
Abstract
Chronic pain among people with HIV (PWH) is a driving factor of emergency department (ED) utilization, and it is often treated with chronic opioid therapy (COT). We conducted a cross-sectional analysis of a prospective observational cohort of PWH on COT at 2 hospital-based clinics to determine whether COT-specific factors are associated with ED utilization among PWH. The primary outcome was an ED visit within 12 months after study enrollment. We used stepwise logistic regression including age, gender, opioid duration, hepatitis C, depression, prior ED visits, and Charlson comorbidity index. Of 153 study participants, n = 69 (45%) had an ED visit; 25% of ED visits were pain-related. High dose opioids, benzodiazepine co-prescribing, and lack of opioid treatment agreements were not associated with ED utilization, but prior ED visits (p = 0.002), depression (p = 0.001) and higher Charlson comorbidity score (p = 0.003) were associated with ED utilization. COT-specific factors were not associated with increased ED utilization among PWH.
Introduction
People with HIV (PWH) utilize healthcare services, particularly the emergency department (ED), at an estimated annual visit rate 1.5 times greater than that of people without HIV. 1,2 Chronic pain affects approximately 50% of PWH, and is a driving factor of ED visits in this population. 1 -3 Although antiretroviral therapy is effective in improving HIV clinical outcomes, pain is common even after treatment initiation and is associated with decreased antiretroviral medication adherence. 2,4 Chronic pain in PWH is more likely to be treated with higher doses of opioids for longer periods of time than pain in people without HIV. 5,6 Hence, chronic opioid therapy (COT) is common among PWH.
COT has been associated with mixed outcomes. COT may be positively associated with retention in HIV treatment and virologic suppression. 2,6 Assessment of attitudes regarding COT suggest that both clinicians and patients believe that COT keeps PWH engaged in care. 7 COT for chronic pain in the general population has also been associated with increased medical and pharmacy cost, ED utilization, and risk of overdose death. 8 -10 Rates of overdose and ED visits among patients on COT are compounded by the co-prescription of benzodiazepines with opioids, a practice occurring in 4-9% of PWH due to the high comorbid prevalence of anxiety and chronic pain. 2,11 -13
Supplemental Questions
What Do We Already Know about This Topic?
Chronic pain affects many people with HIV (PWH), and it is often a driving factor of emergency department (ED) visits. Many PWH with chronic pain are prescribed chronic opioid therapy.
How Does Your Research Contribute to the Field?
Commonly used risk mitigation strategies implemented for PWH on chronic opioid therapy have had varied success and their effects on ED utilization have received limited scrutiny; our research sheds light on the association between ED and chronic opioid therapy-related factors (dose of opioids, benzodiazepine co-prescribing, opioid use treatment agreements).
What Are Your Research’s Implications toward Theory, Practice, or Policy?
Greater understanding of factors driving ED utilization in PWH can help identify areas for intervention that might mitigate ED use for this population.
Commonly used risk mitigation strategies implemented for PWH on COT have had varied success and their effects on ED utilization have received limited scrutiny. 14 For example, risk mitigation via reduction of daily morphine milligram equivalent (MME) in patients on COT has unclear benefit on clinical outcomes. In a long-term implementation study of a risk reduction initiative that successfully lowered peak opioid dose in patients on COT, prevalence of prescription opioid use disorder was unchanged. 15 Despite increases in benzodiazepine co-prescribing and ED visits in the general population, 16 few studies have elucidated the impact of co-prescription practices on ED utilization among PWH. Opioid treatment agreements (OTAs), also known as pain management agreements or “contracts,” are occasionally but inconsistently used by HIV clinicians. 17 The effectiveness of OTAs is unclear; while designed to mitigate adverse outcomes such as overdose or opioid “misuse,” 18 some studies indicate they are unproductive due to the variation in provider protocols and lack of patient understanding. 19
This study examines associations between ED utilization and COT-specific factors, particularly those amenable to provider practices: dose of MME, benzodiazepine co-prescribing, and use of OTAs. We also examine factors known to be strongly associated with ED utilization among PWH, including age, gender, race/ethnicity, anxiety, depression, co-morbidities such as hepatitis C, previous ED use and past substance use that may confound the relationship between COT-specific factors and ED utilization. Given the increased medical and overdose risks associated with COT, as well as the intention of OTAs to minimize overdoses and other adverse outcomes, we hypothesized that high MME, benzodiazepine co-prescribing, and lack of OTAs would be associated with ED utilization among PWH. Greater understanding of COT-specific factors driving ED utilization in PWH could help identify areas for intervention that might mitigate ED use for this population.
