
Abstract
The population with HIV is aging and has unique health needs. We present findings from an evaluation of the geriatric-HIV program, Golden Compass, at San Francisco General Hospital. We used the implementation science framework, RE-AIM (Reach, Effectiveness, Adoption, Implementation, Maintenance) to guide the evaluation and used quantitative and qualitative methods to assess RE-AIM dimensions. From January 2017 to June 2018, 198 adults age ≥50 years participated in the program, with an estimated reach of 17%. Providers and patients indicated high acceptability of the program and were satisfied with clinics and classes. Colocation of services, specific pharmacy and geriatric assessments, and social support from classes were valued (effectiveness). Provider adoption was high, and the program was implemented as originally designed. Areas for improvement included challenges of framing aging services to patients. Future efforts will focus on expanding the reach of the program and examining long-term outcomes.
Keywords
What Do We Already Know about This Topic?
People living with HIV are aging, and new care models are needed to address the health needs of this population, including comorbidities and geriatric conditions.
How Does Your Research Contribute to the Field?
We describe the successes and challenges from the implementation of the Golden Compass geriatric-HIV program based at San Francisco General Hospital using an implementation science framework Reach-Effectiveness-Adoption-Implementation-Maintenance (RE-AIM).
What Are Your Research’s Implications toward Theory, Practice, or Policy?
The use of the RE-AIM framework allows for knowledge learned from our program implementation to be applied to other settings or practices.
Introduction
With expanded access to antiretroviral therapy, life expectancy for people living with HIV (PLWH) has improved, approaching that of the general population. 1 -3 As a result, the number of older adults living with HIV has steadily increased. Worldwide in 2016, 5.7 million PLWH were age 50 years or older, a number estimated to increase to at least 7.5 million older adults in 2020. 1 While the majority of older PLWH live in low- and middle-income countries, in high-income countries like the United States, the proportion of older PLWH is higher, with 50% of PLWH in the United States now age ≥50. 1,4 Although most older adults living with HIV were diagnosed at younger ages and have “aged with HIV,” new HIV diagnoses in people aged 50 years or older also occur. In the United States, people aged 50 years or older account for 17% of new HIV diagnoses. 4
Age 50 is commonly used to define “older” for PLWH in part due to studies showing that PLWH are at increased risk of age-related comorbidities like cardiovascular disease and osteoporosis and that PLWH experience geriatric conditions such as falls and frailty at relatively younger ages than the general population. 5 -9 This increased risk of other comorbid diseases stems from a combination of factors, including chronic inflammation from HIV infection, antiretroviral medication toxicities, and lifestyle factors such as alcohol and tobacco use. 10,11 Older PLWH often experience multiple comorbid conditions, or multimorbidity, which can lead to polypharmacy. 12 -14 Adding to this medical complexity, some older PLWH also face mental health conditions and psychosocial issues such as substance use, loneliness and social isolation, and stigma. 11,15 -17 The combined burden of HIV, comorbidities, and geriatric conditions in this population necessitates a shift in HIV care from a focus primarily on HIV-related outcomes toward more holistic models of care aimed at treating comorbidities and improving quality of life. Addressing geriatric conditions can be especially important as conditions such as functional and neurocognitive impairments are associated with poorer quality of life in PLWH. 18,19 This paradigm shift, dubbed “geriatric-HIV medicine,” endorses that geriatricians and HIV providers start sharing the “same language” and incorporate geriatric medicine principles when caring for this burgeoning population. 20 -22
In response to this needed shift in care, a small number of geriatric-HIV programs have emerged worldwide, mostly in high-income countries in Europe and the United States. 23 A few programs, such as in Italy and Australia, emerged from clinics originally focused on metabolic complications of HIV and are now focused on multimorbidity and frailty. 23 Other programs are based on a consultative model where a consultant or team conducts geriatric assessments focused on domains such as cognition, mental health, and physical function. 23 Examples of consultative models include a geriatrician-led weekly consultative clinic embedded in an HIV clinic (Center for Special Services clinic in New York City); an interdisciplinary review of geriatric screening results by a team comprised of a physician with geriatrics and infectious disease expertise, a pharmacist, a social worker, and a nurse practitioner (former Mmutu Clinic in New Orleans); and a separate, dedicated referral clinic consisting of an HIV consultant, nurse practitioner, pharmacist, and nutritionist (Over 50 clinic in London). 20,23 -25 Although 3 clinics (New York, New Orleans, London) have program descriptions reported in the literature, empirical data on such programs are lacking, especially program evaluation data. 25 -27 Few short-term outcomes are described, and we are unaware of data on concepts such as program acceptability, which is important for long-term programmatic success. 25 -27
