are those who have been complaining but I can’t blame it on Corona. It was due to floods so there was a time the program bought food for them. There was a combination of floods and COVID so people lost property and they were many. They have been staying in schools and Churches for long so getting food was a problem…
Providers also discussed the downstream impacts of COVID-19, mediated by loss of income, on patients’ mental health. Specifically, depression, followed by alcohol use, prevented patients from being motivated to continue adhering to ART.
… we live around lakeshore areas so most of them depend on fishing as their economic activity so it has really affected them because of the lock down issues. Now they are depressed, they cannot take their drugs on time … And then this also leads to poor adherence and then they have high viral loads … And then some of them, due to depression, have also gone into taking alcohol that they are managing stress …. They take alcohol they don’t want to take their medicine well.”
From the providers’ perspective, socio-economic barriers also reduced retention in care. Economic instability arose from the loss of employment due to lockdowns and, therefore, income generation. As such, the ability to afford necessities such as masks, to pay for increased transportation fares to reach health facilities, and to cover the rising costs of living became competing factors destabilizing patients’ ability to continue seeking and retaining care at the same health facilities.
So, you realize most patients who have been affected are patients of low socioeconomic status who depended on small businesses to run their daily activities and their families. So, you realize when Covid-19 started, their businesses were affected, and as a result of that you realize they even currently cannot be able to afford transport to come to the facility, afford a meal for the entire family and sometimes you get they have more than 2 people in the family who are HIV positive so they need good nutrition. So, for them it becomes a bigger challenge to come to the clinic.
Special populations such as children, adolescents, elderly, and disabled patients experienced significant disruptions, not particularly with receiving direct care services, but with social support, transportation means, and other economic challenges, preventing them from optimizing their therapies, picking up their medications, or going to the health facilities for care.
And then in terms of age you realize that patients who are above 55, I would say, the elderly, most of them fear because out there they were told about the risk factor of COVID-19 relating to age. So, most of them depend on either their grandchildren or children during this period to come and pick for them medication. So, those ones who have children who are staying far, and maybe their grandchildren are not around, you realize getting them becomes a problem and taking medication becomes a problem. You realize now our retention comes in there now, getting them back to care becomes a problem.
Lastly, providers also expressed difficulty in monitoring patients’ viral loads due to disruptions in routine clinical appointments. Normally, patients with viremia, for example, would be given short RTC dates for closer monitoring. However, during the pandemic, providers reported that such patients were given longer RTC dates to decongest the clinics. Other patients might choose to seek care temporarily from different health facilities. Because these systems were not universally connected through a unified electronic medical record system, providers were unable to access patients’ records and appropriately keep them on schedule for follow-ups. This negatively impacted aspects of their HIV care plans, such as the timeliness of their routine viral load testing.
The other aspect that is affected by this pandemic is the area of viral load uptake because you realize that a patient decides to go to another facility to pick drugs. They are given drugs the first month. They go to a different facility the second month, they pick another batch of drugs, the third month, you know. All those times for the last 7 months since the pandemic, so you realize that a patient who was supposed to have a viral load done let's say in April or May ends up having her viral load done in maybe November …”
Theme 4: Existing Community-Based Programs and Virtual Technologies Could Be Adapted to More Systematically Provide Differentiated Care During Periods of Public Health Crises
Many providers described beneficial approaches that enabled ART to be conveniently provided to all patients during the pandemic. Those approaches revolved around community-based medication delivery programs through individual outreach efforts or organized community-based ART groups (CAGs). CAGs are formed by patients living with HIV through the support of health facilities. Each CAG consists of around 10–15 patients who meet the following criteria: are stable on their current ART regimen, have demonstrated good adherence and follow-up, and have no other health complications or chronic conditions. Every 3 months, health facility pharmacies pre-pack ART for all the group members in brown bags. Representative group members of each group will pick up the pre-packed ART packages from the pharmacy and distributes them to each member of the group. ART distribution points are agreed upon by the group members and can be at a patient's home or a common community meet-up point. All CAG patients still have regular 6-monthly clinical follow-up visits at the health facility. The group members distributing ART also complete various forms to ensure accountability of medication distribution.
28
The providers listed many advantages observed with medication delivery approaches which included increased access to ART, adherence to medications, and trust between the patient and the provider/health system while reducing workload, facility congestion, defaulter rates, and patient costs. These approaches were noted as having unique advantages towards vulnerable patient populations such as elderly, disabled, socio-economically challenged, and defaulting or lost-to-follow-up patients.
… when we do community distribution, patients will not have to travel long distances to come, we will have to go for them; and then we will have also solved the story of retention plus poor adherence to medication due to lack of transport and lack of means of reaching to facilities. I think that is the major and the best benefit; and of course, others also, they will also feel to be part of the integral unit of the facility. They will feel that we care for them and they will see that the facility, the healthcare workers move with them and care for them much. So, they will end up trusting, their trust on the healthcare system in terms of HIV management through AMPATH might really increase.
Having encounters with clients over the phone, it has reduced the number of visits being made by clients to the facility. That is a good measure with regards to ensuring that COVID 19 is not transmitted. A few clients will be visiting the facility compared to a greater number of clients. It has also been effective in providing adherence counseling and providing education on the importance of being adherent to ART because clients could make consultations on their health and also seek information on issues pertaining their health. That has been effective in reaching out to clients who could not make it to the facility during this COVID 19.
