
Abstract
Background:
Although the concept of treatment as prevention has generated optimism that an AIDS-free generation is within reach, the success of this approach centers upon early diagnosis and linkages to care for people living with HIV. Unfortunately, people continue to present for HIV care at late stages of disease and HIV-related stigma has been recognized as the major impediment to HIV prevention and treatment efforts. Given the relevance of addressing stigma to improve access and utilization of HIV services among men, this secondary analysis assessed perceptions of heterosexual men in HIV-related stigma on HIV testing and ART services in Blantyre District.
Methods:
Purposive sampling was done with maximum variation which included men with unknown statuses, newly diagnosed with HIV infection and not yet on ARVs and those with HIV infection on ART. These participants were varied according to age and area of residency and included men from urban, semi urban and rural areas. Health care workers were included depending in the participation in the provision of HIV services. Eighteen (18 IDIs) and sixteen (16) KIIs were done at private facilities and a total of twenty (20) IDS and seventeen (17) KIIs interviews were conducted at public facilities and fourteen (14) FGD were conducted at public facilities as well. The data were collected from January to July 2017 and March to September 2018.
Results:
Men perceived that there are barriers and enablers that influence men from accessing HIV testing and ART services. These factors include individuals, family, community and workplace. The surroundings can be a person, community and a family and it plays an integral part in ones’ decision to get tested or initiate on ART. At all these levels, men would navigate the options of accessing the services while risking stigma and discrimination.
Conclusion:
HIV-related stigma exists and impedes access to HIV testing and ART services in men. Men preferred private hospitals to public facilities because of their ability to maintain respect to privacy and confidentiality to their client's. Imitating these policies into the public hospitals can help to improve the perception of HIV-related stigma in heterosexual men.
Background
The HIV and AIDS epidemic is associated with stigma and discrimination. 1 Stigma comprises negative attitudes and beliefs about people living with HIV and it is the prejudice that comes with labelling an individual as part of a group that is believed to be socially unacceptable. 2 Perceptions of HIV-related stigma are either actual or potential experiences of diminished social acceptance, opportunity and negative shift in how others perceive the person living with HIV. 3 These perceptions include segregation, prevention from access to something or service resulting in unfair and unjust treatment of an individual based on his or her real or perceived HIV status, limitation of expression, marginalization as well as being judged. 3
Although the concept of treatment as prevention has generated optimism that an AIDS-free generation is within reach, 4 the success of this approach centers upon early diagnosis and linkages to care for people living with HIV. 4 Unfortunately, people continue to present for HIV care at late stages of disease 5 and HIV-related stigma has been recognized as the major impediment to HIV prevention and treatment efforts.4,6
The factors that drive stigma include association of HIV infection with behaviours such as homosexuality, drug addiction and prostitution, 4 availability of a client at an HIV-related clinic, exposure to people living with HIV (PLWHIV) and the level of education on HIV transmission, prevention and treatment. 7
Perceptions of stigma occlude disclosure of an HIV-infected status because it brings out self-blame, fear of rejection, communication difficulties and a desire to protect the other person. 8 Fear of stigma impedes access to health facilities for testing or treatment and is a reason for delaying access to care until one is extremely sick. 8
The strategies for mitigating stigma include home-based HIV counselling and support for PLWHIV, 9 increasing the general public tolerance or healthcare provider's willingness to treat PLWHIV minimizes HIV-related stigma by changing individual level fears, attitudes or behaviours, 9 provision of information, skills building like coping with anxiety skills 10 and problem-focused and emotion-focused strategies to mitigate the negative consequences of stigma. 9 Problem-focused strategies include selective disclosure, disengagement, affiliating with similar others, seeking social support and to lesser extent activism. 9 These prevent internalized stigma by revealing one's status to only those that would be giving social support and encouragement. Emotional-focused strategies include positive reappraisal, distraction, religious coping, misidentifications and acceptance and these provide distracters that help one to focus on positive thinking and not negative thinking. 9
HIV-related stigma is one of the reasons for the low uptake of HIV services by men worldwide and men are the most affected with it. 11 Lack of inclusion of men in HIV services has consigned HIV as a disease that women bring in a relationship and need to manage. 12 Men are impassive in health seeking resulting into limited contact with health services which contributes to the lack of prioritization and uptake of health services. 13 Men have further been systematically sidelined in the services and programs that are implemented by donors because of the female gender oriented direction the services have taken. 14 Stigma if not addressed in the provision of HIV services among men may lead to delays in HIV testing, poor engagement with ART services and non-disclosure to sexual partners, lowered adherence to treatment and care regimens. 14 Although the Malawi health services have addressed issues related to stigma, 12 there remains disparities between men and women in access and utilization of HIV services.12,15
Given the relevance of addressing stigma to improve access and utilization of HIV services among men, this secondary analysis assessed perceptions of heterosexual men in HIV-related stigma on HIV testing and ART services in Blantyre District. The information from this study will help facilities improve on strategies for mitigating stigma and will provide policy makers with information for reinforcing interventions for eradication of HIV-related stigma which will optimize access and utilization of HIV services among men in Malawi.
