
Abstract
The purpose of this pilot randomized controlled trial is to assess the feasibility and impact of a triweekly 12-week yoga intervention among people living with HIV (PLWH). Additional objectives included evaluating cognition, physical function, medication adherence, health-related quality of life (HRQoL), and mental health among yoga participants versus controls using blinded assessors. We recruited 22 medically stable PLWH aged ≥35 years. A priori feasibility criteria were ≥70% yoga session attendance and ≥70% of participants satisfied with the intervention using a postparticipation questionnaire. Two participants withdrew from the yoga group. Mean yoga class attendance was 82%, with 100% satisfaction. Intention-to-treat analyses (yoga n = 11, control n = 11) showed no within- or between-group differences in cognitive and physical function. The yoga group improved over time in HRQoL cognition (P = .047) with trends toward improvements in HRQoL health transition (P =.063) and depression (P = .055). This pilot study provides preliminary evidence of feasibility and benefits of yoga for PLWH.
Background
The most recent estimates indicate that 36.9 million people worldwide are living with HIV. 1 The highest percentage of people living with HIV (PLWH) is in sub-Saharan Africa, having 53% of the global prevalence. 2 Those at risk of HIV transmission include women, men who have sex with men, transgender individuals, people who use drugs, and sex workers. 3
Approximately 15% to 69% of PLWH worldwide experience some form of cognitive impairment, 4 -7 presenting as deficits in attention, memory, and executive function. 8,9 There are sex differences in cognitive performance among PLWH, with women scoring lower on tests of attention, processing speed, executive function, and fine motor performance than men. 10 In addition to cognitive impairment, balance and gait deficits are common among PLWH 11 and are associated with elevated fall risk and mortality. 12 Some evidence has emerged to indicate that a relationship exists between physical and cognitive performance in this population. 13
What Do We Already Know about This Topic?
Yoga has been shown to improve cognition and balance among HIV-negative individuals.
How Does Your Research Contribute to the Field?
This trial was feasible and the 12-week yoga intervention provided benefits to self-reported cognition among people living with HIV.
What Are Your Research’s Implications toward Theory, Practice, or Policy?
This study can inform clinicians and researchers about the feasibility and potential efficacy of a yoga intervention in improving self-reported cognition among people living with HIV.
Mind–body exercise is a type of therapy, such as Tai Chi and yoga, which includes concentration, breathing, and body movement. 14 These interventions can have a positive effect on cognitive performance among older adults without HIV. A recent meta-analysis of 32 randomized controlled trials (RCTs) evaluated mind–body interventions (of which, 8 RCTs included a yoga intervention), showing significant improvements in overall cognitive performance, working memory, verbal fluency, cognitive flexibility, and learning among older adults. 14 Another meta-analysis of 11 RCTs (4 RCTs with yoga interventions) conducted with older adults determined that mind–body exercise had a positive effect on overall cognition, memory, executive function, learning, and language. 15 A prominent theory explaining these cognitive benefits with yoga includes the downregulation of the stress response and upregulation of the parasympathetic nervous system. 16,17 No RCTs to date have evaluated the impact of a yoga intervention on cognitive performance outcomes among PLWH.
Over half of PLWH in Western countries have sought complementary or alternative therapies, which include mind–body interventions such as yoga and Tai Chi. 18 -20 Some authors have evaluated the impact of Tai Chi on health-related quality of life (HRQoL) and mental health in this population. A single-group observational study conducted with male (n = 35) and female (n = 24) PLWH reported a positive effect of Tai Chi on HIV-related psychological distress in addition to emotional, social, and overall HRQoL. 21 An RCT of 38 male individuals living with AIDS conducted by Galantino and colleagues in the United States found significant improvements in overall HRQoL in both aerobic exercise and Tai Chi groups versus controls. 22
Randomized controlled trails and meta-analyses have also demonstrated positive effects of yoga on affective outcomes such as HRQoL and mental health among PLWH. An RCT demonstrated significant improvements in anxiety, depression, fatigue, well-being, and quality of life in a sample of mostly female PLWH who participated in an integrated yoga intervention compared to controls following an 8-week intervention. 23 Another RCT demonstrated positive effects on HRQoL and mental health among mostly female PLWH following a 12-week Sudarshan Kriya yoga intervention compared to controls. 24 However, the intervention did not include a physical activity component, and PLWH taking antiretroviral medications were excluded from the study. 24 An RCT with a 1-month integrated yoga intervention conducted with male (n = 24) and female (n = 20) PLWH showed a significant reduction in depression scores among yoga participants compared to controls. 25 A meta-analysis of 7 RCTs conducted with PLWH determined that yoga interventions resulted in large improvements in perceived stress, positive affect, and anxiety compared to controls. 26 Finally, a systematic scoping review of 84 studies showed that mindfulness, relaxation techniques, cognitive–behavioral strategies, and yoga had beneficial effects on HRQoL and physical and psychological symptoms among PLWH. 18
Emerging evidence also suggests that mind–body exercise can improve physical performance among PLWH. Participants in the abovementioned RCT by Galantino and colleagues who performed aerobic exercise and Tai Chi had significant improvements in balance using the functional reach test. 22 Kietrys and colleagues also observed improvements in gait and balance with their integrative yoga intervention among 2 of 3 case series participants. 27 Yoga has the potential to address both physical and cognitive impairments in this population. However, no RCTs to date have evaluated the feasibility and impact of yoga on cognitive and physical outcomes among PLWH.
