
Abstract
Objectives:
The study aimed to see predictors of undernourished and its implication towards HIV continuum care.
Study Design:
unmatched case-control study was conducted among 678 individuals in Jimma zone, southwest Ethiopia.
Methods:
Randomly selected data of 339 PLWHA who had poor nutritional outcomes (cases) and 339 without undernourished (controls) were analyzed. Logistic regression was used to identify forecasters of undernutrition. The quantitative results were supplemented from key informants who work closely on HIV care, then data were coded and analyzed thematically.
Results:
Rural residence (AOR:1.8; 95% CI: 1.2, 6.4), female (AOR: 2.9; 95% CI: 1.1, 4.3), unstable livelihood (AOR: 5.1; 95% CI: 4.2, 19.6), low meal frequency (AOR: 6.6; 95% CI: 5.2, 21.1), less diversified foods (AOR: 3.5; 95% CI: 1.2, 14.3), and advanced WHO clinical stage (AOR: 4.3; 95% CI: 3.6, 13.7) and were found to be independent predictors of undernourishment. No social support advanced clinical stage, and unstable livelihood adversely affect nutritional status of PLWHA from the qualitative data.
Conclusions:
The socio-cultural, economic, and health-system factors inhibit ideal patient nutritional status. Better tracking, enhanced livelihood and social support along with drug therapy, food aid needs to consider for PLWHA.
What Do We Already Know about This Topic?
HIV-induced immune impairment and its resulting opportunistic infections (OIs) can decrease food intake; increase energy expenditure; cause nutrient malabsorption; and alter the body’s ability to utilize and excrete nutrients leading to nutritional deficiencies health problems. Nutritional deficits can, in turn, hasten the progression of HIV infection and increase the risk of developing OIs. This, in turn, affects overall clinical outcomes, quality of life, and chances of survival.
How Does Your Research Contribute to the Field?
Nutritional support and improvement of livelihood are very crucial to ensure HCC for the following reasons: (1) low BMI is associated with higher morbidity and have poor out came of ART (2), food and nutrition can improve adherence to treatment and retention in care, (3) in addition to Food and nutritional support stable livelihood can support the quality of life for PLWHA.
What Are Your Research’s Implications toward Theory, Practice, or Policy?
Ethiopia badly needs, improvement of livelihood/income generation opportunities and behavioral change on dietary diversity to address nutritional problems at the grass rout level, rather than symptomatic treatment and donor driven program food by prescription which may affect the outcome of HCC.
Introduction
HIV prompted immune impairment and its occasioning opportunistic infections (OIs) can diminution Appetite; intensification energy outflow; effect on malabsorption; and vary the body’s capability to operate and evacuate nutrients prominent to nutritional deficits and unfortunate overall nutritional status. 1 Nutritional shortfalls can, in turn, accelerate the movement of HIV infection and rise the hazard of emerging Ois. 2 -6
In people with high HIV prevalence the adverse interactions between undernourished and HIV can influence health system of a nation. 7 -9
Highly active Antiretroviral therapy (HAART) is believed to be a key to HIV allied degenerative. Nonexistence of diet, food insecurity, and the concern about diet has been shown to decrease treatment faithfulness. 10 -16 Furthermore, starvation and medicine for opportunistic infections may interact in ways that reduce the efficacy of HAART, and HAART itself might influence metabolism, as well as causing side effects that lead to reduce desire for food. 17
Ethiopia has been reducing incidence of adult HIV status from 6.5% to 1.5%, but this symbol represents a huge number of individuals: 793,700 PLWHA plus 200,300 children. 18,19,20 of who 420,000 (59% of those in need) are now receiving HAART. 21 Alternatively, around 9% of Ethiopia’s people is undernourished and the country’s rate of stunting is 38%. 22,23 It is, realistic to expect that many PLWHA receiving HAART in Ethiopia can’t get sufficient, worth and amount diet. Alternatively, nutritional support with early initiation of ART has been known to have a substantial role to interruption the vicious circle between HIV and malnutrition. 24 -27
However, thoughtful of in what manner starvation, HIV behavior and what factors stimulus individuals’ risk of undernutrition while on HAART in developing countries like Ethiopia is still marked with a relatively few studies conducted given the huge overlap among food insecurity, undernutrition, and HIV-infection. In this regard, several studies have focused on assessing recovery rate and benefit of nutritional support, the magnitude and distribution of undernourished. 28 –32 The intention of this research was to assess the predictors of undernutrition and its implication towards Human Immuno virus and HIV continuum care (HCC) among adults PLWHA in in south west Ethiopia.