The field of implementation science can help address this knowledge gap, to allow for better understanding of how geriatric-HIV programs address age-related challenges in real-world clinical settings. Broadly, implementation science can be defined as the study of the strategies used to translate research knowledge into clinical practice. 28 Implementation science research has been proposed as a solution to address gaps in HIV prevention and the HIV care continuum and could also be applied to help identify and address gaps in the care of older adults living with HIV. 29,30 Further, implementation science frameworks provide a way to organize data for dissemination of program findings to other settings. Although multiple implementation science frameworks exist, the Reach-Effectiveness-Adoption-Implementation-Maintenance (RE-AIM) framework is an established framework used in public health settings for 20 years and has been specifically proposed for HIV research. 31 -34
To expand on the current knowledge of geriatric-HIV programs, in this study, we evaluated the initial implementation of the Golden Compass Program, at the Ward 86 outpatient HIV clinic at San Francisco General Hospital, using the RE-AIM framework. The Golden Compass Program is a geriatric-HIV program designed to address key health-related challenges experienced by older PLWH and consists of consultative geriatrics and cardiology clinics located within the HIV clinic and participatory group classes for patients; the theory-based design of the program is described previously. 35 This evaluation focuses on the period from program inception in January 2017 through June 2018. Importantly, through the use of the RE-AIM framework, this article presents assessment of initial outcomes such as acceptability and satisfaction with the program among patients and providers.
Methods
Program Setting and Participants
The Ward 86 clinic is a Ryan White and public health funded clinic located on the San Francisco General Hospital campus. Ward 86 provides HIV primary care and specialty services to approximately 2600 PLWH who are publicly insured or underinsured. From 2017 to 2018, the time frame of this study, approximately 1200 patients were age 50 years or older. All PLWH age ≥50 seen at Ward 86 were eligible to participate in the Golden Compass program. Although we focused on patients at Ward 86, programming was open to the larger San Francisco community.
Program Description
The Golden Compass Program launched in January 2017 involving a team of MDs (medical director, cardiologist, geriatrician), a registered nurse (RN), a pharmacist, a program coordinator, who managed classes, and a medical assistant. We developed the program with input from patients and providers, described in detail previously.
35
Specifically, the program name, including the idea of a compass, came from focus groups with patients who reported feeling unprepared for their “Golden Years” and who reported needing help navigating the health care system.
35
Using this input, we conceptualized the Golden Compass program as a comprehensive care program for PLWH aged 50 years or older, framed around the 4 points of a compass: (1)
Program Referrals
We employed a 2-pronged strategy to introduce the Golden Compass Program to patients and medical providers. First, program components were advertised to patients through flyers and handouts posted around the clinic. Second, we introduced the program to providers and staff via a series of routine staff meetings. To participate in the program, patients could be referred by their primary care provider (most common mechanism), or by a social worker or RN on their clinical care team, to 1 or more program components. Separate referrals existed for the cardiology and geriatrics clinics, although a patient could be referred to both clinics. Participatory group classes (brain health and exercise classes) were attended on a drop-in basis and did not require provider referral. However, if a provider thought a patient might benefit from a class, they could share patient names with the program coordinator, who in turn contacted the patient with details and provided reminder calls for upcoming sessions. Additionally, participation in one programmatic component could facilitate participation in another component. For example, if a patient seen in geriatrics clinic was found to have cognitive concerns or problems with mobility and balance, they were offered participation in brain health or exercise classes. Through these systems, a patient could participate in one component (eg cardiology clinic) or multiple components (eg, geriatrics clinic and brain health classes). The extent of participation was determined by each patient and there were no time limits on participation.