Conceptual Framework
The study was guided by William. L. Holzemer et al. Model namely “Model of the dynamics of HIV/AIDS stigma.” 16 According to this model, stigma in the past years looked much on how others view the stigmatized person forgetting the social process that can only be understood in relation to broader notions of power and dominion. 16
The framework suggests that HIV stigma impacts people's decision to get HIV-tested, decisions to disclose their HIV status, adherence to HIV medications and their day-to-day quality of life. “HIV stigma also impacts the quality of work-life for health care professionals, as they are perceived by some to be contagious, since they work with HIV-positive patients. 16
In our study, we included and exploration of the men's perception on HIV-related stigma especially on the factors that influence occurrence of HIV-related stigma at individual level, family level, community level as well as work place. We also assessed their perceived consequences of HIV-related stigma in heterosexual men.
Methods
Study Design
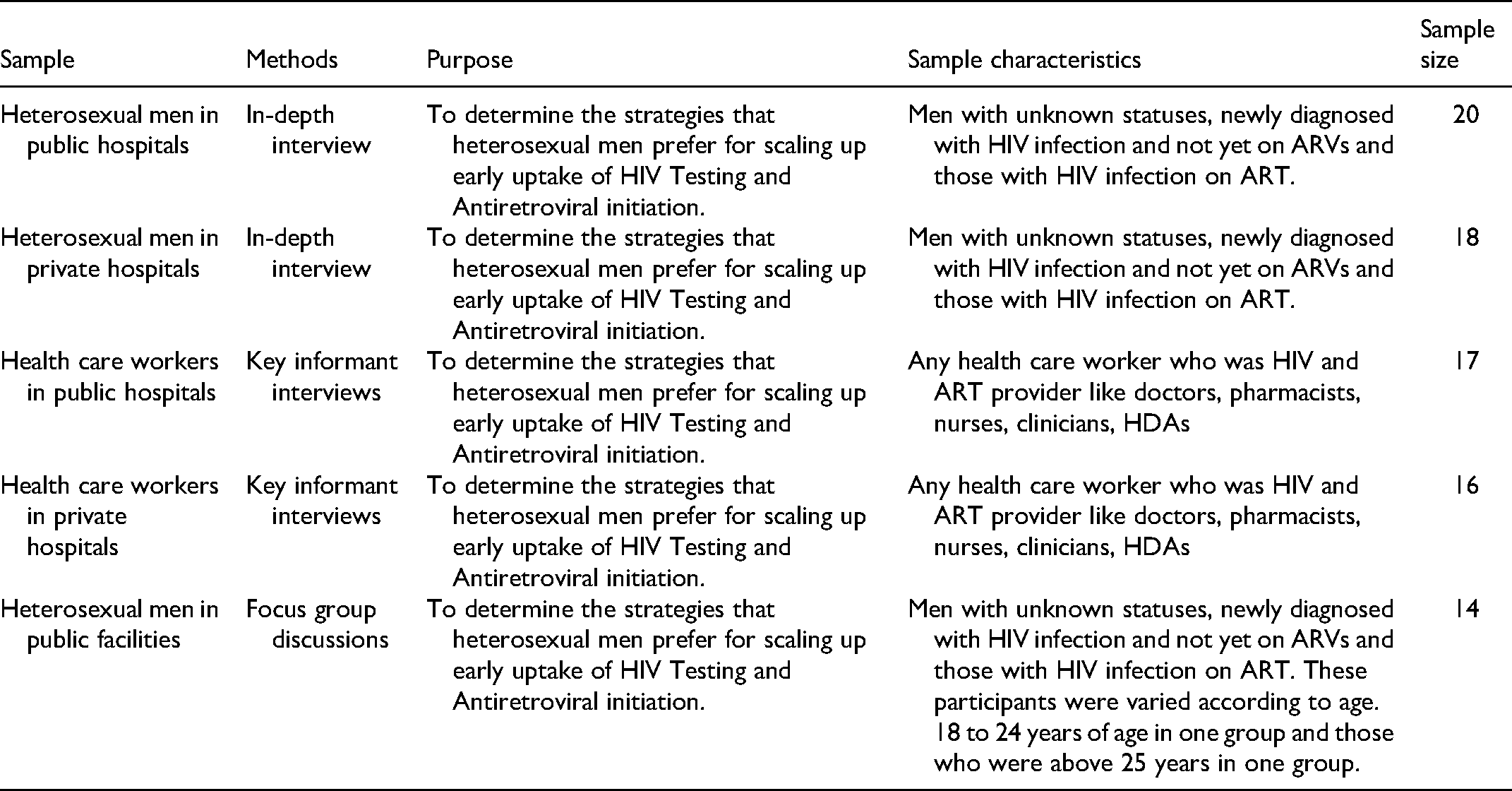
This is a secondary data analysis on a dataset from a qualitative descriptive study. The main study was “Strategies for Early Access to HIV Services by Heterosexual Men in Blantyre, Malawi Version 5.0, dated 8th April 2019.” COMREC number P/06/18/2430 and the details of the primary study are published.17,18 The aim of the study was to determine the strategies that heterosexual men prefer for scaling up early uptake of HIV Testing and Antiretroviral initiation.
Study Setting
This was a qualitative study conducted in 7 public and 10 private health facilities in Blantyre, Malawi from January to July 2017 and March to September 2018 respectively. From the public facilities, it included 2 health centers from urban Blantyre (Ndirande and Chilomoni), 2 health centers from semi-urban (Mpemba and South Lunzu), 2 health centers in rural Blantyre (Madziabango and Lirangwe) and a tertiary hospital (Queen Elizabeth Central Hospital). HIV testing and ART services in the public facilities are done by Blantyre District's HIV and ART Coordinators, ART Clinicians/Nurses, Human Immunodeficiency Diagnostic Assistants (HDAs) and Human Immunodeficiency Testing Service (HTS) providers. HIV testing is done on a daily basis in all the health Centre's excluding ART services which are assigned specific days to be dispersed. Only the tertiary hospital provides both HIV testing and ART services on a daily basis.
In private settings, it included 2 clinics from rural Blantyre, 3 clinics and 1 mission hospital from semi-urban and 3 clinics and 1 private hospital from urban Blantyre, Malawi. The HIV services are done by nurses, doctors, lab assistants, pharmacist and are usually open for 24 h depending on the time they close the hospital for the day.
Sample Size
Purposive sampling was done with maximum variation 19 which included men with unknown statuses, newly diagnosed with HIV infection and not yet on ARVs and those with HIV infection on ART. These participants were varied according to age and area of residency and included men from urban, semi urban and rural areas. Health care workers were included depending in the participation on the provision of HIV services. Eighteen (18 IDIs) and sixteen (16) KIIs were done at private facilities and a total of twenty (20) IDS and seventeen (17) KIIs interviews were conducted at public facilities and fourteen (14) FGD were conducted at public facilities as well. The sample size was adequate as it gave more rich information for both the young generation as well as the older generation.
To expand the possibility of multiple sources of information in the study, men of different individualities such as age, residency, education level, marital status, religion, occupation, HIV status were encompassed in the participants, to achieve thorough variation.