Women are frequently underrepresented in health research, particularly in HIV trials. 28 To address this gap, the Sex and Gender Equity in Research (SAGER) guidelines recommend authors report how sex (biological attributes) and gender (socially constructed roles, behaviors, and identity) factor into the study design and present study data disaggregated by sex and gender if possible. 29 As such, we discuss and evaluate the role of sex and gender in this study where applicable.
Purpose, Objectives, and Hypothesis
Our overall goal is to inform the design of a future, full-scale, multisite, community-based RCT to evaluate the effects of yoga on cognitive and physical function among PLWH from Halifax, Nova Scotia, Canada. Our primary objective is to assess the feasibility of a 12-week yoga intervention for PLWH in terms of participant recruitment, assessments, safety, adherence, and satisfaction with the intervention. Our second objective is to evaluate the effect of a 12-week yoga intervention (yoga group) versus usual care (control group) on cognitive performance and self-reported cognition among PLWH. Our third objective is to compare the effects of the yoga intervention versus control on balance, walking speed, mental health, medication adherence, physical activity, and HRQoL outcomes among PLWH. The fourth objective is to explore the relationships between cognitive performance and self-reported cognition, physical activity, and balance performance. Our alternative hypotheses were as follows: (1) The yoga group would experience larger improvements in cognitive performance and self-reported cognition than the control group and (2) the yoga group would experience larger improvements in physical function, HRQoL, and mental health outcomes than the control group.
Methods
We designed a pilot RCT. The Consolidated Standards of Reporting Trials (CONSORT) checklist for pilot and feasibility studies 30 is given in Supplemental Appendix 1.
Participants
The CONSORT 31 diagram in Figure 1 shows the flow of participants through this randomized, 2-parallel group, pilot trial. Participants were included in the study if they were aged 35 years or older, identified cognitive concerns on the Communicating Cognitive Concerns Questionnaire (C3Q) with a cutoff of 35 points or less at baseline, 32 lived in the Halifax Regional Municipality of Nova Scotia, Canada, were able to provide informed consent, and were medically stable as determined by the Physical Activity Readiness Questionnaire Plus. 33 People living with HIV already participating in regular yoga classes were excluded. We recruited participants from community and health organizations in Halifax, Canada, using posters, newsletters, and clinic staff assistance. We attempted to obtain a diverse sample in terms of ethnicity and gender by using snowball sampling techniques.

CONSORT flow diagram.
Study Procedures
Study procedures were in accordance with institutional ethical standards and the Helsinki Declaration (2013). The study methods are described in detail elsewhere. 34 In summary, individuals wanting to participate contacted the study coordinator who conducted a screening assessment to confirm eligibility; explained the study’s purpose, procedures, risks and benefits, and time responsibilities of the study; reviewed the consent form; and answered questions. Those who agreed to participate in the study signed the consent form and underwent the baseline assessment. Thereafter, participants were randomly assigned in a 1:1 ratio to the yoga or control group. Group assignment was determined by a random computer generator and was concealed in individual, opaque envelopes by a person not affiliated with the study. The study coordinator opened the envelopes after completion of the baseline assessment. Assessors blinded to group allocation conducted the postintervention assessment 12 weeks later. We instructed participants to avoid revealing their group allocation to assessors. To determine the effectiveness of the blinding process, we asked the assessors at study completion if they knew the group assignment of participants, and if they did not know, to guess the group to which the participant had been assigned.
Intervention Protocols
Participants in the yoga group engaged in group-based Hatha yoga classes for 60 minutes, 3 times weekly for 12 weeks at a yoga studio. Hatha yoga has many variants forms of yoga including Iyengar, Vinyasa, and Ashtanga, 35 with considerable variation between and within types. 36 Our yoga program incorporated common components of Hatha yoga: asanas (physical poses or postures), meditation (dhyana), breathing exercises (pranayama), the study of introspection or self-study (swadhyaya), and spiritual discourse (satsang). 35,37 Classes began with 15 minutes of seated meditation; breathing exercises; shoulder, neck, and back stretches; and sun salutations (either in seated or standing). This was followed by 10 minutes of standing poses, 15 minutes of balance poses, and 10 minutes of abdominal and back-bend poses. All classes finished with 10 minutes of cool-down stretches and final rest (savasana). Classes were adapted to all ability levels by providing modifications to physical postures and assistive props. At the yoga classes, participants were provided with yoga mats, chairs, bolsters, blocks, straps, and blankets. To honor the Mi’kmaq peoples, on whose ancestral land the classes were conducted, an Indigenous elder performed brief monthly smudging ceremonies (the burning of plants such as sage or sweetgrass for purification 38 ) at the yoga studio. Participants were not explicitly encouraged to practice at home. We directed control participants to maintain their usual physical activity levels during the study.