Methods
Study Design
This study is a cross-sectional analysis of an observational prospective cohort of PWH on COT receiving care at Boston Medical Center or Grady Memorial Hospital in Atlanta. We collected the cohort data as part of the “Targeting Effective Analgesics in Clinics for HIV,” (TEACH) study, a randomized controlled trial testing the effectiveness of a collaborative care intervention to improve the management of PWH on COT (NCT02525731, NCT02564341). TEACH study primary outcomes included provider adherence to COT guidelines, patient level outcomes such as early refills, provider and patient satisfaction with care, and HIV disease status. 20,21 Data used in this study were from TEACH study participants (patient cohort data) and were collected through self-report and medical chart review.
Inclusion Criteria
The TEACH patient cohort included PWH at least 18 years of age who were treated with COT at 1 of the participating sites. Treatment with COT was defined as having had 3 or more opioid prescriptions written at least 21 days apart in the 6 months prior to enrollment. 22 Inclusion criteria also required that patients speak English, have a telephone number, and provide contact information for at least 2 contacts to assist with follow-up. Patients who were unable to consent for or understand the initial interview or planned to move from the area within 12 months were excluded from the study.
Measurements
Outcome
The primary outcome for this study was having an emergency department visit, defined as 1) any self-reported past 30-day ED visit at the 12-month follow up research visit or 2) any ED visit noted on electronic health record (EHR) review between study entry and 12-month follow up.
Through medical record review of the history of present illness, physical exam, and urine drug testing, ED visits were further categorized by a single abstractor for a for a subgroup analysis on reasons for ED visit. Categories included the following: 1) “probably opioid-related” (positive urine drug test for non-prescribed opioid or several clinical features for opioid-related harm [e.g., overdose, respiratory rate <12, response to naloxone, swelling near site of injection, or opioids explicitly requested]); 2) “possibly opioid related” (negative or no urine drug test, but supporting many clinical features likely for opioid related harm [e.g., musculoskeletal injury secondary to opioid intoxication, opioids were obtained, physician notes referenced concern for opioid use disorder, pain-related complaint]), or 3) “unlikely opioid related” (negative or no urine drug test, lacking clinical features for opioid-related harm [e.g., patient in ED for urinary tract infection]).
Potential predictors
Potential covariates were chosen a priori based on clinical knowledge and literature review. Independent variables included the following COT-specific factors measured at baseline: 1) prescription of high-dose opioids (defined as >50 MME); 2) co-prescription of benzodiazepines; and 3) lack of OTAs.
Morphine milligram equivalents (MME) is a measure of opioid dose and is calculated by taking the average of the doses the patient was prescribed over the course of 60 days prior to baseline. A calculated MME ≥ 50 mg was considered “high dose.” 16 We defined prescription of benzodiazepines as a prescription with >14 doses in order to capture long-term prescriptions. EHR review provided data regarding co-prescription of benzodiazepines and opioids in an outpatient setting in the year prior to enrollment. Lack of OTA at study entry was categorized as “yes” or “no” and obtained through EHR review and non-electronic health record review.