Data Collection
All audio-recorded interviews were done at the health facility at a private place. The FGDs were divided according to age and interpreted into one FGD with younger men with an age bracket of eighteen to twenty-four (18-24) years and the other with older men with an age bracket of 25 years and above at each site. This was done in order to promote participation which could have been limited if we had mixed younger and older men in one group. De-identified data on “Perceptions of Heterosexual Men on HIV Related Stigma in HIV Testing and ART Services in Blantyre District” were extracted from the study “Strategies for Early Access to HIV Services by Heterosexual Men in Blantyre, Malawi.” This was taken from the principal investigator of the study (Supplementary Files 2and 3). Semi-structured open-ended IDIs, FGDs and KIIs guides were used to collect data from the eligible study clients and health workers, respectively. Data collection tools were designed in both English and Chichewa (Supplementary Files 2 and 3). Data collection tools had two parts, part A which contained demographic data while part B contained guiding qualitative questions to elicit answering the intended question of “Strategies for Early Access to HIV Services by Heterosexual Men in Blantyre, Malawi.” The same guides were used to facilitate secondary data analysis in “Perceptions of Heterosexual Men on HIV Related Stigma in HIV Testing and ART Services in Blantyre District.” Before conducting the study, the interview guides were pre-tested and modifications were made based on the lessons learned from the pre-testing exercise and all data collectors that were recruited for the study were oriented to ensure data quality. The orientation included instruction on interviewing techniques, a detailed review of interview guide content and mock interviews between enumerators. All FGDs, IDIs and KII were digitally recorded using 2 digital recorders and then simultaneously transcribed and translated verbatim into English by the research Assistants. There were multiple levels of checking for quality on completeness before final proof reading of the transcripts against the recorded interviews.
Data Analysis
Thematic data analysis using step by step guide was used in this study [13]. The analysis of the findings was guided by the Holzemer model of dynamics framework. The researcher familiarized with the data by reading and re-reading transcripts at least 3 times. This helped the researcher to understand the depth and breadth of the content and also got the meaningful segments and the essence of the data. The objectives and model assisted in the deductive coding of the data. During the process, notes and markings were made within the transcripts for coding. Once the list of codes was made, the researcher reread the transcripts to identify similar codes that were organized under a theme. A set of similar codes that formed a coherent pattern formed a theme. The transcript was then reread to identify additional themes that initially were missed. Themes were reviewed to assess if indeed they were relevant to the themes or subthemes. When all the themes and subthemes were organized, the researcher then defined and named each theme accordingly ready for analysis. A discussion with the main study principle investigator was made throughout the analysis as a quality measure.
Ethical Considerations
Prior to using the secondary data, permission was obtained from the principal investigator of the study and all the data was fully available and granted without restriction for academic use (Supplementary file 2). This secondary analysis protocol was approved by College of Medicine Research Ethics Committee (CoMREC) (CoMREC number P.05/20/3066).
The primary study was approved by CoMREC (COMREC number P/06/18/2430) and the consent forms and interview guides were translated into Chichewa, the local language, to eliminate language barriers and preserve consistency across users. All focus group discussions were conducted in Chichewa. In-depth interviews with health care workers were in both Chichewa and English depending on a health care worker preference and with clients in Chichewa. The consent document was either read or given to the participant to read. An illiterate participant was asked to thumbprint the consent form after it has been read to him or her in the presence of a literate witness. The purpose of the study was discussed, the outline and the risks and benefits of participation, the duration of the study and procedures in the consent forms. Finally, the participants were given a copy of the consent form to take home.
Results
A total of 18 IDIs and 16 KIIs were done at private facilities and a total of 20 IDS and 17 KIIs interviews were conducted at public facilities and 14 FGD we conducted at public facilities as well. The qualitative research provided more insights on the definition and description of HIV-related stigma, consequences of HIV-related stigma and ways of mitigating HIV-related stigma in Blantyre district.
The results have been analyzed following the model of dynamics and have been presented according to this framework while respecting study objectives.
Characteristics of Men in the Public Facilities
The median age of the men was 27 [IQR 21 to 35]. Most men were unmarried, had a primary level of education which spans from Grade 1 to Grade 8 and were self-employed. Of the 133 men, only 32 had not taken an HIV test before, and of those living with HIV infection, only eight were not on ART (Table 1). Of the participants we approached, five men for in-depth interviews and seven men for FGDs refused participation and cited time factor as a limitation.
Summary of Methods.
Characteristics of Men in Private Facilities
The median age of the men was 27 [IQR 21 to 35]. Most men were married, had a tertiary level of education, and were employed. Of the 18 men, only 2 had not taken an HIV test before, and of those living with HIV infection, only one was not on ART (Table 2).