Participants were given CAD$50 honoraria at baseline and final assessments. We offered bus tickets and parking reimbursements for assessments and bus tickets for those attending the yoga classes. We provided child care reimbursement to those in the yoga group to address participation barriers, which are prevalent among female participants. 39
Outcome Measures
We assessed the feasibility of the trial by measuring participant recruitment, assessments, safety, adherence, and satisfaction with the intervention. Participant recruitment measures (including reasons for not participating and recruitment time), assessment duration, adverse events, and adherence (number of yoga classes attended) were recorded. An a priori target for adherence to determine whether to proceed with a large-scale RCT was that participants attend at least 70% of the yoga classes. The postparticipation satisfaction questionnaire consisted of 7 Ordinal scale questions ranging from strongly disagree (1) to strongly agree (5) and 6 open-ended questions. The a priori target for participant satisfaction was that a minimum of 70% of participants would indicate they were satisfied with the intervention, as determined by achieving scores of ≥4 on the Ordinal scale for each item on the postparticipation questionnaire. The questionnaire was administered to yoga participants at study completion.
Study assessments included a demographic questionnaire administered at baseline (age, gender, ethnicity, education, employment, CD4 count, viral load, time since HIV diagnosis, number of comorbidities, and antiretroviral medication use). We administered the following performance-based measures and paper-based self-reported questionnaires at baseline and 12 weeks: the Brief Cognitive Ability Measure (B-CAM), 40,41 a computerized measure of cognitive performance, with higher scores reflecting better cognitive ability; the C3Q, 32 an HIV-specific self-reported cognitive questionnaire, with higher scores indicating fewer cognitive difficulties; Community Balance and Mobility Scale (CB&M), 42 a measure of dynamic balance performance where higher scores indicate better balance performance; the 10-m walk test, an objective test of comfortable and fast gait speed 43 ; the Rapid Assessment of Physical Activity (RAPA) questionnaire, a 2-part, self-reported questionnaire where RAPA 1 indicates aerobic physical activity levels and the RAPA 2 indicates resistance and flexibility activities 44 ; accelerometer data (Fitbit) including steps per day and number of kilometers walked 45 ; the Simplified Medication Adherence Questionnaire (SMAQ), a self-reported antiretroviral medication adherence measure 46 ; the Medical Outcomes Survey-HIV (MOS-HIV), a self-reported HRQoL questionnaire developed for PLWH with 11 subscales (physical function, social function, role function, cognitive function, pain, mental health, energy, health distress, quality of life, general health, and health transition) 47 ; and the Hospital Anxiety and Depression Scale (HADS-A and HADS-D), a self-reported mental health questionnaire. 48
Data Collection and Analysis
Study data were collected at Dalhousie University in Halifax, Nova Scotia, and were recorded using Research Electronic Data Capture (REDCap) software. 49 The authors will provide access to the data if requested. All outcomes were assessed for missing data. Results were analyzed and reported by gender, as recommended by the SAGER guidelines. 29 Although sample size calculations are not recommended for pilot studies, 30 we targeted a sample size of 25 participants in total in order to inform future sample size calculations.
Primary Outcomes
We analyzed Ordinal postintervention questionnaire responses descriptively and open-ended responses using inductive thematic analysis. 50
Descriptive Statistics
Means, mean change, and 95% CIs were calculated separately for the intervention and control groups as per the CONSORT guidelines. 30 Floor and ceiling effects were assessed and calculated for the CB&M by taking the proportion of the sample that scored the minimum or maximum scores.
Second and Third Outcomes
We used intention-to-treat and per-protocol approaches for our second and third outcome analyses. Spearman correlation coefficients were used to evaluate the relationship between outcomes, with 0.1 to 0.3 representing weak associations, 0.4 to 0.6 representing moderate correlations, and 0.7 to 0.9 representing strong associations. 51 We performed independent t tests, χ2, or Fisher exact tests on demographic variables and baseline dependent measures, as appropriate.