Other covariates, measured at baseline, included demographics and health characteristics such as details pertaining to substance use. Patients’ age, gender, race/ethnicity, housing, and employment status, collected by self-report, were included as independent variables in this study. Insurance status was determined from the medical records and was categorized by type of primary insurance at the visit prior to the baseline cohort date, including Medicare, Medicaid, private/commercial insurance, or self-pay/uninsured. Reported past 12-month employment status was measured categorically as working employed (full/part time) or unemployed. Unstable housing was defined as not owning or renting a residence. In terms of health characteristics, anxiety and depressive symptoms were measured at baseline using the self-report assessments State-Trait Anxiety Inventory and Center for Epidemiologic Studies Depression Scale, 23,24 respectively. HIV viral load and hepatitis C (HCV) co-infection were extracted from the EHR. HIV-1 RNA was categorized as above or below 200 copies/mL. HCV was defined as positive based on HCV antibody result or inclusion of HCV on the problem list. Co-morbidity burden was calculated using the Charlson comorbidity index. 25
Substance use variables, including past 12-month history of injection drug use, cocaine use, and overdose requiring medical attention, were collected via self-report upon enrollment. Alcohol use was recorded as healthy or unhealthy, based on the self-reported Alcohol Use Disorders Identification Test (AUDIT). 26 Data regarding opioid use disorder (OUD) among the participants was collected by EHR review. Other COT-related covariates, such as location of chronic pain and duration of opioids were collected through self-report. Number of ED visits prior to study entry were collected through self-report (past 30 day) and through EHR review (past 1 year).
Statistical analysis
Descriptive statistics on patient characteristics were conducted overall and by presence of a post-baseline ED visit. Differences by ED visit were compared using chi-square, Fisher’s Exact, 2 sample t-tests, and Wilcoxon rank sum tests, as appropriate. Additional descriptive analyzes were performed on the reason for ED visit. We also examined reason for ED visit by high versus low MME. For the multivariable analysis testing which factors were associated with an ED visit, a forward stepwise selection approach was used to select a final parsimonious model. See Table 1 for variables originally included in the model. COT-specific factors of interest (i.e., benzodiazepine co-prescribing, OTAs, and high dose opioids), age, and gender, were forced into the model. The model selection for these covariates was guided by Bayesian Information Criterion. 27 As a sensitivity analysis we used a selection approach based on the Akaike Information Criterion. 28 The final model included the following predictors: age, gender, years on opioids, high dose opioids, co-prescribing of benzodiazepines, lack of OTAs, hepatitis C, depression, prior baseline ED visits, HIV-1 RNA <200 copies/mL, and Charlson co-morbidity index. We also performed a sensitivity analysis that included an indicator variable for enrollment in the randomized control trial.
Select Demographics, Health Characteristics, and Chronic Opioid Treatment (COT)-Specific Factors of PWH on COT at Study Entry.