Methods
Study Setting
The study was conducted in five public hospitals found in southwest Ethiopia; namely: Jimma Medical center, Shenen Gibe, Seka, Agaro and Limugent Hospitals. Jimma zone is found in Oromia Regional State, to Southwest of Ethiopia at a distance of 355 kilometers from the Capital city of the country Addis Ababa. During the study period, a total of 11,186 adults and 2,683 pediatric PLWHA were on chronic HAART care.
Study Design and Population
This is unmatched case-control study conducted among PLWHA aged 18 years and above. Cases/undernourished were defined to be those PLWHA who had body mass index (BMI) less than 16 kg/m2, which implies severe undernutrition or those who had moderate mild undernutrition (BMI 16.5-17.4 kg/m2). Controls were PLWHA who had normal nutritional status (BMI between 18.5 kg/m2 and 24.9 kg/m2). In addition in-depth interviews of ART service providers, ART coordinators, community advocators, and adult PLWHA were conducted and supplemented to the quantitative data.
Sample Size and Sampling Procedures
The sample size was calculated using G-Power software using double-population proportion formula. Our outcome of interest was predictors of undernutrition for PLWHA. We estimated the proportion of the patient population that would be malnourished by reviewing patient records to find how many patients had reported problems with sever or moderate undernutrition at intention of ART by BMI.
The percentage of PLWHA with undernourished was 19% and the adjusted odds ratio for the association between consumption problem was 2.4, one-to-one ratio of control to a case, 33 a 5% level of significance and a power of 80% were considered. Accordingly, the overall sample size was 678 (339 cases and 339 controls) PLWHA. We selected our sample by extracting a list of all of the eligible patients on ART in the clinic from the clinic registration book. This list was divided into cases and controls based on the patient BMIs recorded in the registration book. We then used simple random sampling to select participants from the case and control lists using SPSS (version 20).The sample size was allocated to each of the hospitals based on probability proportional to sample size of cases (1,231) and controls (9,955).
The aim of in-depth interviews were used as exploratory of the predictors for undernutrition among 14 study participants from HAART service providers, community advocator, HAART coordinators, and adult PLWHA, who were purposively selected considering their roles and experiences they had to provide rich and relevant information. Finally, research team leader made further probe the content of the field notes and debriefing sessions.
Data Collection and Instrument
Data was collected using interview administered questionnaire. Economical status was assessed using wealth index, which was determined by Principal Component Analysis (PCA). Out of 24 variables namely source of income in the last 12 months 8 variables were extracted in the final iteration. three variables were highly loaded on the first and second PCA components, namely own mobile, bed with sponge, fuel, charcoal, household farmland, households own sheep, goats and two variables in the third component namely having a refrigerator and fuel electricity.
Therefore, the wealth index score was made by eight variables with three components that explained a total variance of 66.86% and Kaiser Meyer Olkin measure of sampling suitability 0.75 with Bartlett’s test of sphericity at a worth of 0.001.
Data Analysis
The data were entered into Epi data version 3.14 Software and transferred to SPSS for window version 20.0 Software. At the outset, frequencies tables were computed to summarize socio demographic information of the study participants. Secondly, bivariate analysis was carried out to identify candidates of the outcome variables at P-value ≤ 0.25. Multivariable logistic regression was used to assess the adjusted odds ratio and variables were considered significant if the p-value is <0.05. Before the inclusion of predictors to the final logistic regression model, the multi-collinearity was checked using the Variance Inflation Factor (VIF) <10 for continuous independent variables. The goodness of fit of the final logistic model was tested using Hosmer and Lemeshow test at a p-value of >0.05. Outcome measures were indicated by the odds ratio with 95% confidence interval, and the significant association was declared at p <0.05 for the final model.
We have developed a four teams of the qualitative data as exploratory indicators of the quantitative data, such as: household food insecurity situation, challenges with food by prescription program and Food Aid, stigma and challenge of HIV continuum care and dietary diversity and coping mechanisms of PLWHA.
Ethical Approval and Informed Consent
This study was approved by the institutional review board of the Institute of Health Jimma University, Ethiopia (Ref. No. IHRPGC/1095/2017).All participants provided written informed consent prior to enrollment into the study, and data were explained in aggregated way to maintained confidentiality throughout the data analysis and manuscript preparation.
Results
Back Ground Characteristics of PLWHA
Majority of the study participants were females who constituted 239 (70.5%) and 215 (63.4%) among cases and controls, respectively. Urban residents comprised more than two-third both in cases 216 (63.7%) and controls 248 (73.3%). Close to three in ten of both cases (29.7%) and controls (28.9%) were able neither to write nor to read. Another three in ten of cases (30.9%) and controls (29.6%) were either unemployed or daily laborers (Table 1).