Description of Initial Program Implementation
Initial program implementation focused on 3 programmatic components: (1) group classes, specifically exercise and brain health classes (Eastern and Northern Points, respectively); (2) a bimonthly consultative cardiology clinic (Northern Point); and (3) a weekly consultative geriatrics clinic (Eastern, Western, and Northern Points). All classes were on a drop-in basis and there were no limits or caps on the number of classes each patient could attend. Brain health classes were developed in conjunction with a community-based gerontologist, who led the classes. The curriculum was adapted to focus on cognitive domains relevant to HIV-associated neurocognitive disorder. 36 We conducted 3 series of brain health classes, occurring weekly for 9 weeks, between February 2017 and April 2018. Each class in the series was 2 hours long and concluded with a meal at the end. Content included strategies for addressing cognitive concerns and included sessions on mental health issues such as depression. Exercise classes, known as “Wellness Club,” focused on balance, cardiovascular, and strengthening exercises. Wellness club classes were conducted on a weekly basis over 2 time periods, between January and April 2017 and then from January 2018 on an ongoing basis. An exercise instructor with experience in leading classes for older adults in a medical setting, led the Wellness Club classes. Classes were 50 minutes in length and all exercises could be performed sitting in a chair or wheelchair.
For implementation of the cardiology clinic, a cardiologist with HIV expertise conducted cardiology consultations twice a month at Ward 86 for patients aged ≥50 years. Electrocardiography and laboratory specimens needed for cardiology clinic could be done at Ward 86, while other testing was done on the same hospital campus. For the geriatric consult clinic, a geriatrician with HIV expertise held a weekly consult clinic at Ward 86. Each initial geriatric consultation visit was scheduled for 60 minutes and included a consultation with the clinic pharmacist to review all medications. During this visit, geriatric assessments were performed and a treatment plan developed. Assessments included depression screening (Patient Health Questionnaire-9), cognitive assessment (Montreal Cognitive Assessment), functional status (Activities of Daily Living and Instrumental Activities of Daily Living), falls and gait assessment, and assessment of social supports. In this initial program implementation, only patients who were seen in geriatrics clinic underwent geriatric assessment (eg, someone who only participated in Wellness Club did not undergo geriatric screening). For both geriatrics and cardiology clinics, the need for ongoing follow-up visits was at the discretion of the consultant. Consultant notes with assessment results and treatment plans were sent to primary care providers and any medication changes discussed with providers over email or phone.
Initial implementation of screenings for dental problems and sensory impairment (Western Point) focused on older adults seen in the geriatric consultation clinic. Standard single-item screening questions assessed vision, hearing, and dental concerns and dates of last screening exams. 37,38 Referrals were made to appropriate services and information provided about discounted eyeglasses or hearing aids. Initial activities to address social isolation (Southern Point) focused on a pilot support group for older adults, along with linking patients, as appropriate, to community-based programs to address social isolation.
Evaluation Using the RE-AIM Framework
The implementation science framework RE-AIM focuses on the reach of a program to a representative proportion of the target population (often defined at the patient level), effectiveness of the program on specific outcomes, adoption of the program in a specified setting (often defined at the provider level), fidelity to the originally planned implementation, and long-term effects including how a program becomes incorporated into routine practices, or program maintenance. 31,32 -34,39 For this initial evaluation of the first 1.5 years of the program (from January 2017 to June 2018), we did not examine the maintenance dimension of RE-AIM. We used both quantitative and qualitative methods as data sources for the RE-AIM dimensions. Satisfaction surveys for the overall program and consultative clinics were administered once in the fall of 2018, at the same time and one-on-one qualitative interviews with primary care providers and patients were conducted. Qualitative interviews provided important data on barriers and facilitators of each RE-AIM dimension as well as additional effectiveness data. Table 1 summarizes the definitions and data sources utilized in our study for each RE-AIM dimension.