Characteristics of Participants in the Public Facilities. 20

Characteristics of Health Care Workers
Public Facilities
On the 17 health care workers, 15 were male and their median was 38 years old. Interquartile range (IQR) was 32 to 48 years old. There were nine (9) HDAs, four (4) nurses, two (2) Medical Assistants, one (1) HIV testing Coordinator, and one (1) ART coordinator, respectively. One health care worker refused participation and cited time factor as a limitation (Table 3).
Characteristics of Participants in the Private Facilities. 20

Of the 16 health care workers, 8 were females and their median was 38 years old. Interquartile range (IQR) was 32 to 48 years old. There were one (1) HDAs, two (2) nurses, six (6) medical officers, two (2) pharmacists, three (3) lab technicians, one (1) ART clerk and one (1) social worker. One health care worker refused participation and cited time factor as a limitation.
Factors That Influence Occurrence of HIV-Related Stigma
Agent
According to the model of dynamics barriers and enablers are factors related to an agent. An agent can be a person, family, community as well as a work place that influences men from accessing HIV testing and ART services. According to the model, the surroundings can be a person, community and a family and it plays an integral part in ones’ decision to get tested or initiate on ART.
Factors Related to the Individual
Most men put themselves in an ‘‘if’’ situation before thinking of going for HIV testing and before initiating on ART. Looking at the responses most men consider what the future will hold more especially what would become of them when they go for VCT. The following excerpt shows the self-stigma that a man portrayed over his decision to take an HIV test. What if I am going to be found with HIV in my body, it means that my wife is going to think that I have been going around with different women out there (Private clinic 3).
Family
Family can be a significant source of stress for men when found with HIV. Families experience HIV-related stigma because of their association with infected family members. The stigma comes from the risk behaviours that bring the disease such as commercial sex. Participants from both private and public clinics shared equal sentiments on the family as a contributing factor to one's experience of HIV-related stigma. And again there are some people instead of discussing their things in their homes they end up discussing your HIV status by telling the family members that you are on ARV's. People will be talking behind their back by saying that ‘that family are on ARV's’ (FGD, Ndirande health Centre 18-24years)
Community
The communities that men live in have not been very accommodating when it comes to issues on HIV. Participants from both private and public facilities expressed concerns about how a community treats an individual who is living with HIV. The closeness of the facilities to their homes does not make things easier for the men either. Once people find out why one usually visits the hospital it becomes an issue. In the community men are scared that others will know and will discriminate against them so they would rather not start treatment. In some communities, when you are on treatment you are a victim and they don't treat you like part of them. You are like the black one. (Private clinic 6)
Workplace
In the workplace, men living with HIV may suffer stigma from their co-workers and employers. Most people felt that they are going to be denied work opportunities because of equating HIV infected status to ill health. Men would ponder over whether they need to reveal their HIV infected status once employed and would linger over the question ‘should I tell my employer about my status?’. Men fear the reaction that will come from an employer and at most are afraid that it may cost them their job especially when they need to absent themselves from work to meet their ART appointment needs. It was noted that in instances where there is a clinic at the workplace then issues of disclosure are obscured especially for those that access their ARVS from their workplace. Maybe other people are HIV positive at the company and then if there is a clinic at that company most of the times it becomes so hard to keep secret of those who are HIV positive and that is what I have observed so far and that's my thinking anyway (Private clinic 5)
Stigma Influenced by the Health Care System
Participants stated that the health care system does not give much reassurance over the fears most men have when they want to access HIV services. Men are met with unintended disclosure of their status just by the setting where these services are provided which is a primary setback in public facilities. Lack of privacy was one of the major concerns men raised especially in public facilities. They described public facilities to be of inferior quality when it comes to privacy and confidentiality as most of the public facilities are too open. People are always everywhere where everyone can see and understand what services are being provided. these days were established that Tuesday and Thursday people are supposed to collect drugs for example, I happen to pass by here and I have a girlfriend who take medication but didn't tell me, you will know that oh she is also amongst the group, and this one too and this one too and the other thing they have identification. They are given peg cards. (FGD, Mpemba health centre 18-24)
In general, in public hospitals they lack privacy so they fear and lack of time. Men are always on the move. And again you have to include self-stigma as well which comes about because of your own making (Private clinic 3)