Socio-Demographic Characteristics of Adult PLWHA, Jimma Zone Public Hospital, South West, Ethiopia, September 2018.

House Hold Food Security and Livelihood of PLWHA
A hundred percent of cases reported to have worried about availability of food. While only 55 (16.1%) of the controls reported worries about food availability. The study also found that 98.6% of cases and 1.4% controls had household food insecurity. A total of 103 (30.4%) of cases have reported experience of coping mechanisms to support their livelihood. The mechanisms include: borrowing money from family, borrowing food or selling agricultural products, selling property, use of previous savings, mortgaging/renting property and loan from micro-finance /bank/friends (Table 2).
Responses Household Food Security Status and Livelihood of Adult PLWHA in Public Hospitals of Jimma Zone, September, 2018.

N.B. Way of assurance on stable livelihood: Borrow money from family + Borrow food or sell agricultural products + selling property + previous savings, mortgaging/renting property + Loan from microfinance /bank/friends.
Nutritional Diversity Practice and Livelihood of PLWHA
The study also indicated that majority of the cases 297 (87.4%) reported eating less than the mean dietary diversity while only 58 (17.1%) of the controls reported to have had eaten less diversified foods during the preceding 24 hours of the study. The food types frequently consumed by the controls were cereals 334 (98.4%), oil/fats 324 (95.5%) and condiments/coffee/tea 293 (86.3%), whereas Fish/sea foods 9 (2.7%), eggs 87 (25.6%) were least consumed food groups (Table 3).
Nutritional Diversity Practice and Livelihood of PLWHA on ART, JIMMA Zone Public Hospitals, September 2018.
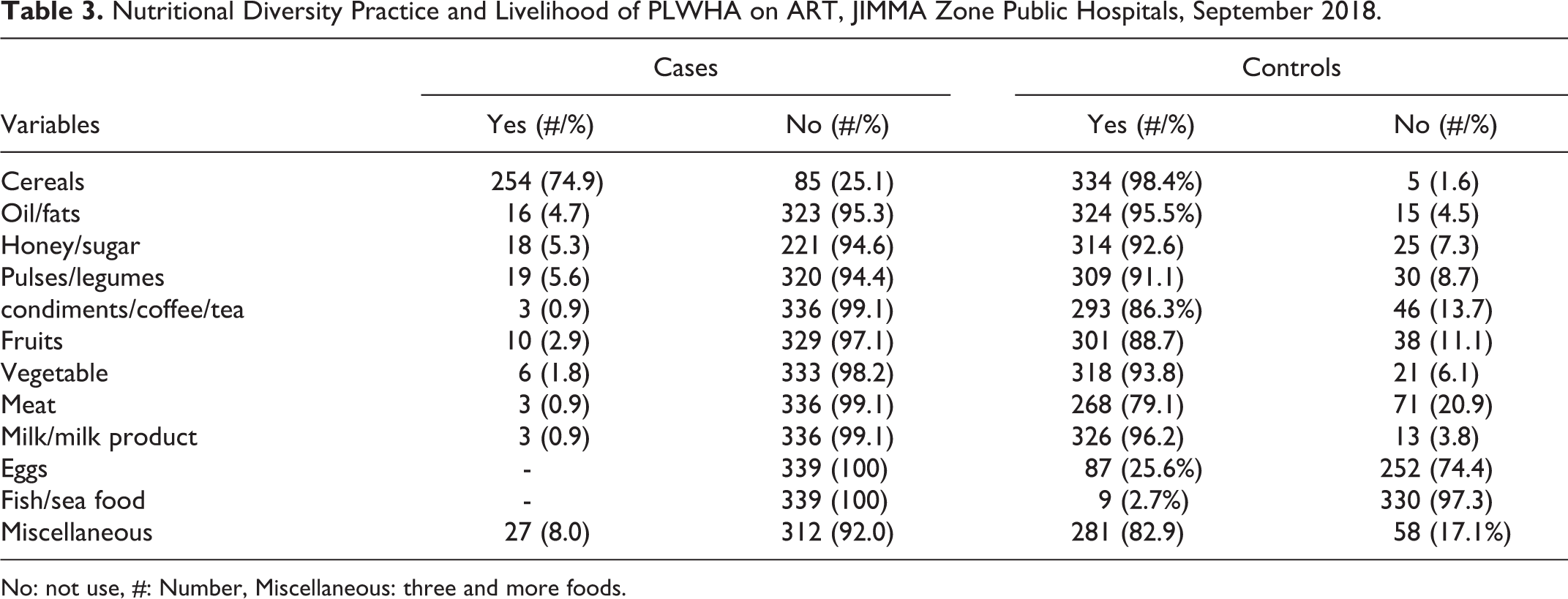
No: not use, #: Number, Miscellaneous: three and more foods.