Definitions and Data Sources of RE-AIM Dimensions.a
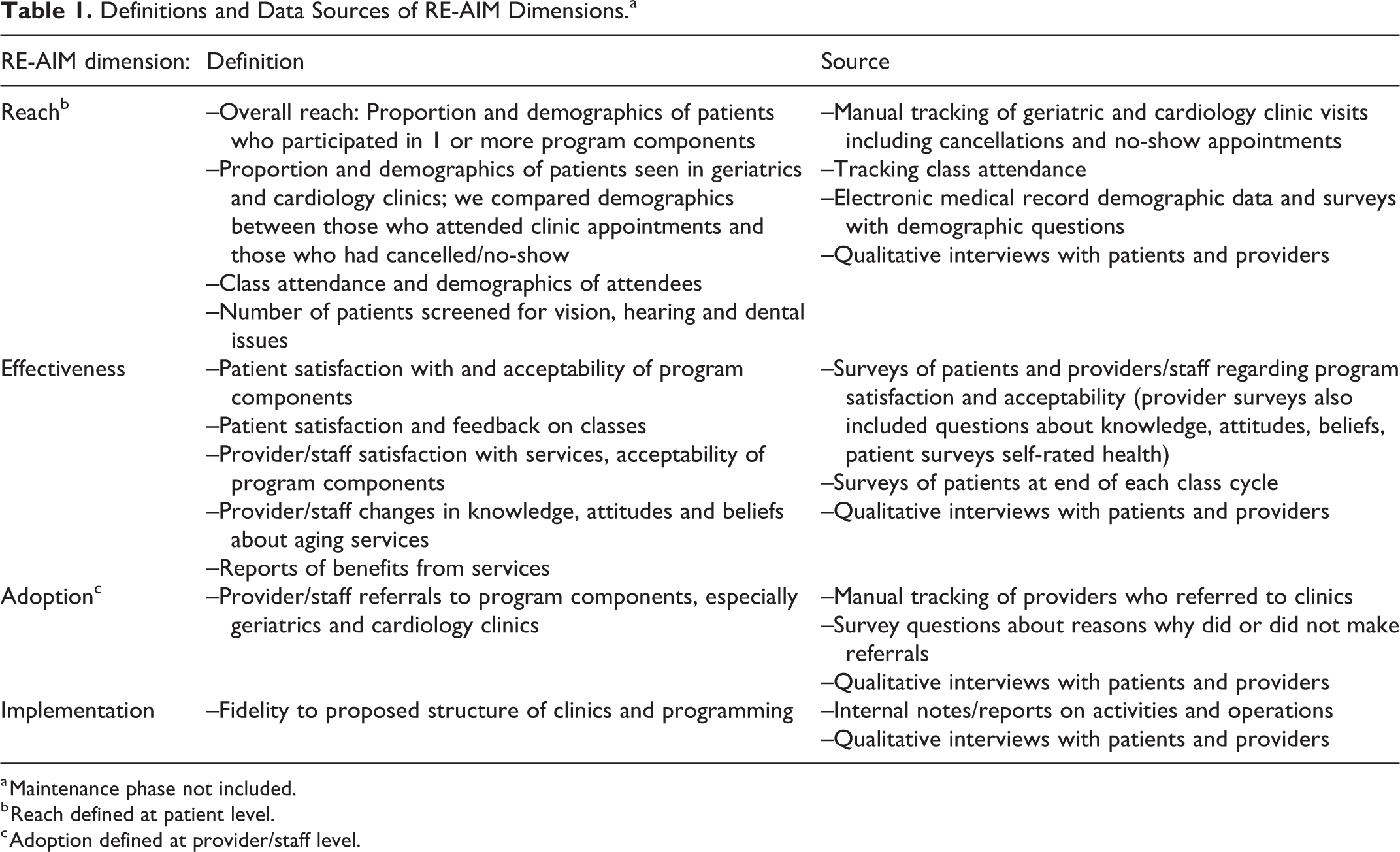
a Maintenance phase not included.
b Reach defined at patient level.
c Adoption defined at provider/staff level.
RE-AIM Dimensions
Overall reach was defined as the proportion of patients who participated in ≥1 program components compared to the total number of patients aged ≥50 years listed as patients in the clinic. The primary data source was attendance at clinic appointments and classes. We also examined participant demographics and compared the demographics of those who attended clinic appointments in the cardiology and geriatrics clinics to those who did not attend (cancelled and no-show appointments).
