
Abstract
Background:
People living with HIV (PLWH) have been shown to have an increased risk of autoimmune diseases. Corticosteroids are the cornerstone of autoimmune diseases treatment, but their use is associated with an increased risk of infections. It is unclear how HIV status affects the risk of infection associated with corticosteroids use.
Methods:
We conducted a retrospective cohort study from 1991 to 2011, using a medico-administrative database from Quebec. Medical billing codes were used to identify PLWH, and we matched them on age, sex, and index date with up to 4 HIV-negative controls. The exposure of interest was the use of corticosteroids, defined as a systemic corticosteroid dispensation lasting at least 20 days. The outcome of interest was hospitalization for severe infection. Crude and adjusted incidence rates ratios of infection were obtained using a random effect Poisson model, and results were stratified by HIV status.
Results:
In total, 4798 PLWH were matched to 17 644 HIV-negative controls, among which 1083 (22.6%) PLWH and 1854 (10.5%) HIV-negative controls received at least one course of corticosteroid. The mean duration of corticosteroids use was 4 ± 4.4 months in PLWH and 1.6 ± 5.5 months in HIV-negative controls. The incidence rate ratio (IRR) for infections associated with corticosteroids use was 2.49[1.71–3.60] in PLWH and 1.32[0.71–2.47] in HIV-negative controls (P value for interaction 0.18). The most frequent infections were pulmonary infections (50.4%), followed by urinary tract infections (26%) and opportunistic infections (10.5%).
Conclusion:
Although our interaction term did not reach significance, the increased risk of infection associated with corticosteroids use was more pronounced in PLWH. However, further research with contemporary data is warranted to confirm if the risk associated with corticosteroids use remains high in PLWH with well-controlled HIV infection.
Key Points
Strength: The major strength of this study is its large sample size of 4798 PLWH and 17 644 HIV- controls, matched for sex and age.
Key findings: We found that the increment in risk of severe infections is greater in PLWH taking corticosteroids than in age and sex-matched pairs who are not.
Introduction
The rate of AIDS-related infections has significantly decreased since the introduction of Highly Active Antiretroviral Treatment (HAART).1–4 According to the World Health Organization (WHO), 680 000 people worldwide died from AIDS-related illnesses in 2020, compared to 1.9 million in 2004 and 1.3 million in 2010. 5 Improvements in antiretroviral treatment have resulted in prolonged lifespans, but a set of chronic diseases has emerged in people living with HIV (PLWH), such as cardiovascular, metabolic, liver, neurocognitive, cancer, and autoimmune diseases.6–8 Several studies have established that PLWH are at increased risk of developing autoimmune diseases compared to the general population.9–12 Prior investigations of a large HIV-positive cohort study in Quebec compared the incidence rate of autoimmune disease to that of HIV-negative controls matched for sex and age and found that in PLWH the incidence rate was 16.14 (14.65- 17.79) per 1000 person-years (PY), compared to 6.44 (5.90-7.02) per 1000 PY in the HIV-negative group. PLWH were more than twice as likely to have autoimmune disease than their matched counterparts. 13
Corticosteroids are the cornerstone of autoimmune disease treatment. Moreover, they are often used as an adjunctive treatment for cancers or certain infections such as severe meningitis, pneumocystis jirovecii pneumonia, all of which appear to be more prevalent in PLWH.14–18 However, corticosteroids use is associated with an increased risk of other infections, which is well documented in HIV-negative populations. Two systematic reviews and meta-analyses estimated the relative risk of corticosteroids-associated infections (CAIs) to be 1.6 IC [1.3-1.8],19,20 with a more pronounced risk observed in people with underlying medical conditions, 19 but these meta-analyses did not include PLWH.
To date, it remains unclear whether HIV status modulates the risk of CAIs. 21 Given the higher incidence of autoimmune diseases and other chronic diseases in PLWH, establishing the safety of corticosteroids used for their treatment is paramount. In this study, we hypothesized that CAIs risk would be higher in PLWH versus an age and sex-matched HIV-negative population.