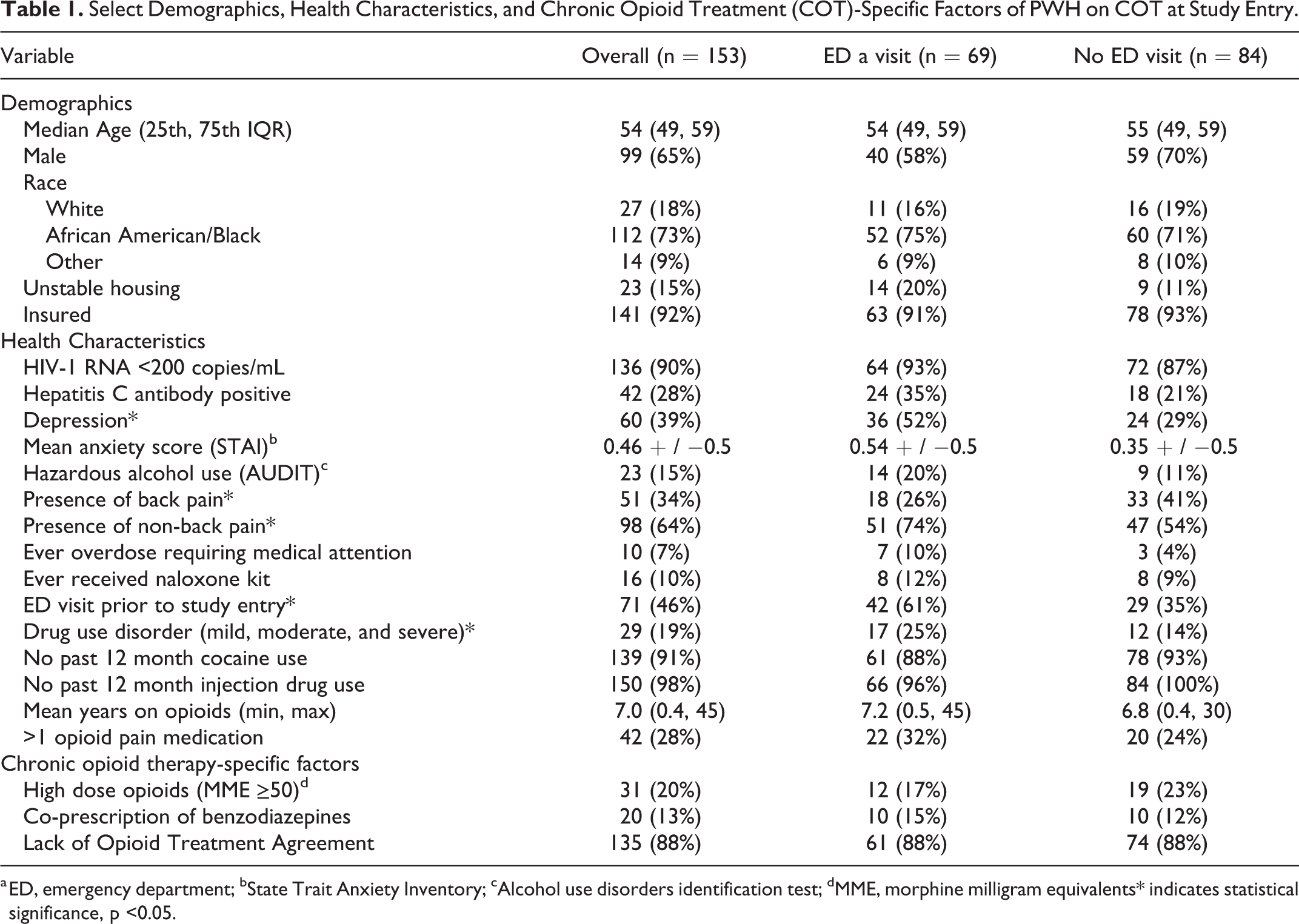
a ED, emergency department; bState Trait Anxiety Inventory; cAlcohol use disorders identification test; dMME, morphine milligram equivalents* indicates statistical significance, p <0.05.
Ethical Approval and Informed Consent
The TEACH study was approved by the institutional review boards at Boston University Medical Campus (H-33343, March 24, 2015), Emory University (CR001-IRB0008834, April 7, 2016) and Grady Research Oversight Committee (000-81024, April 12, 2016). All patient participants provided written consent to participate.
Results
Study participants (N = 153) had the following characteristics: mean age of 54 years old (+ / −8 years); 65% male; 73% African American/Black; 85% with housing; and 92% had health insurance. Ten percent of participant had reported ever receiving a naloxone rescue kit. Almost all participants reported past 7-day pain (34% back pain and 64% other kinds of pain). Almost half (45%; n = 69) of study participants visited the ED within the previous 12 months. While 22% of participants self-reported an ED visit within the previous 30 days, a majority (n = 60) of ED visits were identified through EHR review (Table 1). When examining reasons for ED visits, 25% of all ED visits were due to pain, 12% were probably or possibly related to opioid use, and 17% of ED visits resulted in hospital admission (Table 2). Opioids were prescribed in 10% of ED visits. Very few visits were due to opioid-related harm (1%), intoxication (0.7%), or injection drug use-related infection (0.7%). No visits were due to opioid overdose. Seventeen percent of participants with pain-related ED visits were prescribed high dose opioids prior to those visits, compared with 83% prescribed low dose opioids. Of those participants prescribed high dose opioids, the median number of COT provider visits was 5 visits in the prior 12 months. Participants who received low dose opioids had a median of 4 visits in the prior 12 months.