We examined effectiveness among patients, primary care providers, and staff in terms of the degrees of acceptability and satisfaction with the Golden Compass program. This was done through quantitative methods (satisfaction surveys done at one time point in the fall of 2018) and qualitative interviews with patients and primary care providers, for example, through benefits of the program reported during interviews. Acceptability was measured using a single item, “I would recommend x service to another person,” rated on a Likert scale from strongly agree to strongly disagree. 40 We assessed satisfaction with program components using survey items, “How satisfied were you with x,” rated on a Likert scale from very satisfied to very dissatisfied.
For patients who attended one of the consult clinics, we also assessed satisfaction with geriatrics and cardiology clinics using the 18-item Interpersonal Processes of Care scale, 41 which focuses on communication and patient-centered decision-making (items scored between 1 “never” and 5 “always”). Self-rated health before and after geriatrics and cardiology clinics was assessed retrospectively using 2 items: “How would you rate your overall health before your appointment with Dr X?” and “How would you rate your overall health after your appointment with Dr X?” The response scale for each item ranged from “excellent,” “very good,” “good,” “fair,” to “poor.” Items rating patient satisfaction with classes included satisfaction with instructors and open-ended questions about what participants liked most and least about classes, as well as any specific benefits observed or learned in classes (“Please describe any specific benefits achieved”).
Among providers and staff, we also assessed changes in knowledge, attitudes, and beliefs about aging issues and services (eg, “As a result of the Golden Compass Program, I am knowledgeable in providing care to older adults,” ranked on a Likert scale of strongly agree to strongly disagree).
Adoption was defined as provider uptake of the program, or the number of providers who made referrals to geriatrics and cardiology clinics. Provider referrals were assessed primarily through tracking scheduled appointments in each clinic. Provider satisfaction surveys also included questions about which program components they referred patients to and reasons for non-referral. Barriers and facilitators of provider adoption of the program were explored further in qualitative interviews.
We assessed fidelity to the proposed implementation of the program through internal notes, activity reports on operational changes, and through qualitative interviews of patients’ and providers’ experiences of the program.
Data Collection
Data on referrals and class attendance were collected from January 2017 through June 2018 (cardiology clinic began March 2017 and geriatrics clinic July 2016). We administered satisfaction surveys evaluating satisfaction and acceptability with the overall program and consultative clinics at a single time point in the fall of 2018 with staff, providers, and patients. We also conducted one-on-one qualitative interviews with primary care providers and patients during this time. Patient satisfaction with classes was assessed at the end of each brain health class cycle (April 2017, September 2017, and April 2018) and at the end of the second series of exercise classes (June 2018).
Patients were recruited for surveys (approximately 15 minutes in length) and interviews (45-60 minutes in length) via flyers. Flyers were posted in the clinic and were also given to patients who attended the geriatrics and cardiology clinics by a medical assistant. The flyer included a brief description of the evaluation goals and a telephone contact. Patients in turn contacted the evaluation team if they were interested in completing surveys or interviews. All providers and staff were recruited through email with links to an online survey (approximately10 minutes in length). Primary care providers who had referred at least 1 patient to the program were recruited over email to participate in qualitative interviews (20-45 minutes in length). Patient surveys were self-administered in person, either on paper or on a tablet device, with staff assistance if needed. Provider surveys were self-administered online directly through the secure UCSF REDCap survey platform. All survey data were entered and stored using REDCap electronic data capture tools hosted at UCSF. 42 Interviews were conducted by researchers experienced in conducting qualitative research in person or via videoconference using a semi-structured interview guide with open-ended questions about experiences with the program. A transcription company approved by the UCSF Committee on Human Subjects Research transcribed interview data. Patients received a $10 gift card for survey completion and a $20 gift card for qualitative interviews. Providers who completed qualitative interviews received $10 gift cards.
Data Analysis
We used descriptive statistics to summarize survey data and participant demographics. We used a framework analysis to analyze the qualitative interview data, with codes based on the RE-AIM dimensions. 43 Three coders independently reviewed the interview transcripts and met to discuss codes (JM, JT,CB). Representative quotes for each RE-AIM dimension were selected for this study.