We evaluated the data to determine whether they met the assumptions for parametric tests. If the assumptions for parametric tests were not met, we used nonparametric tests or bootstrapping. Bootstrapping is a nonparametric approach to hypothesis testing that is recommended for small samples that do not meet the assumption of normality. 52,53 This process generates an estimate of the sampling distribution of a statistic (such as the standard error or CI) by performing repeated random resampling from the available data and estimating bias-corrected and accelerated coefficients and P values. 52,53 We then analyzed secondary and tertiary outcomes using univariate analysis of covariance (ANCOVA) with bootstrapped CI, mixed ANCOVA, or Wilcoxon signed rank tests. Two-sided tests with a minimum α level of .05 were used for all analyses using SPSS version 25 (IBM, 2017). 54 We calculated effect sizes using partial η2 for parametric and r for nonparametric tests, with 0.1 representing a small effect, 0.3 representing a moderate effect, and 0.5 representing a large effect. 55 -57 We also conducted a separate analysis with gender as a covariate to determine its effect on all secondary and tertiary outcomes.
Supplementary Analyses (Fourth Objective)
We performed a moderator analysis to determine the effect of the interaction between baseline cognitive and balance performance on cognitive performance at study completion.
Ethical Approval and Informed Consent
We obtained ethics approval through the Nova Scotia Health Authority (protocol reference #1022158) and the study was registered on clinicaltrials.gov (NCT03071562). Written informed consent was obtained prior to enrollment in the study.
Results
Sample Characteristics
The characteristics of the sample are summarized in Table 1.
Characteristics of the Sample at Baseline (n = 22 Participants).

a Significant difference (P < .05). Undetectable viral load is defined as <50 copies of HIV per milliliter of blood.
b Refers to Indigenous people who identify fluid gender roles and sexuality beyond the Western binaries of male/female and homosexual/heterosexual. 58
Participants were on average 55.5 years old (SD = 10.7) and had been living with HIV for a mean of 20.1 years (SD = 13.0). Most (86%) participants were taking antiretroviral medication, were virologically suppressed (84%), and were not immunocompromised, with a mean CD4 count of 515.5 (SD = 231.4). Participants mostly identified as male (68%) and Caucasian (73%), with some education (59% had some high school education or a high school diploma), and were not currently working (68% were not working, retired, or studying). The 2 groups differed at baseline in cognitive performance (B-CAM) and age; therefore, these variables were included as covariates in all parametric analyses to control for group imbalances.
Feasibility Outcomes (First Objective)
We approached 29 individuals to participate in the study. All were eligible and 22 (76%) agreed to participate over a 23-month recruitment period. Five individuals gave no reason for declining to participate, 1 person did not wish to practice yoga, and 1 individual reported a lack of time. We did not achieve our initial goal to reach 25 participants, as recruitment slowed during the summer months and Halifax has a small HIV community. The blinded assessors reported that they were unaware of group allocation of any participant at follow-up.
Assessments took less than 2 hours to complete and study assessors deemed them to be feasible. One minor musculoskeletal injury occurred as a result of the balance assessment. There were no known injuries associated with the yoga intervention. Two (9%) participants withdrew from the yoga group. Reasons for drop-out included illness and relocating out of province. None of the participants withdrew from the control group. Mean attendance to total yoga classes was 82% (mean attendance = 29.4/36 classes), and 89% (8/9) of participants in the yoga group met the a priori adherence criterion. One participant was unable to attend some classes at the yoga studio; therefore, the participant was offered taped or live virtual classes, which the participant accepted.
Nine participants had difficulties syncing their accelerometers as many did not have access to smartphones or computers. As a result, the study coordinator met with participants to sync their devices with a study computer.
Quantitative Satisfaction Questionnaire responses
From the 9 participants in the yoga group, 100% enjoyed the sessions, 100% felt there was some benefit from participating in yoga, 100% felt safe during the sessions, and 100% agreed or strongly agreed that they felt comfortable during the yoga sessions. One minor musculoskeletal injury occurred as a result of the balance assessment. There were no known injuries associated with the yoga intervention. The blinded assessors reported that they were unaware of group allocation of any participant at follow-up.
Qualitative Satisfaction Questionnaire responses
Five themes regarding benefits of the yoga intervention emerged from the open-ended postparticipation questionnaire responses: cognitive function, mental health, sleep, quality of life, and social interaction. Improved thinking was identified by 6 participants; one participant said, “[I’m] remembering pills,…remembering to pick stuff up at the store.” Five of 9 participants in the yoga group reported stress relief or decreased depression as a benefit to the intervention. One participant said, Doing the yoga sessions gave me new skills to deal with every day stresses and participating gave me something to look forward to weekly…I appreciate this study because it was something that had immediate results. It was something for “me” and right from the beginning, it felt less of a research project and more of a therapy course.
