
Abstract
The research was designed to assess the stigma and discrimination faced by People living with HIV and AIDS (PLWHA) that are receiving treatment in UITH, Ilorin. The study was a descriptive cross-sectional survey conducted on three hundred (300) people living with HIV and AIDS receiving care at the antiretroviral therapy (ART) clinics within University of Ilorin Teaching Hospital (which was the only ART site in Kwara State as at then). A quantitative method through the use of interviewer administered questionnaire was used for data collection. This study was a cross-sectional descriptive study design. All the patients who came to the clinic and met the selection criteria were recruited until the desired sample size was reached. Data were analyzed by EPI-INFO 2005 software package. The mean age of the respondents was 39 years (SD = 9.32), and their age ranged between 19 and 65 years. About two thirds (64.7%) of the respondents were females, 62.7% were married, and 62.9% were from monogamous family settings. Slightly less than half (47.3%) of the respondents were not informed before they were tested for HIV, majority (63.3%) were not counseled before the test, but only 11% did not receive posttest counseling. One quarter of the respondents had experienced stigmatization/discrimination. Various forms of stigmatization/discrimination experienced by the respondents include blame for being responsible for their HIV status, various name callings, telling them that they are no more useful to anybody, violation of confidentiality, social isolation, restriction of their participation in family/religious activities, rejection by their spouses/families, dismissal from place of work, isolating them from other patients, and denying them care at health centers. It is therefore recommended that government at all levels should develop and implement programs to educate health care providers about HIV and AIDS, ethics, and treatment and care; educate the general population on HIV and AIDS, put in place policies that will reduce/stop HIV-related stigma and discrimination at all levels of the society, educate PLWHA on their right to live and work without discrimination, and also ensure full community participation in HIV control programs.
Introduction
HIV and AIDS is not only the greatest health challenge of our time, it is also the greatest human rights challenge. 1 Thus people living with HIV (PLWH) shoulder the twin burdens of stigma and discrimination. The fear of becoming HIV infected underlies stigma and discrimination, and the impediment to prevention of HIV transmission and provision of treatment, care, and support services to the PLWH and their families. 2 HIV- and AIDS-related stigma is increasingly recognized as the single greatest challenge to slowing the spread of the disease at the global, national, and community level.3–7
Stigma and discrimination exist at different levels and constitute barriers to the full involvement of people living with HIV and AIDS (PLWHA) in policy and planning, and acceptance in many communities. Stigma and discrimination are common practices in many health facilities and are disincentives to people seeking voluntary testing. 8
Three phases of HIV and AIDS epidemic have been described, the epidemic of HIV; the epidemic of AIDS; and the epidemic of stigma, discrimination, and denial. The third phase is as central to the global AIDS challenge as the disease itself. 1 It is now a well-known truth that PLWHA in Nigeria suffer human rights violations, in the work place, hospital, community, and family. Many of such violations are hardly redressed or challenged. 9
Globally, the HIV and AIDS epidemic is magnified by denial, stigma, and ignorance on modes of transmission. Many people living with the virus are ostracized by friends, family members, and the larger civil society. This in turn keeps many people from finding out their HIV status for fear of stigmatization. 10
HIV- and AIDS-related stigma is as complicated as it is dynamic. It changes both as the individual progresses from HIV to AIDS, and as the HIV epidemic evolves in a given society. The diversity of its manifestation impacts negatively on preventive behaviors and accelerates transmission. Stigma and discrimination mainly manifest in the forms of social isolation from family, friends, and community; gossip, name calling, insults, judging and blaming; and a loss of rights, decision-making power, and access to resources and livelihood. 11
HIV- and AIDS-related stigma and discrimination are strong barriers to the success of HIV and AIDS controlled programmes and must be overcome in order to achieve effective HIV and AIDS control globally. People living with HIV face stigma and discrimination both from within and outside their communities. This keeps many of them out of the workforce and on the margin of the society. It also prevents them from getting the health care and other services they need to stay healthy. Inadvertently some workers have described stigma and discrimination as more deadly than the HIV virus. The rapid spread of HIV and AIDS can be directly attributed to HIV- and AIDS-related stigma and discrimination. Stigma and subsequent discrimination causes silence that in turn results in the spread of HIV and AIDS. 12
Considering the myriads of stigma and discrimination manifestations coupled with the fact that there is dearth of studies on HIV-related stigma and discrimination in this environment, it is pertinent to know the common manifestations of stigma and discrimination among PLWHAs accessing care in health facilities. This informed the need for this study which was aimed at assessing stigma and discrimination experienced by the PLWHAs receiving care/treatment at University Teaching Hospital, Ilorin, North Central, Nigeria.