Patients and Methods
Study Design
We conducted a retrospective cohort study using the administrative healthcare database of the Régie de l’Assurance-maladie du Québec (RAMQ), province of Québec, Canada.
Database Description
Every resident of the province of Québec, Canada, is admissible for universal medical care coverage, of which RAMQ is the unique provider. In 2020, this included about 8.2 million people. 22 The database contains data on medical billing claims and hospitalization discharge summaries. Information is also available on all prescription drug dispensations for subscribers to the public pharmaceutical insurance (including name of drug, dosage, quantity of dispensed medication, and duration of prescription). Pharmaceutical insurance is mandatory in Québec, but there are multiple providers. RAMQ provides insurance for all residents aged ≥ 65, recipients of last-resort financial assistance, and residents who do not have access to a private insurance plan; this represents about 40% of the total Québec population.
Cohort Constitution
HIV infection was identified using ICD-9 codes in physician billing claims (042-044 and Québec-specific ICD-9 7958) and pharmaceutical dispensation of at least one HIV-specific antiretroviral drug. Each HIV-positive patient was matched to up to four HIV-negative patients by age, sex and cohort entry date. The earliest date of the first HIV-specific code or date of the first dispensation for any HIV-specific drug was defined as the cohort entry date for PLWH. HIV-negative controls were assigned the cohort entry date of their matched counterparts. The exclusion criteria were: being less than 18 years old at cohort entry, having no public insurance drug coverage for a year before cohort entry, or prior use of corticosteroids before cohort entry. Patients were followed in the cohort until the occurrence of 1) death, 2) end of pharmaceutical insurance coverage, or 3) the end of the study. The study period was from first January 1991 to 31st of December 2011.
Exposure and Outcome
The exposure of interest was corticosteroids use, defined as a systemic corticosteroids dispensation lasting at least 20 days. Corticosteroids use was considered as time-dependent variable. Corticosteroids dispensation was identified using DIN codes, listed in Appendix 1. A 30-day grace period between dispensations was used to define continuous treatment episodes, meaning that 2 consecutive treatments were considered as the same treatment episode when the gap between the end of the first dispensation and the start of the following one was less than 30 days. In addition, we considered a 7-day lag period at treatment initiation to limit protopathic bias, when an undiagnosed but symptomatic infectious event would generate corticosteroids prescriptions such as prednisone given for chronic obstructive pulmonary disease (COPD) flare-ups, which would inaccurately be ascertained as a CAIs. This lag period also allowed time for the biological effect of corticosteroids to increase CAIs risk. Patients were considered unexposed for 7 days following the start of a corticosteroid dispensation, and dispensations lasting less than 7 days were not considered. The use of other immunosuppressant drugs (such as disease modifying antirheumatic drugs and biological immunosuppressant) were also noted.
The primary outcome was hospitalization for severe infections. Severe infections were identified using ICD-9 and ICD-10 codes in hospitalization discharge summaries. Admission date was considered as diagnosis date and severe infections occurring less than 30 days apart were considered as the same infectious event. The subtypes of severe infections (sepsis, pulmonary, abdominal, joint and tissue, nervous central system, urinary tract, and cutaneous infections) and their corresponding codes are presented in the Appendix 2.
Statistical Analysis
Appropriate descriptive statistics were used to compare baseline characteristics and corticosteroids use in both cohorts. Crude and adjusted incidence rates ratios of hospitalization for severe infection were obtained using a Poisson model. To explore the potential effect modification of HIV status on the risk of severe infections related to corticosteroids use, an interaction term between HIV and corticosteroids use was added into the model. In addition, we also considered a random effect to account for repeated events. All results are presented stratified by HIV status. Due to the limited data on non-corticosteroids immunosuppressants and combined treatment, these exposures were not included in the analysis. Models were adjusted for hepatitis C, alcohol abuse, chronic obstructive lung disease, chronic kidney disease, diabetes, and active cancer, (Appendix 3). A secular trend analysis was also conducted to evaluate the effect of the calendar time variable on the incidence rate of severe infections, given the evolving HIV treatment landscape as well as the optimal access to potent antiretroviral therapy, all of which characterize our study period. 23 The Akaike information criterion (AIC) was used for model selection. All analyses were performed using R software version 1.2.1335.