Ethical Approval and Informed Consent
The study was conducted in accordance with the World Medical Association Declaration of Helsinki. All study procedures and activities were reviewed by the UCSF Committee for Human Subjects Research (study # 15-17859) and determined to be a project that includes program evaluations, quality improvement activities, or other activities which did not require further institutional review board oversight according to US federal regulations. Even with the exemption, we still followed principles of informed consent including emphasizing the voluntary nature of participation in the evaluation process.
Results
Results are reported in the context of each RE-AIM dimension. During the evaluation period of January 2017 to June 2018, a total of 39 providers and 28 staff worked at Ward 86, and 198 patients participated in the Golden Compass program. Sixty-three percent (n = 42) of staff and providers and 20% (n = 39) of patient participants completed satisfaction surveys. Ten patients and 9 primary care providers completed qualitative interviews.
Reach
In the first year-and-a-half since formal program launch, 198 individuals participated in 1 or more components of the Golden Compass program. Specifically, 119 were seen in geriatrics clinic, 48 in cardiology clinic, 40 attended brain health classes, and 32 attended exercise classes. Moreover, 30 (15%) participated in ≥2 components of the program. The mean age was 62 years (range 48-81); the majority were male (89%); 17% were Latino; 14 participants were from outside Ward 86. Other participant demographics are given in Table 2. Since 1200 adults aged 50 years or older are listed as patients of Ward 86, the estimated overall reach was approximately 17%.
Demographics of Golden Compass Program Participants (n = 198).

In geriatrics clinic, 119 patients were seen for a total of 182 visits. An additional 34 patients were referred to clinic but did not attend. Compared to those who attended, there were no statistically significant differences by demographic characteristics including race and ethnicity, although it was noted that those who did not attend were relatively younger (59 versus 64 years, P = .07) and more likely to identify as female (P = .08). In cardiology clinic, 48 patients were seen for a total of 98 visits. In cardiology clinic, an additional 17 referred patients did not attend appointments. Compared to those who attended, patients who did not were more likely to identify as female (23% versus 6%, P = .05); no differences were seen by race, ethnicity, or age.
Attendance in Golden Compass classes increased over time. Brain health class attendance grew from a regular group of 4 participants to a group of 10. Similarly, attendance increased over time in the exercise classes with an initial group of 8 participants attending on average 2 weeks of classes, to a group of 30 participants attending on average 5 weeks of classes. Notably, 7 participants attended ≥10 consecutive weeks of classes. For the Western point (Dental, Hearing, Vision), among geriatric clinic patients, 42 (34%) had difficulty seeing, 55 (45%) had difficulty hearing, and 45 (36%) noted dentition problems. Attendance in the support group (Southern Point) at Ward 86 was low, necessitating outside referrals.
In qualitative interviews, providers noted that convincing patients to participate in an aging-focused program was sometimes a barrier to reach. Many providers noted that discussing the program with younger patients (such as those in their early 50s) could be challenging. One provider noted that although cognitive assessments were valued (reflecting provider level effectiveness), cognitive impairment carries its own stigma, which could also be a barrier to patient reach. Table 3 includes example quotes related to the reach of the Golden Compass program.
Example Quotes for Each Re-AIM Dimension from Qualitative Interviews with Patients and Providers.

Patient Effectiveness
Thirty-nine (20%) program participants completed satisfaction surveys. Overall satisfaction and acceptability with programmatic components were high (>90%; Table 4). Interpersonal processes of care scores also reflected high satisfaction with clinics (Table 4). Although self-rated health was assessed by retrospective report, patients reported higher self-rated health (more “excellent”, “very good” responses) after being seen in geriatrics clinic (P = 0.015; Table 4). Twenty-three participants completed class surveys about brain health classes and 9 completed surveys about Wellness Club. Across all 3 brain health class cycles, in response to the prompt “What did you like most about the class?,” the most common response was interactions with others. In a prompt about benefits gained from Wellness Club, participants reported improvements in balance and posture, with one-third noting improvements in mental health (“feel happier,” “more motivated,” “emotional health has improved”) and one-third noting connection with others.