Materials and Method
The study was conducted in University Teaching hospital, Ilorin, Kwara State, Nigeria. It is a 500-bed capacity and the only tertiary health facility in Kwara State. The hospital provides HIV counseling and testing (HCT), antiretroviral treatment (ART), and supportive care at 3 distinct clinics; Medical Outpatient Department (MOPD), hematology clinic, and the General Outpatient Department (GOPD). The available hospital records showed that about 1300 clients had enrolled for treatment and care in the hospital between 2005 and September 2007. This number (1300) of enrolled patients on ART registered at the time of this study comprises the dead, lost to follow up, transferred out, and the currently active patients in the hospital. The study was a descriptive cross-sectional survey. First, approval for the study was sought and obtained from the hospital’s research ethics committee. Because we could not get the actual number of patients that were on care/treatment in the clinics at the time of this study due to poor data management, we decided to use all the patients that came to the clinics during the period of data collection. The patients were recruited consecutively into the study as they were coming to the clinics. All the selected participants were adequately informed about the survey, and their individual verbal and written informed consents were obtained. A pretested interviewer-administered questionnaire was used to obtain information on the participants' sociodemographic data, pretest and posttest HIV counseling information, and the various forms of stigma and discrimination experienced by the respondents. About 50 questionnaires were administered every week by 6 recruited and trained research assistants. The data obtained were analyzed using Epi-Info 2005 statistical soft ware.
Result
A total of 300 respondents were interviewed from the 3 ART clinics within University of Ilorin Teaching Hospital (UITH). The questionnaires used were interviewer-administered, and all were returned, giving 100% response rate.
The mean age of the respondents was 39.04 years (SD = 9.32 years) with a range of 19 to 65 years. The modal age group was 35 to 39 years and 84.3% of the respondents were below 50 years of age. About two thirds (64.7%) of the respondents were females, while 35.3% of them were males. About three quarters (73.3%) of the respondents were Yoruba by tribe. Majority (62.7%) of the respondents were married, 17% of them were widowed, 9.3% were single, 6.0% were divorced, and 5.0% were separated. Thirty-two percent (32.0%) of the respondents had primary education, 29.3% had secondary education, 25.0% of them had tertiary education, while the remaining 13.7% had no formal education. The predominant occupation of the respondents was trading or business (39.7%), followed by civil service (19.3%), artisan (13.0%), driving (5.7%), farming (4.0%), and others (4.3%).
Muslims constituted 52.3% and Christians 47.7% of the respondents. Majority (62.9%) of the married respondents came from monogamous family settings (see Table 1 ). Fifty-two percent (52.0%) of the respondents were diagnosed to be HIV positive 1-to 3 years ago; nearly 40% were diagnosed less than a year ago, while 8.0% and 1.3% were diagnosed 4–6 years and over 6 years ago, respectively.