Predictors Associated with Undernourishment among Adult PLWHA
Rural residents were about two times (AOR: 1.8; 95% CI: 1.2, 6.4) more likely to be undernourished compared to urban residents. Female respondents were almost three times (AOR: 2.9; 95% CI 1.14, 4.3) more likely to be undernourished compared to males. Similarly, the likelihood of being undernourished was more than three times higher among households who were food insecure (AOR: 3.3; 95% CI: 4.3, 14.4).PLWHA who were in unstable livelihood were five times (AOR: 5.1; 95% CI: 4.2, 19.6) more likely to be undernourished compared to those who had stable livelihood. Those who reported lower meal frequency were six times (AOR: 6.6; 95% CI: 5.2, 21.1) more likely to be undernourished compared to their counterparts (Table 4).
Predictors of Undernutrition among Adult PLWHA in Jimma Zone Public Hospitals, South West Ethiopia, September 2018.

*:P < 0.05, **:P < 0.01, AOR: adjusted odds ratio, CI: confidence interval. The AOR was calculated after adjusting for other independent variables, religions, marital status, employment status at p < 0.05.
Qualitative Results
The in-depth interview data were collected to explore the finding of quantitative study. Finally we have develop the following themes; Household Food Insecurity situation, Challenges with Food by Prescription program and Food Aid, Stigma and discrimination as challenge of HIV Continuum care and Dietary diversity and Coping Mechanisms of PLWHA.
Most of the participants were sensitive when they were chatting about food insecurity condition of PLWHA. One of the female ART advocater participants said……“Live alone with the disease and the limited capacity because of the disease HIV, now a day it is difficult to survive even for one BSc graduate Ethiopian with his/her monthly income.” Another 36 years old ART coordinator participant explained the food security status of PLWHA by saying……“You better leave asking such a question because PLWHA is wasted thinking of food and becoming difficult taking their pill without food.”
Similarly, a 46 years old respondent from PLWHA explained the impact of household food shortage on ART compliance as follows:…. “You have been asking me, what I didn’t want to talk; I am suffering in thinking of food and becoming difficult taking the pill without getting food. I can say it is difficult to consume any food on time in my home and I know similar problems with others too.”
Another 35 years old female participant from rural residence said that……” Living is getting expensive for PLWHA,” you see ‘I need to eat 6 times per day. The drug needs that much,’ But most of the time I couldn’t even afford to eat three times per day. Sometimes I feel shame when I visit my friends and eat any food they give me without any hesitation.”
The participants also mentioned that the food ration/support they were getting from the program of Food by prescription was inadequate. In addition, it reported to be very small in amount and inconsistent to cover dietary needs of the PLWHA. The discussants mentioned that the problem of getting enough food aid of what one likes is not confined to PLWHA on ART. But when there is increased need to eat and the stakeholders and health system denies the chance of accessing food through BMI as criteria of nutritional wellbeing. Things become worst for nutritional problems and lead to be hopeless for PLWHA.
In addition, almost all participants mentioned some dangerous coping strategies that could even exacerbate the existing prevalence of the pandemic. One 36 years old female from the PLWHA participant said: “Had it not been for God help……you know when you fail to find any food to eat you are obliged to do anything….anything including changing sex for money.” All participants recommended some sort of income generating activities and creating job opportunity for PLWHA on ART as the state-of-the-art food security strategy to sustainably respond to the increasing support need of PLWHA on ART regularly other than the symptomatic treatment and criteria based approach of food aid.
A 35 years old male participant of ART service provider said that……“ART took PLWHA far away from illness and death. But to keep the sustainability of this promising outcome and to start thinking more about their health, they need to have access to job and sustainable livelihood. If they work, they support themselves and their country, thus they don’t want any food ration if they have food at home.”
Stigma and discrimination by relatives, poor counseling, lack of home-based care service, being away from home, religious reasons (wholly water), simply forgetting the pills and especially lack of food were mentioned to reasons for interruption of HCC. A 40 years old female advocator participant said that……“I know a PLWHA who discontinued ART. They came to Hospital long after they stopped taking their drugs. I asked some of them friendly why they discontinued their ART. Most of them said that their families and community at large were stigmatizing them a lot. Even they couldn’t sell something to their community. People buy from others by passing them; they think as if they put their blood in the goods they sell.”