Discussion
Our qualitative findings characterized ways in which the COVID-19 pandemic and severe flooding interrupted HIV care delivery in western Kenya, as experienced by frontline HIV care providers. First, system-level changes due to the pandemic trickled down to create constraints with respect to healthcare delivery, both at the health facility and the health-provider levels. Frontline providers also experienced an exacerbating burden on their physical and psychosocial well-being during the initial phase of COVID-19 and in the aftermath of the floods. Second, our frontline providers described their observations of how these interruptions impeded their ability to provide high-quality patient care at each step of the HIV care continuum. Importantly, these interruptions disproportionately impacted the most vulnerable patients, including socio-economically disadvantaged populations, children/adolescents/elderly, and patients with physical disabilities. Lastly, the pandemic accelerated interest in community-based programs and telemedicine for differentiated care, given their potential to mitigate strain on the healthcare system and providers to benefit patients who are most at risk from the consequences of these events.
Stress, burnout, and mental health challenges among frontline healthcare providers during COVID-19 have been well documented across multiple care settings globally.29,30 In other natural disaster and public health crises, such as the 2003 SARS outbreak or the 2003–2006 Ebola epidemic, adverse mental health outcomes were also reported.31,32 In difficult work conditions and environments where resources are extremely limited, these challenges become magnified. 33 Our current study adds to the limited literature detailing the mental health impacts of COVID-19 on healthcare providers in Kenya, which is built upon an already constrained clinical work environment. 34 Because sustainability of the entire HIV care delivery continuum depends on the presence of healthcare providers who are physically and mentally healthy to care for patients, additional pathways must be established to support frontline healthcare providers during periods of social upheaval. 35 Our findings suggest that protecting providers from occupational health hazards through low-cost interventions, such as adequate protective equipment, would be essential in this regard. 35 Additionally, there should be careful consideration and fair allocation of risk allowances, and collaboration with other community health workers for organized task-shifting.35–37
In the early phase of the pandemic, HIV essential services were substantially interrupted across SSA.2,4,6 Our findings from providers in Kenya resemble what has been reported in the literature. 14 Across the HIV care continuum, declines in testing, linkage, treatment, retention, and viral suppression were observed. 4 However, these declines seem to be transient, and rebounds have been documented as the pandemic progresses. 4 One unexpected consequence of the pandemic may have been the acceleration of differentiated care models in SSA, which contributed to the quick rebounds described above. 38 Prior to the pandemic, the implementation of differentiated care models had already been in place to transition stable patients to more efficient models of HIV care delivery. 39 During the pandemic, programs leveraged these models and built upon them to ensure patient-centered care and timely delivery of treatment to PLWH. Those efforts included expanding eligibility for differentiated service delivery for HIV treatment, extending multi-month dispensing and reducing the frequency of clinical consultations, emphasizing community-based models, and integrating preventative (eg, TB, family planning) and primary care (eg, non-communicable disease treatments). 38 Differentiated care services with a focus on community-based care have the potential to extend HIV care to hard-to-reach patient populations who face socioeconomic barriers. In the context of COVID-19, it is clear that holistic strategies to address the social determinants of health, namely socioeconomic challenges, food insecurity, transportation barriers, and stigma faced by PLWH, must be incorporated as part of HIV care delivery going forward.13,14
Telemedicine has the potential to be employed with high acceptability among providers. However, challenges surrounding implementation to ensure equitable access to these services must be addressed if these strategies are to bridge gaps in care during times of public health crises for the most vulnerable patient populations. 40 Recommendations from providers to overcome these challenges (ie, accessibility, proficiency and confidence in technology use, confidentiality concerns) could inform the development and expansion of a more robust telemedicine service within low- and middle-income countries. 41
Our study was not without its limitations. First, we included healthcare providers from only two restricted geographical counties within our care program. While this may have limited our ability to generalize our findings, we were intentional in selecting providers from health facilities where we had established a good rapport, ensuring that providers were comfortable sharing their critical perspectives with our trained interviewers. Another limitation of this study is that it focused primarily on perspectives from providers and not from PLWH. Our study team is currently undertaking efforts to analyze and present data collected from PLWH to add insights into challenges and opportunities experienced during COVID-19.
Conclusions
Healthcare providers working and providing care in resource-limited settings experienced insurmountable challenges to continue providing care to PLWH at different stages of the HIV care continuum. Policies and programs to protect healthcare providers from physical and psychosocial distress, especially during times of public health crises, must be implemented. Differentiated care models through community-based or telehealth programs have the potential to alleviate exacerbating strain on health facilities, health providers, and better serve vulnerable patient populations most at-risk from health crises such as COVID-19 and natural disasters.
Footnotes
Acknowledgments
We thank the administrative leadership and the clinicians for taking the time to share their stories. We also thank the AMPATH Social and Behavioral Team for their expertise in conducting the interviews.
Declaration of Conflict Interests
SDP serves as a consultant for Abbott Labs and Becton Dickinson for philanthropic work unrelated to the work described here. All other authors declare no competing interests.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Johns Hopkins Alliance for a Healthier World Launchpad Grant. Authors DNT, CK, JW, JS, SP, OG, and BLG are also supported by the National Institute of Mental Health of the National Institutes of Health under award number 5R01MH118075. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. The content of this work is solely the responsibilities of the authors and does not necessarily represent official views of the Johns Hopkins Alliance for A Healthier World or the National Institutes of Health.