Sociodemographic Variables N = 300

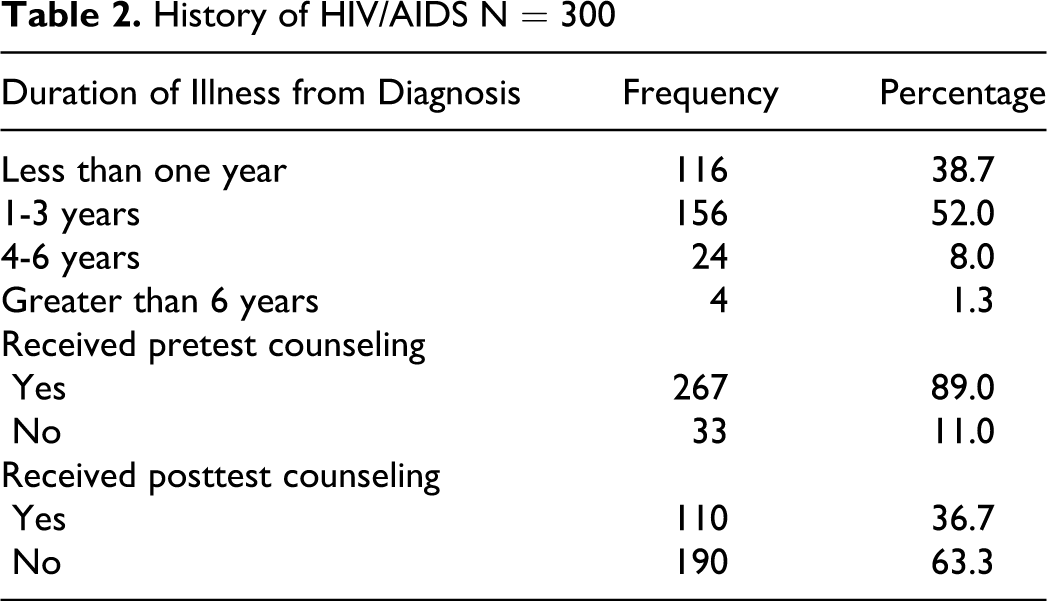
As much as 52.7% of the respondents were informed before they were being tested for HIV, while the remaining 47.3% got to know that they were tested for HIV after the result came out. Nearly two third (63.3%) of the respondents were not counseled before they were being tested for HIV. However, about 90% of the respondents had posttest counseling, while the remaining 10% were not counseled after they were tested HIV-positive (see Table 2 ). The first reactions of the respondents to their positive HIV status varied. More than half of the respondents(56.3%) felt bad and broke down with emotion, about one third took it in good faith, some denied the diagnoses, others reacted by attempted suicide and refusal to eat for some days (see Table 3 ).
History of HIV/AIDS N = 300
Stigma and Discrimination
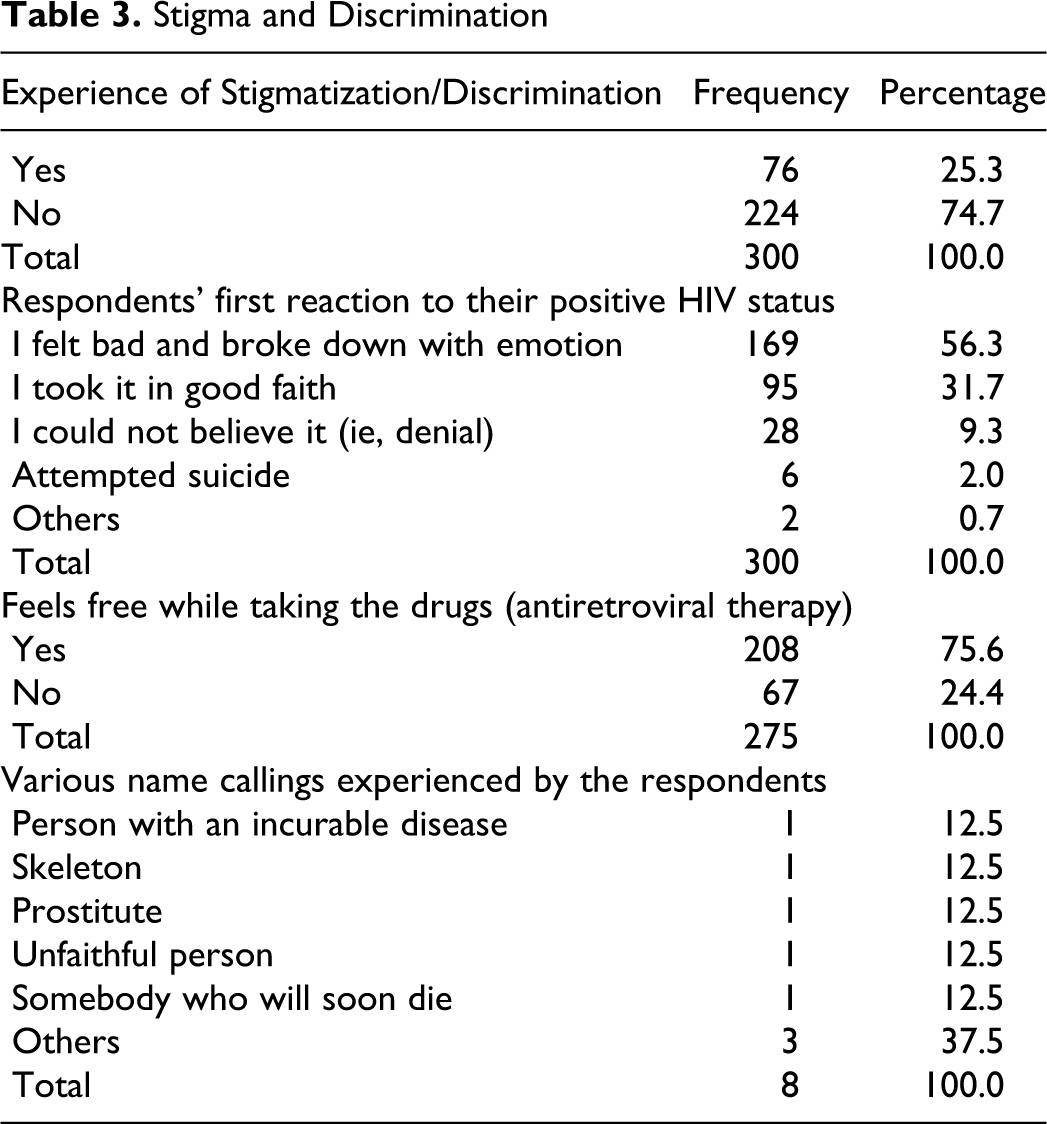
One quarter of the respondents had experienced stigma or discrimination (ie, unfair treatment) due to their positive HIV status. The commonest form of stigma faced by the respondents was blame for being responsible for their positive HIV status, followed by violation of confidentiality. Others were being told that their HIV status is a punishment from God, that they are no more useful to anybody and various name-callings (see Tables 3 and 4 ).
Various Forms of Stigma Experienced by the Respondents