Descriptive Statistics
There were no missing data for the second, third, or fourth outcomes. The B-CAM, Comfortable and Fast Gait Speed, and MOS-HIV General Health, Mental Health, and Energy subscales met the assumptions for parametric tests, while the other outcomes did not. Mean B-CAM scores in the overall sample at baseline were 19.0 ± 4.6 and 19.6 ± 5.3 at study completion. The mean C3Q scores of the overall sample were 24.6 ± 8.1 at baseline and 25.7 ± 6.5 at 12 weeks.
Mean overall CB&M scores at baseline were 67.1 ± 22.3 and 68.7 ± 22.5 at 12 weeks. The mean score on the CB&M in the overall sample (including baseline and final scores) was 67.9 ± 21.1 (range = 22-96). One participant (2.38% of 42 observations) obtained a maximum score of 96 on the CB&M, and none of the participants obtained the minimum score of 0.
Effect of the Intervention
Results of the intention-to-treat analyses (n = 22) are reported. When we reanalyzed the data using per-protocol analyses, we found no differences in the results unless otherwise stated. We found no significant effect of gender between groups on all outcomes.
Cognitive performance (second objective)
A summary of results for cognitive performance is listed in Table 2. There were no significant between-group effects of the yoga intervention on the B-CAM scores at study completion, F 1, 16 = 0.687, CI: −1.164 to 5.718, P = .353. There were also no within-group differences on the B-CAM scores over time, as determined by the mixed ANCOVA, F 1, 17 = 1.769, CI: −2.979 to 0.746, P = .201. Self-reported cognition (C3Q) scores did not differ significantly between the groups at study completion, F 1, 16 = 0.002, CI: −8.362 to 8.563, P = .965. There were also no significant within-group differences in C3Q scores (yoga group Z = −0.983, P = .326; control group Z = −0.089, P = .929). Figure 2 shows pre- and post-intervention scores on the B-CAM, C3Q, and CB&M.
Cognitive Outcomes.

Abbreviations: B-CAM, Brief Cognitive Ability Measure; C3Q, Communicating Cognitive Concerns Questionnaire.
a Bootstrap values are bias corrected and accelerated based on 1000 bootstrap replications. Effect sizes are
Third Objective Outcomes
Physical performance and physical activity outcomes
Physical performance and physical activity results are summarized in Table 3. There were no significant within- or between-group differences in balance or gait speed. We did not observe between-group or within-group differences in physical activity as measured by the RAPA and accelerometer data.
Physical Performance and Activity Levels.
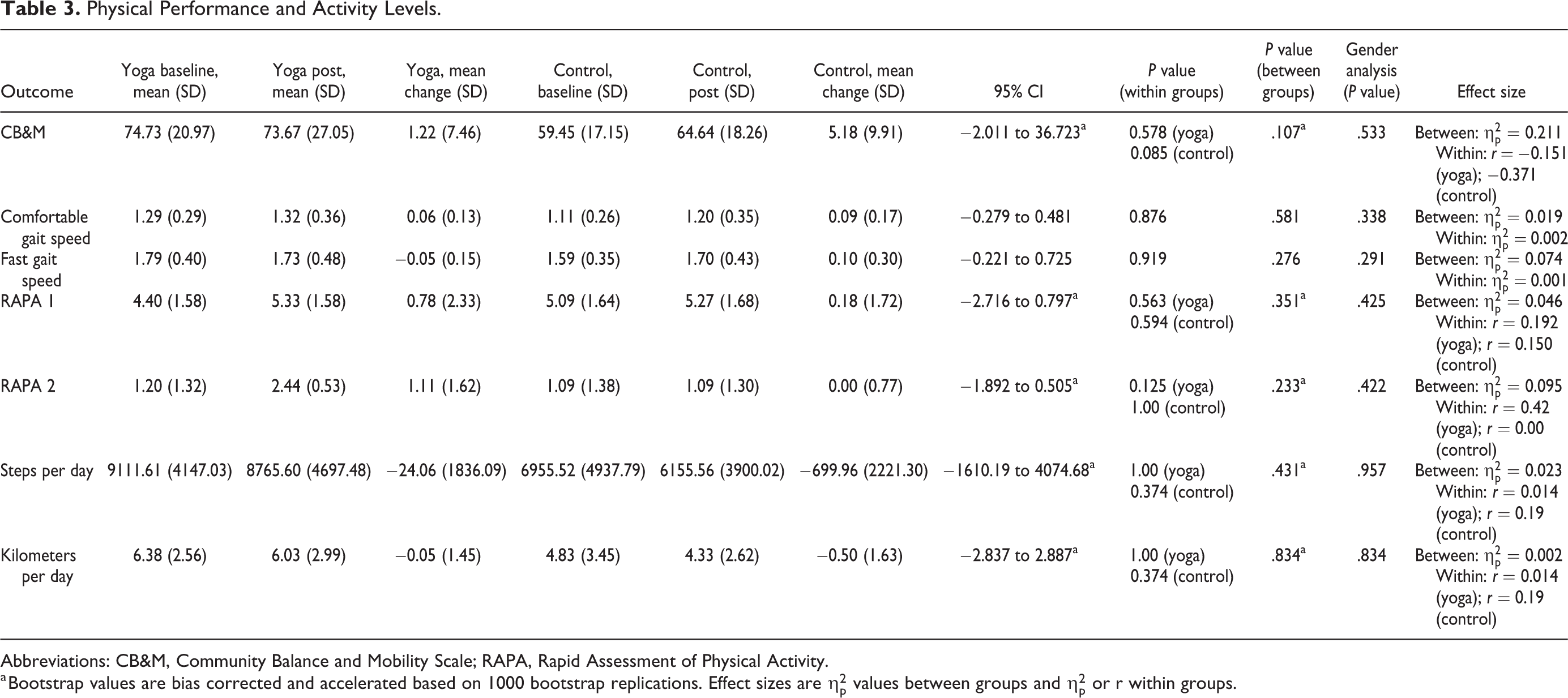
Abbreviations: CB&M, Community Balance and Mobility Scale; RAPA, Rapid Assessment of Physical Activity.