Another participant aged 28 years who was ART coordinator explained stigma and discrimination as negative implication of HCC by stating: “If clients are sex workers, they prefer to be happy and live temporary life without thinking about their future. They mostly don’t even get social support and become hopeless. This group will not share and communicate their ideas with the community members. They feel loneliness owed to worry of shame and refinement. At the same time, individuals in the community consider as if they would attack them, so such PLWHA may not regularly follow their ART care according the new HCC.”
For majority of the patients food is their big head ache; however, they take their ART despite of adverse effects and insufficient food. Right of entry medicine on the Right time was extremely prized and PLWHA described HAART and food aid as “a new courage for the upcoming life.” When patients were asked directly about what makes them happy in their lives, majority of them mentioned that availability of ART and food by prescription program. But the availability of food at home as demanding is a very critical challenge for economically poor PLWHA.
The participants also reported some coping strategies; reducing the portion of the food they consume, passing part or whole of meals of the day, selling fixed asset they have, borrowing money from relatives & friends and sending their children to their families were some of the coping mechanisms they mentioned.
Discussion
In this study, the main predictors of undernutrition were found to be rural residence, less meal frequency, less dietary diversity, Kchat chewing, low level of hemoglobin, difficult livelihood, female, advanced WHO stages both at ART initiation and during the study, presence of OIs and low level of CD4 counts during the study, household food insecurity and lack of food aid.
In this study PLWHA who live in rural settings were more adversely affected nutritionally. This finding is similar with studies done in Tanzania and west shewa 34 –41 which showed that rural residents were prone to undernourishment and poor clinical outcomes. This similarity might be because access and utilization of services are rendered in urban areas as compared to rural. Regard to behavioral factors, participants who chew Kchat frequently were more affected by undernourished. This is similar to the findings of Butajura 42 and Nekemte. 43 This could be because of PLWHA who use substances /alcohol poorly adhere to ART, which in turn may adversely affect nutritional status.
Those PLWHA in an unstable livelihood were more likely to be undernourished. This finding is similar with studies conducted in Nekemte 44 and Brazil 45 which shows that unstable livelihood was strongly associated with poor nutritional status. This could be because of low economic status and poor working capacity, both of which lead to a lack of access to sufficient foods, consequently resulting in undernourishment.
PLWHA who had advanced WHO stages at ART initiation were more likely undernourished than those who had WHO stage I and II. This finding is inline with the studies conducted Kenya and South Africa 46,47 that patients with WHO stage III and IV reported to have a poor nutritional status than their counterparts. On the other hand, studies conducted in Tanzania 48 and Brazil 49 revealed that symptomatic patients significantly presented with undernutrition. In this regard, Ethiopia has only one program which is called “food by prescription” which mainly focuses on symptomatic PLWHA.
The present study identified clinical related predictors of undernourishment were low level CD4 count at ART initiation, advanced WHO stage both at ART initiation and during the study and, low level of hemoglobin. Similarly, behavioral and demographic factors such as kchat chewing, low meal frequency, household food insecurity, absence of food Aaid and low dietary diversity, rural residence, female gender, unstable livelihood were significantly associated with undernourishment. 50 –52
The qualitative findings indicated that, nutritional support and improvement of livelihood are very crucial to ensure HCC for the following reasons: (1) low BMI is associated with higher morbidity and have poor out came of HAART (2), food and nutrition can improve adherence to treatment and retention in care, (3) in addition to Food and nutritional support stable livelihood can support the quality of life and HCC for PLWHA. From this point of view, Ethiopia badly needs, improvement of livelihood/income generation opportunities and behavioral change on dietary diversity to address nutritional problems at the grass rout level, rather than symptomatic treatment and donor driven program food by prescription which may affect the outcome of HCC.
Limitation
A limitation of this study is that BMI has been used as a criteria for the selection of cases and controls. BMI detects simply protein-energy malnutrition/macronutrient problems. A further prospective study on a large size of study participants or randomized clinical trials is needed to better understand the actual predictors of undernourishment both macro and micro nutrients among PLWHA for evidence based action.
Footnotes
Authors’ Note
All the data sets used and/or analyzed are include in the article.
Acknowledgments
Our acknowledgment goes to study participants, data collectors, research assistants and Jimma University for covering the cost of the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Jimma University. The views presented in the article are of the author and not necessarily express the views of the funding organization.