The findings in this study revealed that disclosure of 7.3% of respondents' HIV status without their permission was caused by their family members. Violation of confidentiality of 4.7% of the respondents was by health workers. Religious group leaders were also reported to violate the confidentiality of the respondents (see Table 4). This study found out that about one quarter of the respondents on antiretroviral therapy did not feel free to take their drugs (see Table 3), they either hide it when people are coming or remove it from its container and put it in another one to prevent people from knowing they are HIV-positive.
Various forms of discriminating attitude exhibited by health workers when the respondents were seen by them included selective use of gloves or use of extra gloves (13.3%), provision of poor quality of care (4.3%), isolation from other patients (3.3%), charging them more than other patients (3.0%), and refusing to provide care, treatment, and support (2.7%; see Table 5 ).
Forms of Discrimination Faced by the Respondents at Various Levels

At the family or community level, forms of discrimination faced by some of the respondents included denying them support, social isolation, restricting their participation in local or family events, and violence against them (see Table 5). Others included public disclosure of a respondent’s HIV status by his father, friends running away from some of them, separation of a respondent’s things from others'. One of the respondents experienced threat of expulsion from her brother’s house, withdrawal of her baby from her, preventing her from watching television with others in the family, and locking her up in a room to die there (see Table 6 ). Respondents also faced refusal of the family members to share cutleries, bedding or sleeping space, cooking utensils, toilet facilities, and seats with them (see Table 5).