Reasons for Emergency Department Visits During Study Period for PWHa on COT.b

a PWH, person with HIV; bchronic opioid therapy; cED, emergency department.
In unadjusted analyzes, participants with high dose opioid prescriptions were not more likely to have ED visits (Table 1) (17% vs. 23%, p = 0.42). No significant differences in ED visits were associated with co-prescription of benzodiazepines (15% vs. 12%, p = 0.64), and lack of OTAs (88% vs 88%, p = 0.95). Participants with hepatitis C were more likely to have an ED visit (35% vs. 21%), as were those with depression (52% vs. 29%, p = 0.003), higher anxiety scores (STAI score 0.54 vs. 0.35), hazardous alcohol use (20% vs. 10%), drug use disorders (25% vs. 14%, p = 0.02), and unstable housing (20% vs. 10%). Mean duration of opioid treatment duration was slightly longer for participants who visited the ED than those who did not (7.2 vs 6.8 years, p = 0.09). Presence of non-back pain was more likely among those with an ED visit than those without (74% vs. 54%, p = 0.05). Participants who had an overdose requiring medical attention in the past were also more likely to have an ED visit (10% vs. 4%). Other variables are further described in Table 1.
In the multivariable analyzes, a priori COT-specific factors including high dose opioid prescriptions (adjusted odds ratio, 0.37; 95% CI 0.13-1.05), co-prescribing of benzodiazepines (aOR, 0.97; 95% CI 0.0.33-2.86), and lack of OTA (aOR, 0.62; 95% CI 0.18-2.12) were not significantly associated with an ED visit (Table 3). The strongest predictors of ED utilization were a history of ED visits prior to baseline (aOR, 3.54; 95% CI 1.63-7.69), history of depression (aOR 3.81, 95% CI 1.71-8.51) and increased co-morbidities as defined by the Charlson co-morbidity index (aOR, 1.47; 95% CI 1.17-1.85). Although not statistically significant, participants with hepatitis C had a higher odds (2.31 (95% CI 0.96-5.56) of visiting the ED than those without those risk factors. In the sensitivity analysis, enrollment in the randomized control trial was not associated with ED utilization.
Factors Associated With Emergency Department Utilization for PWHa on COT.b

a PWH, person with HIV; bchronic opioid therapy; cED, emergency department; dMME, morphine milligram equivalents.