Some participants recommended private facilities on how they deliver their services. Most of the men preferred private hospitals to public hospitals because of how the health care workers respect and value them when offering their services. Here is what they had to say There is always privacy on that issues of HIV and AIDS and you will not know that the client is here for HIV testing because they always maintain the privacy issue here. When I say privacy it's the way we are treated and their hospitality, they welcome us with warm hands and that's how I can put it. (Private clinic 3)
Some men went further to differentiate public and private hospitals as contributing factors to their reasons for not being able to gather the courage to go for HIV tests and initiate ART. Most men don't like going to public hospitals because they are most congested and lack privacy. Men want to do things at their own time and free will but the conditions they meet for them to get tested personally were not meeting their innermost peace. Here are some of the responses they had to give. There is always congestion in the public facilities so there are some people who most of the times are shy to go to the public facilities to get the drugs hence coming here to the private clinics to get the drugs. (Private clinic 7)
The fundamental facilities where HIV testing and ART services were provided from were reported suboptimal for promotion of access to the services among men. Most of the facilities were close to the road where most people pass, close to another room which is not meant for HIV services thus could be seen by those that are there for other illnesses and also most of them were near markets hence visible to the masses or business partners. The lay out of this hospital since one is able to see who is on the queue waiting to go HIV testing and this makes girls to start thinking that the client is already on ARV's (FGD, Mpemba Health Centre.18-24)
For example, where they do the testing it is near the road and also near where some women seat when they leave the hospital and they can clearly see what they are with different kit saying look I was tested with that kit but they are testing him with another kit for the second time; people will just conclude that maybe he has been found positive. (FGD,Mpemba Health centre. 18-24)
Participants further described how the rooms where HIV services occur have no measure to conceal activities happening in the room let alone visibility of one entering and accessing such services. Some places do not have a conducive environment and even if they do it inside the rooms from outside everyone can see everything that happens in that room and they can notice that the person entering into that room is going there for this reason even at a place where we offer the ART clinic is easily noticeable by people (FGD, Mpemba Health Centre. 25 years above)
Some men complained that health workers responsible for HIV testing and ART services were not to be trusted that they can disclose their status to other people. To avert that type of stigma hence men patronize private facilities. And also as I said, sometimes service providers of this hospital go around in the villages, they talk don't just see that guy he was found with the virus (IDI,Madziabango Health Centre)
Perceived Consequences of HIV-Related Stigma
HIV-related stigma among men living with HIV and AIDS has been associated with many negative consequences. These factors include isolation, shame and fear.
Isolation
Men stated that secondary to living with HIV, they may not be able to associate with others for fear of being stigmatized. As such, participants preferred to shun from an HIV test for them to avoid being isolated. A lot of men are always anxious and we always doubt that we can be moving freely in this area more especially if we are found to be HIV positive and people can know about our HIV status. (IDI,Chilomoni Health Centre)
Shame
A painful feeling of humiliation because of HIV status if it turns out to be positive was raised among the participants, where guilt is primarily associated with a belief that one has acted in a transgressive manner, violating a law or social norm and shame. It is often proposed and operates on one's being: it is less about what one does and more about who one is, and how this might stand in relation to a person's awareness of how others perceive them. The act of attending a clinic for a test can be shaming in itself, in that the person perceives their attendance at the clinic for testing serves as a confirmation or admittance that they warrant the suspicion that they might be infected even looking at what HIV is perceived out there in the communities. Men are usually shy to be seen in public especially with issues that are private and confidential like HIV-related issues. They have this feeling that once they are discovered then everyone will know about their status and will be the talk of the town. He does not want to be seen by people that he is on ARV's for fear of being publicized and it will be a very shameful thing for him because these people will start to talk and spread the news to the public (IDI, Ndirande Health Centre)
Some men went further to describe the kind of shame men faces depending on the environment they come from and also the facility environment, they gave their example Sometimes it can be as a result of the place when that man lives, for example, will talk more of myself, I stay at my wife's place so for me to be found to be HIV positive whilst staying at that place, it will be very difficult and this will bring shyness in the process because people will be saying a lot of things behind my back by saying that have you seen that Mary father? He has HIV and I will become shy in the process because of the status and this comes in because of the place which one lives or stays at that particular time or maybe if the man is staying at a certain plot or he is renting at a certain place, people will be talking a lot of things behind his back by pointing at him and that is the reason why we men just stay without accessing the HIV testing. (FGD, South Lunzu Health Centre. 18-24)