Other Forms of Discrimination Faced at the Family/Community Level

Two (0.7%) of the respondents reported refusal to hire them by other employers, while one (0.3%) of the respondents each, reported refusal of his coworkers to work with him, dismissal from the place of work due to positive HIV status, violation of confidentiality, and social isolation (see Table 5).
This study also showed that discrimination against PLWHA also takes place in the religious group. The findings in this study show that respondents were faced with restricting access to marriage, denying participation in religious activities, isolation by other members, and name calling (see Table 5).
Relationship between Other Variables and HIV/AID-Related Stigma and Discrimination
The influence of other variables on HIV/AID-related stigma and discrimination was investigated by running a statistics of association (using chi-square) on each of the variables and experienced stigma/discrimination. The only one with significant level of association with stigma/discrimination was status disclosure to at least 1 person (P = .001), the others including sex, social status, educational status, religion, family type, tribe, age, and others were not statistically significant (P > .05).
Discussion
Findings from this study showed that PLWHA faced stigma and discrimination at all levels of the society (even in the heath care settings). These findings are supported by findings in similar studies conducted in other African Countries which showed that people living with HIV experienced stigma and discrimination at all levels of the communities.13–17 One quarter (25%) of the respondents had experienced stigmatization and discrimination (ie, unfair treatment) due to their positive HIV status. This finding is lower than findings from similar studies conducted in South Africa and Kenya, which found stigma and discrimination rates of 40% and 43%, respectively.4,18
If HIV testing without patient’s informed consent is included, nearly half (46%) of the respondents would have experienced stigma. The rate of stigmatization and discrimination experienced by the respondents might be more than the finding in this study, if majority of the respondents had disclosed their HIV status beyond their families. Another thing that may be responsible for this low rate is presence of HIV in both couples (concordant sero-status among couples in the studied population), since most of the respondents were married and many of them had HIV-positive spouses.
The commonest form of stigma faced by the respondents was blame for being responsible for their positive HIV status, followed by violation of confidentiality. Others were telling them that their HIV status is a punishment from God, saying that they are no more useful to anybody and various name-callings. These findings are supported by finding from a similar study conducted in Enugu 19 which revealed that people still believe that PLWHA are being cursed by God for their sins. This implies that stigma associated with HIV and AIDS occurs everywhere in the country.
The findings in this study revealed that disclosure of 7.3% of respondents' HIV status without their permission was caused by their family members. Violation of confidentiality of 4.7% of the respondents was by health workers, this is in agreement with the finding in a similar study, 20 which reported 5% for violation of PLWHA confidentiality by health workers. A study conducted in South Africa 21 also found out that “the common human right violation of PLWHA included disclosure of one’s HIV status without consent, and often the worst human right violators were family members and health care workers.21,22 Religious group leaders were also reported to violate the confidentiality of the respondents. This implies that if this continues unchecked, PLWHA may find it difficult to disclose their HIV status. Another implication of these findings is that there is a need to educate people at all levels of the society (including the religious leaders) on HIV and AIDS, and rights of PLWHA.
This study found out that about one quarter of the respondents on ART were not feeling free to take their drugs, they either hide it when people are coming or remove it from its container and put it in another one to prevent people from knowing they are HIV-positive. This perception of these respondents who were not free taking their drugs shows the degree of self-stigmatization the PLWHA are going through and also the possible effect of stigma and discrimination on adherence of PLWHA to ART. This finding is consistent with finding from a similar study conducted in 5 African Countries that showed correlation between HIV/AIDS-related stigma and ART adherence. 23 It also revealed the psychological trauma that PLWHA may be going through because of the stigma and discrimination associated with HIV and AIDS.