Ethical Approval and Informed Consent
This research project was approved by the Commission d’Accès à l’Information, and the Ethics review board of the Centre Hospitalier de l’Université de Montréal (CHUM) research center (Approval number 2008-4773). Given the anonymized nature of the data, the need for individual consent was waived.
Results
Characteristics of Study Population
Figure 1 shows the population selection process. We included 4798 PLWH receiving antiretroviral therapy and matched them to 17 644 HIV-negative controls. Baseline characteristics are shown in Table 1. Both groups were of similar age (mean 50 years old). Mean duration of follow-up was 6.3 years in PLWH and 4.9 years in the HIV-negative controls. Alcohol abuse was more prevalent in PLWH (5.8% vs 1.2%). At baseline, PLWH had more prevalent comorbidities such as chronic kidney failure (1.2% vs 0.3%), cancer (1.6% vs 0.27%), chronic obstructive lung disease (7.3% vs 2.9%), hepatitis B (1.8% vs 0.02%) and hepatitis C (3% vs 0.02%). AIDS-defining conditions were present in 19% of PLWH.
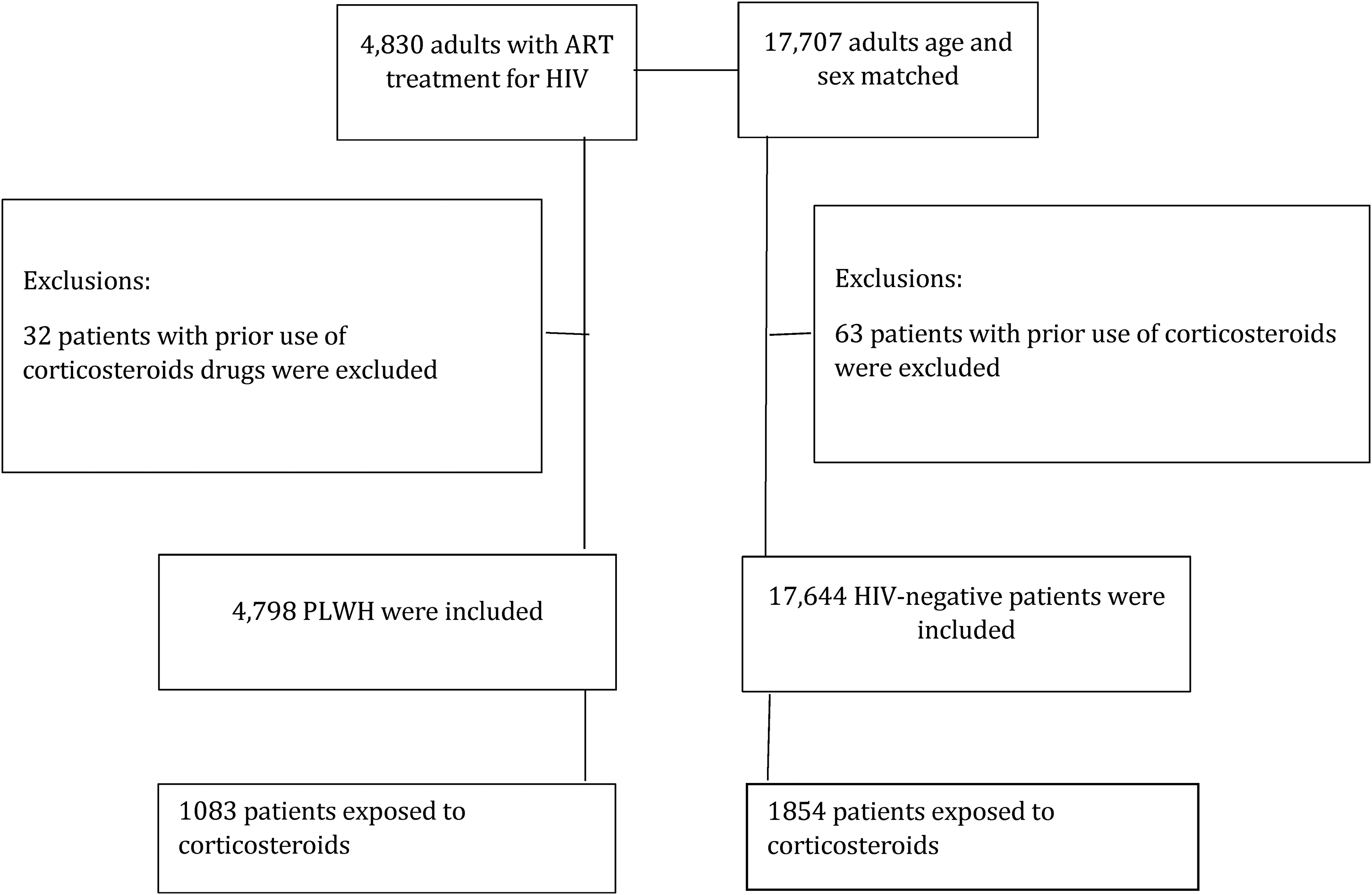
Flow chart of study participants.
Baseline Characteristics of Study Participants.

Unless stated otherwise, numbers in table are n, %.
Baseline characteristics are defined in the year prior to index date.
SD: Standard deviation, IQR: Interquartile range.
*Follow up duration calculated in patients exposed to corticosteroids.
**AIDS defining conditions at baseline or within the year prior cohort inclusion.
Corticosteroids use
Significantly more PLWH (1083, 22.6%) than HIV-negative controls (1854, 10.5%) received at least one course of corticosteroids (p < 0.001). Table 2 presents corticosteroids use in both cohorts. Median time between cohort inclusion and corticosteroids use was 3.9 years [1.3-7.2] in PLWH and 4 years [1.9-7.9] in HIV-negative controls. Mean