There is however a different notion from what participants from public hospitals said to what participants from private hospitals said. Most men expressed satisfaction with the kind of treatment they get from the private facilities. They expressed loyalty, respect and privacy from their service providers and they did not see any reason why they would be ashamed to come to the hospital to get tested and even start on ART when they are found HIV positive. Here are some of the comments they had to make I should say I have been handled professionally or ethically including privacy and the like and nobody knows what I am so far that I give them credit. You can get several people with different illnesses out there but you are taken into a private room like this one and you and the clinician himself discuss the matters arising and when going back say for example you have been given the drugs and if you have something like a good container he tries to find one so that as you are leaving this room nobody should be able to know what has been discussed inside the room or what has taken place. (Private clinic 4)
Fear
Some participants expressed an unpleasant emotional feeling they may have once they find out that they are HIV positive. Lack of knowledge about HIV can lead to fear which can increase stigma whether in community or families. Some men conveyed apprehension that a positive HIV test would undermine their ability to support a family as they may not stay healthy which they felt was necessary to be successful in all other areas of their lives. They questioned the impact of HIV and their ability to find female partners and be heads of their households at all. Those married men fear to go out there and do the testing because they feel like their marriages will end in the process after being found to be HIV positive (Private clinic 3)
Discussion
The study explored perceptions of heterosexual men on HIV-related stigma in HIV testing and ART services in Blantyre, Malawi. Men perceived that stigma occurred at the individual, family, community and workplace level. All of these act as a trigger and may play a role in one's decision to access HIV testing and ART services. At all these levels men would navigate the options of accessing the services while risking stigma and discrimination. Men also perceived consequences of HIV-related stigma like shame, fear and isolation.
Our findings that privacy is critical to accessing HIV services by men is consistent with an earlier study from 2013 where they highlighted that Health care workers gossip about a client HIV tests result because the person tested positive. 21 Similarly, a study done in Ethiopia reported incidence of gossiping and showed that health care workers stigmatization is decreased by increased knowledge, education and training on HIV and AIDS. 22 This implies that privacy is paramount and needs to be strengthened with assistance from human rights activists to combat such issues. Educational activities should highlight teaching on ethics and healthcare law with a clear understanding of patient's rights. 22
We found that family members experience HIV-related stigma because of their significant other. This was also earlier reported in a study that highlighted that family members were being discriminated because of ones’ HIV status 8 and because of that many participants preferred not to disclose their status to anyone in an attempt of protecting them from HIV-related stigma. 8 However this proved to be a problem when one has visible signs associated with HIV infection. 23 Additionally, it has been noted that some families with HIV-infected member are still ashamed of having an HIV-infected family member. 23 This underscores the continued existence of stigma irrespective of the progress made in HIV treatment and survival. Notably, a study done in Malawi, Zimbabwe and Zambia reported that when there has been disclosure of an HIV status, family members offer support to PLWHA. 24 This implies that, even though there is a positive feedback on how families support each other in some parts of Malawi, there is still stigma within the family members when one is found with HIV infection.
Our findings show that employees are afraid to disclose their HIV status because of the reaction they may get from their bosses. These findings are consistent with the findings reported by Mbokazi et.al. in 2020 where they highlighted that men feared losing their jobs which presents a difficult task for them on how to balance the competing interest of their health needs against their economic needs. 25 There is however need for employee empowerment in human rights as well as strengthening HIV work policy programs. The International labor organization emphasized that no employer is to deny employee opportunities or fire any employer in his line of duty because he is found with HIV infection unless when the employee is failing to deliver services. 26 Therefore, incorporating human rights activists in making these policies known to everyone through community sensitization would help to reduce HIV-related stigma in work places. 27
The health care system influences HIV-related stigma and this was previously reported by Chambers et.al. where they highlighted confidentiality violations as one way of inciting HIV-related stigma. 28 This was also highlighted in our study when participants complained of privacy and confidentiality especially in the public hospital and are usually afraid of being exposed by the health care workers. They further highlighted how institutional practices such as labeling client records was potentially a form inciting HIV-related stigma from other healthcare providers to the individual as a client has to carry the charts from laboratory to doctors all those people would give a judgmental eye to the individual. 28 Providing files that are not labelled, with no specific colour to those who are HIV infected can help to reduce HIV-related stigma and improve men involvement in health seeking behaviours.