Discussion
In this study of PWH receiving care and chronic opioid therapy at 2 urban safety net hospitals, COT-specific risk factors were not were not associated with ED visits, whereas presence of co-morbidities and history of a prior ED visit were. While co-prescription of benzodiazepines has been associated with ED visits in other studies, it has not been extensively studied among PWH on COT. 9 Increased risk of death and ED utilization from benzodiazepines has been shown to be dose-related and also more likely with shorter-acting benzodiazepines; it is possible that some participants could have been prescribed lower dose, longer-acting benzodiazepines or taken fewer benzodiazepines than prescribed. 29 -31
In our study, the lack of OTAs was also not associated with an increased likelihood of an ED visit. While not specific to PWH on COT, some research in rural areas has suggested that OTAs have the potential to reduce ED visits, 32 while other studies have not found an association between OTAs and ED utilization. 33 Although perhaps well-intentioned and sometimes serving the purpose of meeting regulatory requirements, the use of OTAs, as assessed in our study, was not associated with decreased ED utilization. Other ways to optimize safety measures for COT patients, such as prescribing naloxone and intensifying mental health referrals when applicable, should be further investigated among PWH. 34
Lastly, the effect estimate for prescription of high dose opioids, while not statistically significant, was in the direction opposite of what we hypothesized, favoring less ED utilization. This finding could have been due to adequate pain control; notably only 17% of participants with pain-related ED visits were prescribed high dose opioids, compared with 83% prescribed low dose opioids. Interestingly, however, self-reported pain relief was similar in both groups. Participants prescribed high dose opioids could have also had more frequent primary care follow-up and/or case management, both of which have previously been associated with lower frequency of ED visits. 35,36 We were unable to capture those variables across the 2 study sites; however we were able to capture the median number of COT provider visits, which was just slightly higher among patients who received high dose opioids (5 visits in the past 12 months) versus low dose opioids (4 visits in the past 12 months). While it is possible that participants prescribed high dose opioids could have had providers that adhered to safe prescribing guidelines, in a prior TEACH analysis, only 6.5% of participants who received high dose opioids had complete COT monitoring (OTAs, urine drug tests, and pill counts). 17
Multivariable analyzes additionally found that the presence of other medical co-morbidities and prior ED visits were associated with increased ED utilization, which is consistent with prior literature. Our results suggest that the presence of multiple co-morbidities and history of prior ED visits should heighten providers’ awareness of the potential risk of frequent ED utilization, more so than COT-specific factors. Use of an ED utilization risk assessment score, particularly for those with prior ED visits and several co-morbidities like hepatitis C and depression, could help identify people at risk for ED utilization. 35,37 In addition, facilitating follow-up primary care appointments, mental health referrals, and expanding access to health insurance could also be helpful in reducing ED visits. 36,38
The descriptive results from this study support existing literature regarding the care and treatment of PWH. As would be expected, chronic pain was prevalent in this cohort, and accounted for a quarter of the ED visits that took place during the observation period. The finding that over half the participants with an ED visit reported depression also further bolsters the established association between chronic pain, HIV, and psychiatric symptoms. 39 While notably no ED visits were due to overdoses, only 10% of the study population reported receiving a naloxone kit. While low, these results are similar to prior research that has examined naloxone co-prescribing in individuals at risk for overdose. 40 With 20% of the study population prescribed >50 MME, naloxone co-prescribing and increasing naloxone access remain areas for improvement. 16
Limitations of this study include the risk of recall bias; some variables, such as past 12-month injection drug or cocaine use and provision of naloxone kits, were measured via self-report. Variables of interest such as stimulant use and injection drug use were excluded from the model due to small numbers. Two COT-specific variables of interest (MME, OTA) were collected at baseline and follow up, but to ensure that these variables pre-dated follow up ED visits, we used baseline data for the COT-specific variables. Thus, we were unable to account for any potential changes between study entry and follow up study visits. Categorization of ED visits was a clinical decision based on EHR notes, so misclassification could have occurred. Chart review of ED follow-up visits were limited to the study site health systems; however, self-report data on ED visits were also collected to address this limitation.
Conclusions
Opportunities to promote decreased ED utilization for PWH on COT should focus on individuals with prior ED visits and other co-morbidities. COT-specific factors such as high dose opioids, benzodiazepine co-prescriptions, and lack of OTAs were not associated with ED utilization in this population.
Footnotes
Author’s Note
Conceived and designed the study: KT, AK, SR, AW, ML, LF, JC, JS. Analyzed the data: LF, SR. Wrote the paper: KT, AK, SR, AW, ML, LF, JC, CDR, JS. Identifying information removed per author guidelines.
Acknowledgments
The authors would like to acknowledge the study participants for providing their time and would also like to thank Florencia Pereira and Christine Capozzi for their contributions to this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by awards R01DA037768, P30AI050409, and P30AI042853. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.