The study showed that discrimination against PLWHA persists at all levels of the society. Various forms of discriminating attitude exhibited by health workers when the respondents were seen by them included selective use of gloves or use of extra gloves (13.3%), this finding is different from that of a similar study in Abuja, Nigeria, some years back, which showed that 61% of the respondents experienced selective use of gloves when they were seen by health workers. 20 This difference may be due to various campaigns and training on HIV and AIDS that had taken place between the periods of these 2 studies. Other forms of discrimination experienced by the respondents from health care givers included provision of poor quality of care (4.3%), isolation from other patients (3.3%), charging them more than other patients (3.0%), and refusing to provide care, treatment, and support (2.7%). These findings are different from the findings in a similar study conducted in Nigeria some years back by the physicians for human rights 20 (which showed use of extra glove [61%], charging them more than other patients [26%], separating them from other patients [11%], and refusal of admission [6%]). 24 These differences may be due to the fact that the latter study was carried out some years back, and a lot of training and campaigns on HIV and AIDS, and HIV-related stigma and discrimination had taken place between the 2 periods. Similar surveys conducted in Adamawa, Lagos, and Port Harcourt 8 revealed that fear of stigmatization or discrimination at all levels of health care was a great obstacle to PLWHA’s access to health care. Another study conducted by FMOH also showed that discrimination against PLWHA is a common practice in many health facilities. 8 Several similar studies conducted in other African Countries and other parts of the world also showed that PLWHAs experienced stigma and discrimination in the health care settings.14,16,17,25–32 The implication of these findings is that because of stigma and discrimination in health care settings, PLWHA may be given substandard care, treated with disdain, face limited access to services, or avoid services all together. If these attitudes continue in the health care settings, it will be difficult to control HIV and AIDS.
Forms of discrimination faced by some of the respondents at the family or community level included denying them support, social isolation, restricting their participation in local or family events, and violence against them. Others included public disclosure of a respondent’s HIV status by his father, friends running away from some of them, and separation of a respondent’s things from others'. One of the respondents experienced threat of expulsion from her brother’s house, withdrawal of her baby from her, preventing her from watching television with others in the family, and locking her up in a room to die there. This finding is supported by findings in similar studies in other African Countries that revealed both verbal and physical abuse of PLWHA at the family/community level.14,33 Respondents also faced refusal of the family members to share cutleries, bedding or sleeping space, cooking utensils, toilet facilities, and seats with them. These findings show that despite the possibility of the family to support its members in all situations (including HIV and AIDS), there is still discrimination against PLWHA at the family level. Full community participation at all levels of HIV and AIDS programmes is needed to reduce discrimination faced by PLWHA at family/community level.
Two (0.7%) of the respondents reported refusal to hire them by other employers, while one (0.3%) of the respondents each, reported refusal of his coworkers to work with him, dismissal from the place of work due to positive HIV status, violation of confidentiality, and social isolation. This low prevalence of stigma and discrimination at place of work may be due to the fact that majority of the respondents did not disclose their HIV status at their places of work. Discrimination at the place of work is likely to make it very difficult for PLWHA to cope with HIV and AIDS because most of the affected persons (as revealed by this study and others8,24,34,35) were in the working class.
This study also showed that discrimination against PLWHA takes place in the religious groups. The findings in this study show that respondents were faced with restricting access to marriage, denying participation in religious activities, isolation by other members, and name calling. This finding is supported by a similar study conducted in Tanzania which also reported discrimination against PLWHA by religious leaders. 16 The implication is that religious groups and their leaders need be involved in planning and implementation of HIV and AIDS control programmes. Another implication of the findings is that spiritual support which is an important part of chronic care of HIV and AIDS may be difficult to access by the PLWHA.
Conclusion and Recommendations
The study showed that discrimination against PLWHA persists at all levels of the society, and is an all pervading phenomenon. The more stigmatization and discrimination against PLWHA persist, the more difficult it will be to successfully prevent, control, and eradicate HIV and AIDS in the society. This is because many PLWHAs will not be identified if they are not shown love and care. Therefore, government at all levels should develop and implement programs to educate health care providers about HIV and AIDS, ethics, and treatment and care of HIV/AIDS patients. Government should also educate the general population on HIV and AIDS, put in place policies that will reduce/stop HIV-related stigma and discrimination at all levels of the society, educate PLWHA on their right to live and work without discrimination, and ensure full community participation in HIV control programs. The PLWHA should also be encouraged to seek legal redress anytime their fundamental rights are infringed upon.