a Bootstrap values are bias corrected and accelerated based on 1000 bootstrap replications. Effect sizes are

Pre- and postintervention scores of B-CAM, C3Q, and CB&M. B-CAM indicates Brief Cognitive Ability Measure; C3Q, Communicating Cognitive Concerns Questionnaire; CB&M, Community Balance and Mobility Scale.
Health-related quality of life, mental health, and antiretroviral medication adherence outcomes
Health-related quality of life and mental health results are displayed in Table 4. There were significant within-group differences in the MOS-HIV Cognitive subscale in the yoga group (Z = −2.120, P = .047) only. We also observed within-group difference trends among yoga participants on the MOS-HIV Health Transition (P = .063) and the HADS–Depression (P = .055) subscales. In contrast with the intention-to-treat analyses, per protocol analyses showed a trend in improved cognitive subscale scores (P = .094) and no trend in improved health transition scores among yoga participants (P = 0.125). We did not observe between-group differences on any other MOS-HIV subscales or the HADS questionnaire. There was no effect of the intervention on antiretroviral medication adherence at study completion using the SMAQ (χ = 1.650, P = .362).
Health-Related Quality of Life and Mental Health Outcomes.

Abbreviations: HADS, Hospital Anxiety and Depression Scale.
a Bootstrap values are bias corrected and accelerated based on 1000 bootstrap replications. Effect sizes are
b P < .05.
c P < .10 (trend).
Supplementary Analyses (Fourth Objective)
Associations with cognitive performance
We created a correlation matrix to determine the relationship between self-reported cognition (C3Q) and cognitive performance (B-CAM) scores, revealing that baseline C3Q was not associated with B-CAM scores at baseline (r = 0.262, P = .239). At study completion, however, C3Q was significantly moderately associated with B-CAM scores (r = 0.585, P = .007). Baseline balance (CB&M) scores were strongly associated with cognitive performance (B-CAM) scores at baseline (r = 0.843, P = .000) and final balance scores were associated with postintervention B-CAM scores (r = 0.612, P = .004). Physical activity was also related to cognitive performance in this sample. The number of steps at baseline was related to cognitive performance (B-CAM) at baseline (r = 0.685, P = .000) and study completion (r = 0.534, P = .015). Furthermore, baseline kilometers walked per day were associated with both baseline (r = 0.660, P =.001) and final B-CAM scores (r = 0.504, P = .023).
Moderator analysis
We found a significant interaction between CB&M and B-CAM scores at baseline in the prediction of B-CAM scores at follow-up in the yoga group (B −0.49, CI, −0.089 to −0.009, P = .026), but not the control group (B 0.002, CI, −0.046 to 0.050, P = .914).
Power Calculation for Future Trial
We performed a power analysis for cognitive performance (B-CAM) to determine the sample size for a future, full-scale RCT. The sample size for this effect size (
Discussion
Feasibility
This RCT was the first to evaluate the feasibility and impact of a 12-week yoga intervention on cognitive and physical outcomes among a sample of PLWH. The intervention was feasible as determined by reasonable assessment times, lack of known adverse events, adherence to the intervention, low attrition, and participant satisfaction. No known injuries occurred as a result of the yoga intervention, providing evidence that this is a safe form of exercise for PLWH. Furthermore, the participants reported 100% satisfaction and comfort with the intervention. Although we did not achieve the anticipated sample size within the time frame to conduct the study, we met the a priori targets for adherence and satisfaction, which indicate that a future large-scale RCT should be conducted. In order to meet recruitment targets, future RCTs evaluating cognitive and physical performance outcomes among PLWH should use multiple sites. Our findings can inform future power calculations for large-scale RCTs evaluating cognitive and physical outcomes among PLWH.