duration of corticosteroids use was 4 ± 4.4 months in PLWH and 1.6 ± 5.5 month in HIV-negative controls (p < 0.001). Prednisone was the most commonly used corticosteroids (82% in PLWH vs 75% in HIV-negative controls), followed by dexamethasone (15% in PLWH and 10% in HIV-negative controls). Mean daily corticosteroid dose (prednisone equivalent) was 27.8 mg in PLWH and 34 mg in HIV-negative controls.
Corticosteroids Use.

Unless stated otherwise, numbers in table are n, %.
PE: Doses are in prednisone equivalent.
Denominator is the number of patients exposed to corticosteroids in HIV positive (1083) and HIV-negative (1854).
Incidence Rate and Incidence Rate Ratios of Severe Infections
In all, 1400 patients were hospitalized for severe infections (1048 in PLWH and 352 in HIV-negative controls). The most frequent infections were pulmonary infections (50.4%), followed by urinary tract infections (26%) and opportunistic infections (10.5%). Table 3 displays crude and adjusted incidence rate ratios of severe infections according to corticosteroids use, stratified by HIV status. PLWH exposed to corticosteroids had a higher incidence of severe infections than unexposed subjects (14.7 cases vs 5.9 cases per 1000 patient-years), while incidence of severe infections in HIV-negative controls was very low (0.005 cases per 1000 patient-years in those exposed to corticosteroids vs 0.004 cases in the unexposed). The IRR for infections associated to corticosteroids use was 2.49 95% CI [1.71-3.60] in PLWH and 1.32 95% CI [0.71-2.47] in HIV-negative controls. The evolution of severe infections incidence rate according to corticosteroids use during the study period in both groups are presented in a Table 4. The rate of severe infections in PLWH exposed to corticosteroids during the study period remains much higher compared to exposed HIV-negative controls.