There is a need therefore to reinforce the policy that looks at confidentiality of clients in HIV and AIDS. This can be done through refresher trainings for the health care workers on how HIV is transmitted and how to conceal patients or client's status in the health care setting. Health care providers with training in HIV-related stigma present with lower rates of stigmatizing attitudes than those who never attended the training. 29
Our finding also shows that the delivery of services in public facilities triggered stigma from others unlike in private hospitals where no one would notice the reason why one visited the hospital as everyone is treated equally. Another study also reports confidentiality violations by putting them on a line to receive ART treatment 18 as one way of inciting HIV-related stigma in public hospitals. 28 An earlier study reported that hospitals where policies regarding HIV-related stigma are reinforced experience lower levels of HIV-related stigmatizing attitudes compared to hospital which do not reinforce such. 29
Our finding show that hospital infrastructures where HTC and ART services are provided are close to the market or the road. This incited HIV-related stigma because people who are passing by can easily relate on what is going on. Earlier studies alluded to the fear harboured by men regarding members of their communities seeing them in health care facilities and assume that they were HIV infected. 29
Similarly, Treves-Kagan et al. argued that infrastructure played a role in keeping PLWHA from accessing care due to fears of disclosure. 9 This is compounded by the congestion in the facilities physical infrastructure that are not designed to serve such a high patient load eventually leading to long waiting times.
HIV testing services in Malawi have been criticized for being located near antenatal or under-five clinics which are traditionally female-oriented spaces where men do not find it comfortable to be. 30 This implies that men can be stigmatized by the women and that alone precipitate HIV-related stigma from the lookers. Dovel K et.al. found that general health education which was to give men an open point of entry to HIV testing and ART services were not done. 30 Therefore, taking into account the policies that govern men participation in public institution is very vital because more people will be knowledgeable to accommodate men when they see them accessing the services. In this way more men would be more comfortable hence reducing HIV-related stigma
In our study, participants preferred private facilities to public facilities because of unconsented disclosure which was also highlighted earlier that participants chose to receive care from private facilities than public facilities because of concerns over sero-status disclosure and added that care provided at public hospitals was inferior to care at private facilities. 31 People living with HIV are willing to spend money to receive treatment in a more confidential setting instead of utilizing the free care at the public health facilities to avert unintended disclosure. 31 This implies that Reinforcing confidentiality policy and human rights sensitization in these hospitals will help to minimize unintended disclosure thereby reducing HIV-related stigma.
Strength and Limitations
The study has presented the opinions and perceptions of heterosexual men and health care workers which means it provides the true opinions on how heterosexual men perceive HIV-related stigma, however the study used secondary data which means that the intended data set was not meant for this research nevertheless it highlights important insights in issues of HIV-related stigma. The sampling technique and the study design employed does not allow for generalization. Further research should use primary data to have reach information on HIV-related stigma.
Conclusion
HIV-related stigma exists and impedes access to HIV testing and ART services in Men. Isolation, shame and fear have shown to be among the factors precipitating poor access to HIV testing and ART services. HIV-related stigma is propagated by individual factors, family members, community members, workmates even health care workers. Our health care system needs to be amended in order to accommodate men to improve HIV testing capacity and access to ART services. There have been good reports, however, on how private hospitals provide these services country wide. Men preferred private hospitals to public facilities because of their ability to maintain respect to privacy and confidentiality to their client's. Imitating these policies into the public hospitals can help to improve the perception of HIV-related stigma in heterosexual men.
Supplemental Material
sj-docx-1-jiapac-10.1177_23259582211059921 - Supplemental material for “Men Are Scared That Others Will Know and Will Discriminate Against Them So They Would Rather Not Start Treatment.” Perceptions of Heterosexual Men on HIV-Related Stigma in HIV Services in Blantyre, Malawi
Supplemental material, sj-docx-1-jiapac-10.1177_23259582211059921 for “Men Are Scared That Others Will Know and Will Discriminate Against Them So They Would Rather Not Start Treatment.” Perceptions of Heterosexual Men on HIV-Related Stigma in HIV Services in Blantyre, Malawi by Thokozani Kazuma-Matululu and Alinane Linda Nyondo-Mipando in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.