The rates of attrition (less than 10%) and adherence to the yoga classes (82%) in this study are encouraging and are likely due to high participant satisfaction. Three meta-analyses 59 -61 and 1 systematic scoping review 18 have identified high levels of withdrawal from exercise trials (20%-29%) and mind–body interventions (39%), as well as variable adherence (61%-100%) among PLWH to these interventions. Another study evaluated the feasibility of a yoga intervention for PLWH and observed similar feasibility outcomes to our study, reporting an average of 88% attendance to the classes and 83% retention at study completion. 62 However, retention in the control group was poor (50%) in the aforementioned study and the authors posited that this could be attributed to a lack of meaningful intervention. 62 In comparison, we had 100% retention in our control group at study completion, likely due to the short study duration and small time commitment.
Cognitive Performance
We found no significant improvement in cognitive performance following the 12-week yoga intervention. This finding is in keeping with those of McDermott et al, whose 16-week aerobic exercise intervention (n = 11) did not have an effect on cognitive performance among PLWH. 63 Evidence from the cross-sectional literature has showed positive associations between physical activity and better cognitive function among PLWH, 64 -71 but RCT evidence has yet to determine a causal relationship. There are a few potential reasons for the lack of effect of the intervention on cognitive performance in the present study. First, the small sample size was not sufficient to detect a change in outcomes. Second, there may have been some factors related to the dose of the intervention. For example, results from a meta-analysis of exercise moderators among older healthy adults indicate that more frequent (5-7 sessions per week) exercise sessions have larger benefits for cognitive performance than less frequent sessions (3-4 per week). 72 The intervention may also have been too short in total duration, as evidenced by a systematic review that determined that total exercise duration was the most potent predictor of cognitive performance and the authors recommended that exercise interventions for older adults last at least 52 hours in total. 73 Finally, the impact of social engagement on cognitive performance should be investigated further in the HIV population. Fazeli and colleagues performed a cross-sectional analysis and concluded that the combination of physical activity with social interaction and employment had a stronger impact on cognitive performance than each of these factors alone. 64 Future large-scale RCTs evaluating cognitive outcomes among PLWH should involve longer exercise interventions and active control groups.
Self-Reported Cognition
Despite the lack of improvement in objective cognitive performance in this sample, there were significant improvements over time on the Cognitive subscale of the MOS-HIV among yoga participants. This finding is surprising, as we did not observe concurrent improvements in self-reported cognition in the yoga group when measured using the C3Q. Both questionnaires have items measuring self-reported executive function, attention/concentration, and memory, but the items on the C3Q are more specific than those in the Cognitive subscale of the MOS-HIV, and the C3Q also includes items on language and motivation. 32 Self-reported cognition is an important clinical outcome in this population. As such, more research is needed to determine a gold standard measure of self-reported cognition among PLWH.
We observed significant improvements over time among yoga participants on the MOS-HIV Cognitive subscale with an intention-to-treat analysis, but no improvement when using a per protocol analysis. This is an unexpected result as intention-to-treat analyses are typically more conservative. 74 Our results may be explained by a participant in the yoga group who did not achieve the 70% adherence target but had improvements in self-reported cognition.
Health-Related Quality of Life and Mental Health
There were trends toward improvements in the MOS-HIV Health Transition subscale and Depression as measured using the HADS among yoga participants. We also found qualitative reports of improved social interaction among yoga participants. This evidence is in keeping with other literature evaluating the effect of mind–body interventions on HRQoL outcomes among PLWH. An observational study of male and female PLWH determined that Tai Chi benefited cognitive HRQoL as measured by the Functional Assessment of HIV Infection. 21 Another study found a positive effect of a yogic breathing and meditation intervention on the General Health, Social Function, and Cognitive Function subscales of the MOS-HIV among PLWH. 75 Galantino and colleagues observed within-group differences in their aerobic exercise and Tai Chi groups on health transition scores of the MOS-HIV, with no corresponding changes in the control group among men with AIDS. 76 Similarly, a pilot RCT determined that a meditation intervention enhanced HRQoL in a sample of mostly male PLWH. 77 In contrast, Agarwal et al 62 did not find an effect of yoga on HRQoL among mostly male PLWH as measured using the Short Form-36. However, the demographics between that study were different than the present study as their inclusion criteria were PLWH who used crack cocaine.
Physical Performance
There is some RCT evidence to indicate that yoga can improve balance among older adults without HIV. 78 -81 In fact, it appears that yoga is as effective as Tai Chi and balance training at improving balance performance among older fallers. 82 However, in the present study, we found no effect of yoga on dynamic balance. This lack of effect may be related to the variation in balance performance observed among some participants in the control group and the small sample size. No other studies have evaluated CB&M performance among PLWH, but baseline values in this study were lower than normative values for healthy adults in all age categories except one (ages 60-69). 83 To date, no balance measures have been validated with PLWH. Further research in this area is needed to investigate balance impairments and appropriate balance performance measures in this population.