Crude and Adjusted Incidence Rate Ratios for any Severe Infections According to HIV status and Covariates.
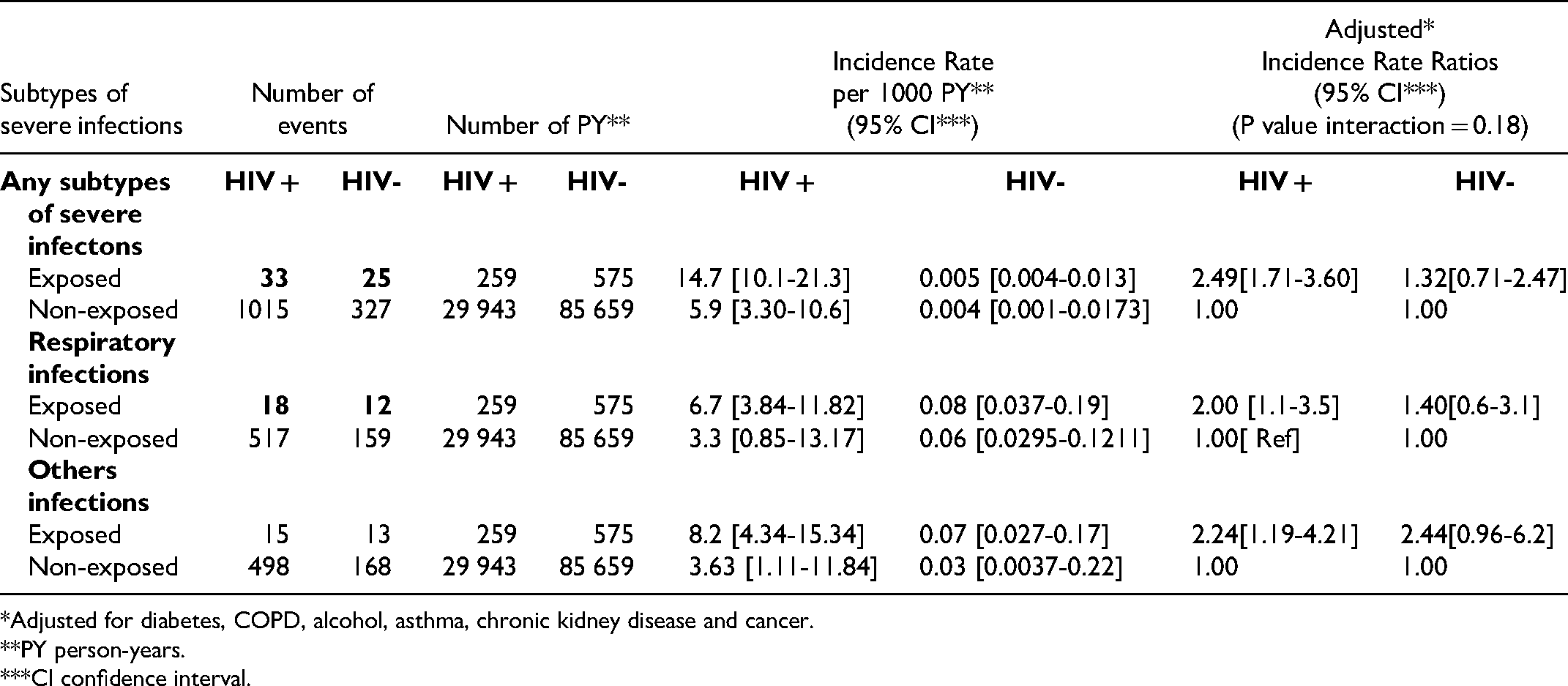
*Adjusted for diabetes, COPD, alcohol, asthma, chronic kidney disease and cancer.