Association between Cognitive and Physical Performance
The strong association between cognitive performance and balance found in this study is of interest, as this finding corroborates the results of other studies conducted with healthy older adults and individuals with mild cognitive impairment. A study conducted with older adults from South Africa showed a negative relationship between time taken to tandem walk (where the toes of the back foot touch the heel of the front foot during each step) for 10 m and the number of correct responses on the Stroop task, which is indicative of an association between physical and cognitive performance. 84 Another study conducted with healthy older adults from Malaysia determined that a positive relationship exists between dynamic balance and digit symbol test and matrix reasoning tests. 85 In the same study, an agility test predicted performance on cognitive tests such as the digit span test, clock drawing test, and the Mini Mental State Examination. 85 A study conducted with older adults with mild cognitive impairment determined that comfortable gait speed and Timed Up and Go performance were each associated with executive function performance using the Trails Making B test and the Stroop Interference test. 86 Among individuals with subcortical dementia, a reduction in gait speed is related to changes in subcortical structures, connections between frontal and subcortical structures, and subcortical neurotransmitters. 87
There is evidence of an association between physical and cognitive performance among PLWH as well. A large multisite study of 1549 mostly male PLWH and HIV-negative individuals reported that slowed gait was strongly associated with worse neuropsychological test scores. 13 Another study of 164 mostly female PLWH determined that motor impairment (as measured by the HIV Dementia Motor Scale), cognitive dysfunction, and cerebrovascular disease were related to each other at baseline. 88 The underlying pathology of this relationship is thought to include inflammation and underlying cardiovascular comorbidities. 88,89 Future work should evaluate the interaction between balance and cognitive performance among PLWH with a larger sample.
Study Limitations
There are several limitations to the present study that may have contributed to our findings. The principal investigator taught the yoga classes to the participants, which could bias the results. Recruitment was limited by the small number of PLWH in the geographical area. We also were only able to recruit 5 PLWHs who identified as female. Due to the small number of female and 2-spirited participants, it was not possible for us to report the results disaggregated by gender. Rather, gender was entered into the analyses for each variable as a covariate to determine whether differences existed between groups. As a result, sex and gender may have had an unknown effect on the uptake and impact of the yoga intervention. We also did not report study withdrawal by gender to avoid identifying participants. The small sample size may have negatively affected the process of randomization, as it is difficult to obtain equal groups, 90 which may have had a confounding effect on outcomes. Changes in medications, substance use, and other factors could have contributed to the variation in cognitive and physical performance observed in this sample. As such, stratification based on cognitive performance at baseline may be useful for future RCTs. Finally, the use of a passive control group limited our ability to determine the effect of social interaction on cognitive and affective outcomes.
Conclusion
This 12-week yoga intervention was feasible as determined by assessment protocols, adherence to yoga sessions, small attrition rates, and participant satisfaction. Our results indicate that a future multisite RCT is warranted. Future work should include an active control group and an intervention lasting at least 52 hours in total in order to investigate the effectiveness of yoga in this population. We found no significant differences in cognitive or physical performance between groups, but there was a significant improvement in MOS-HIV Cognitive subscale scores and trends toward improvements in HRQoL subscales and depression scores in the yoga group following the intervention. Future research should follow the SAGER guidelines and employ sex- and gender-based analyses in order to explore the impact of yoga interventions on health outcomes across different sexes and genders among PLWH.
Supplemental Material
Supplemental Material, CONSORT_extension_for_Pilot_and_Feasibility_Trials_Checklist_march21_2020 - Feasibility and Impact of a Yoga Intervention on Cognition, Physical Function, Physical Activity, and Affective Outcomes among People Living with HIV: A Randomized Controlled Pilot Trial
Supplemental Material, CONSORT_extension_for_Pilot_and_Feasibility_Trials_Checklist_march21_2020 for Feasibility and Impact of a Yoga Intervention on Cognition, Physical Function, Physical Activity, and Affective Outcomes among People Living with HIV: A Randomized Controlled Pilot Trial by Adria Quigley, Marie-Josée Brouillette, Jacqueline Gahagan, Kelly Kathleen O’Brien and Marilyn MacKay-Lyons in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Footnotes
Authors’ Note
This trial was registered on clinicaltrials.gov (NCT03071562). NCT03071562 https://clinicaltrials.gov/ct2/show/NCT03071562?term=NCT03071562&rank=1.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a Canadian Institutes of Health Research Catalyst Grant in HIV/AIDS Community Based Research (371452) and a Physiotherapy Foundation of Canada Neurosciences Division Award for Physiotherapy Research.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.