**PY person-years.
***CI confidence interval.
Crude and Adjusted Incidence Rate Ratios for any Severe Infections According to HIV status and Calendar Period.

Adjusted for diabetes, COPD, alcohol, asthma, chronic kidney disease and cancer.
*The strata 1991-2001 represents a combination of 1991-1996 and 1996-2001 periods, as one of the cells had very small number of severe infections (<5).
**PY person-years.
***CI confidence interval.
Discussion
We found that PLWH taking corticosteroids have a higher risk of severe infections than PLWH not taking corticosteroids (IRR 2.49 [1.71-3.60]), whereas the difference in the IRR associated with corticosteroids use in HIV-negative controls (corticosteroids users vs non-users) was not statistically significant (IRR 1.32 [0.71-2.47]). The incidence rate of severe infections was higher in PLWH from 1991 to 2001 and significantly decreased from 2001 to 2011.
Several lines of evidence have suggested that PLWH use corticosteroids at a higher rate than the general population, due to their comorbidities and autoimmune disorders.13,24,25 It has been shown that clinicians avoid prescribing corticosteroids to PLWH out of concern for adverse outcomes. 26 Drug-drug interactions between HAART and corticosteroids or other medications can explain the increased risk of severe infections in PLWH.27–30 The temporal trend observed is likely the reflection of declining rates of AIDS events associated to constant progress observed with HAART treatment, their indications, toxicity and availability, as noticed by other authors.2–4
Very few observational studies have reported corticosteroids safety profiles in PLWH, making comparison difficult.9,11 Two descriptive studies found similar trends, despite major limitations due to small sample sizes and the absence of comparator groups.9,31 A literature review of cases reports on systemic erythematous lupus (SLE) and HIV included 55 PLWH with SLE. The median age was 32 years old [23-29] and median CD4 count of 353/mm3 [214-560.] Fifty-three patients received treatment for SLE of which 52.2% were administered corticosteroids. An AIDS related event was identified in 66.7% of the 15 patients who died, but the authors did not provide neither the proportion of infections among corticosteroids users nor information about the type of infection. 31 Another cohort study included 52 PLWH with autoimmune diseases, followed from 1983 to 2013. Authors identified 18 patients who were treated with corticosteroids, 11 of which developed infections. Respiratory infections were the most incident infections reported in 5 patients. 9
Several clinical trials on the use of corticosteroids as an adjunctive treatment in HIV opportunistic infections have also been published in the literature,32–35 but they only considered CAIs as secondary endpoints, and thus lacked power. These studies tended to report more contradictory results than the observational studies, likely due to their inherent limitations (sample size, short period of exposure, and insufficient reporting of adverse effects). A double-blinded randomized controlled trial on the use of dexamethasone for tuberculous meningitis enrolled 98 HIV patients, 44 in the treatment group and 54 in the placebo group. The treatment group received dexamethasone intravenously for 4 weeks and orally for 4 additional weeks. Bacterial infections were reported in 5 patients in the dexamethasone group and 7 patients in the placebo group. 33 Another discordant result was reported by Meintjes et al in a double-blinded randomized controlled trial on prednisone and tuberculosis associated immune reconstitution inflammatory syndrome (IRIS). In this trial, 120 PLWH received prednisone (at a dose of 40 mg per day for 14 days, then 20 mg per day for 14 days) and 120 PLWH received placebo. The median age was 36 years-old (30-42). The median CD4 was 51 cells/ul (27-84) in the prednisone group and 49 cells/ul (23-88) in the placebo group. Severe infections were mostly observed in the placebo group (11/119 (9.2%) versus 18/119 (15.1%) RR 0.61 95%CI [0.30-1.24]). 34 Beardsley et al 32 conducted a multicentric double blind randomized controlled trial using dexamethasone for the treatment of HIV associated cryptococcal meningitis. All patients in the dexamethasone arm received 0.3 mg / kg of this molecule initially, then decreased doses for 6 weeks. A total of 21 patients (48%) had developed infections during follow-up in the dexamethasone group, compared to 11 (25%) in the placebo group (p = 0.003). 32 Thus, one of three clinical trials appears to corroborate our findings.
A similar trend for increased risk of infection in HIV-negative controls exposed to corticosteroids was found, though this did not reach significance, likely due to the small number of events in this group. The incidence rate ratio for severe infections was 1.32 [0.71-2.47] in the exposed group. The risk ratio of infections is well documented in non-HIV population and was estimated to be at 1.6[1.3-1.9] in a systematic review dated from 1989. 19 More recently, another systematic review and metanalysis in non-HIV patients with rheumatoid arthritis reported a RR of 1.67 (1.49 −1.87) from 42 included observational studies, which is relatively close to our findings. 20
Strengths and Limitations
To our knowledge, this is the first retrospective cohort study with a large sample size and an HIV-negative control group to estimate the risk of severe infections associated with corticosteroids among PLWH. The long follow-up period allowed observation of the long-term effects of corticosteroids. In contrast to past reports, we considered the possibility of repeated events in the statistical analysis. The choice of severe infection requiring hospitalization is specific which reduced information bias.
However, several limitations need to be considered when interpreting these findings. First, the comparability of the two populations for measured confounders may have been extremely limited, given the high proportion of AIDS events in PLWH and differential monitoring between PLWH and HIV-negative controls. Our results were not stratified by CD4 count and viral load. These two factors are strong predictors of AIDS-related events and would have helped to identify the infection risk at baseline and permit a sensitivity analysis according to CD4 count and viral load. Second, corticosteroids indications are heterogeneous and the infectious risk (and subsequent interaction associated with HIV) may have differed from one indication to another. Corticosteroids indications were not clearly mentioned in the database, and some patients may have been exposed to corticosteroids for various reasons, such as immune reconstitution inflammatory syndrome (IRIS) and the severe infections observed in our study could be the result of immune reconstitution. This scenario appears less likely as IRIS generally develops 3 months after HAART introduction and the median time between cohort inclusion and corticosteroids exposure was 3.9 years [1.3-7.2]. Further, important confounders such as smoking habits, disease severity, injectable drug use, and socioeconomic status were not controlled for, and this may have led to residual confounding bias. As hospitalization for infections is a rare event, this study may be underpowered, especially in the non-HIV group. Third, our study covers a period from 1991 to 2011. PLWH in the early 90s weren't systematically treated according to modern recommendations, and they may therefore have been at an increased risk of infection at baseline.
Conclusion
Although our points estimate suggest a more pronounced risk of infection associated with corticosteroids use in PLWH, confidence interval (as well as P-value for interaction) remain large in both groups. Therefore, we cannot conclude with certainty that the additional risk of serious infections conferred by corticosteroids exposure is larger for PLWH than for HIV-negative controls. These findings warrant further research with contemporary data and a larger control group to verify if the CAIs risk remains high in PLWH with well-controlled HIV infection.
Footnotes
Acknowledgments
JJD wrote the protocol draft, planned the study, performed the analysis and wrote the manuscript first draft. Corresponding author MD reviewed the protocol draft, the final manuscript and planned the analysis. YJ and LS participated in the analysis. ML planned the study and MMP reviewed the final manuscript.
Disclosure of Conflicting Interests
The Authors declared no potential conflicts of interests with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article. MD is supported by a clinician researcher salary award from the Fonds de Recherche du Québec – Santé.
Data Availability
Authors had full access to data and take responsibility for the integrity of the data and the accuracy of data analysis.