Patient Satisfaction with and Acceptability of Golden Compass Program Components.

a N = 28 for geriatrics clinic, 8 for cardiology clinic, 16 for brain health, 17 for Wellness Club.
b Acceptability measured by “How strongly do you agree, “I would recommend the x to someone else?”.
c Asked at one time point, retrospectively, P values using Wilcoxon signed-rank test.
d Asked for both cardiology and geriatrics clinics, reported as average scores from 1 to 5, with 1 being a low score or “never” and 5 being a high score or “always.”
In qualitative interviews, patients noted benefits of attending classes, including social aspects and interactions, as well as specific benefits such as learning how to “feel calm” in brain health classes. Patients appreciated meeting with the pharmacist to review medications during geriatrics clinic and appreciated a “more broad, wider” or holistic approach to health in geriatrics clinic including addressing mobility problems, which was noted as an issue for many older adults. Table 3 includes example patient quotes related to the effectiveness of the Golden Compass program.
Provider and Staff Effectiveness
Overall, 42 (63%) of staff and providers completed satisfaction surveys (16 staff and 26 providers, with 18 providers having referred at least 1 patient to geriatrics clinic and 14 providers having referred at least 1 patient to cardiology clinic). All disciplines were represented among survey respondents, with MD/NP providers (n = 22), nursing (n = 4), medical assistants (n = 8), and other staff (n = 8). Table 5 summarizes staff and provider satisfaction survey data. Satisfaction with the Golden Compass program was high, with 38 (90%) reporting very satisfied or satisfied with the program overall and with cardiology and geriatric clinics. A majority (90%) of staff and providers agreed or strongly agreed that the program improved the health of older adults at Ward 86. In open-ended survey responses, comments included phrases such as “pivotal program,” or “welcomed addition.” Areas for improvement in comments included appointment wait times, how to best communicate with specialists and refer to appointments, and advertising more effectively.
Provider and Staff Satisfaction with and Acceptability of Golden Compass Program Components.

a Acceptability measured by “How strongly do you agree, “I would recommend the x to someone else?”
b n = 18 for responses to geriatric consults, n = 14 for responses to cardiology consults.
c No one answered dissatisfied or very dissatisfied, but 29% answered “unsure” or that “patients referred did not participate.”
With regard to knowledge, attitudes, and beliefs about aging services among staff and providers, 30 (72%) strongly agreed or agreed that their comfort in providing care for older adults had increased since program inception and 26 (62%) strongly agreed/agreed that they felt knowledgeable about caring for older adults since program inception. Similar responses were obtained regarding changes in confidence in ability to care for older adults, with 25 (59%) noting strongly agree/agree. Overall, 11 (76%) providers who referred to cardiology clinic felt the referral increased their knowledge of cardiology topics and 17 (94%) providers who referred to geriatrics clinic felt their knowledge of geriatric assessment and management increased.
Among the 9 primary care providers who completed qualitative interviews, combined they referred 70 patients to cardiology and geriatrics clinics, with an average of 2 referrals to cardiology and 5 referrals to geriatrics. Complementary to survey data, reviewing consultants’ notes and applying knowledge gained to other patients was noted during interviews (Table 3). Improvement in patients’ lives, such as addressing cognition and mobility issues in geriatrics clinic, was another notable theme. Addressing polypharmacy and pharmacist support was viewed as a benefit to patients and helpful to providers. Providers also observed that patients benefitted from class participation (Table 3). A desire for increased mental health services for older adults was noted.
Adoption
A total of 39 providers and 28 staff were working at Ward 86 in 2017 to 2018. Through tracking clinic appointments, 33 (85%) providers had referred at least 1 patient to the geriatrics clinic, with a range of 1 to 16 patients referred. Twenty-three (59%) had referred to the cardiology clinic, with a range of 1 to 14 patients referred. The most common reasons for referral to geriatrics clinic included general evaluation (n = 48, 40%), cognition (37, 31%), and falls (14, 11%). The most common referral reasons to cardiology clinic included coronary artery disease (20, 42%), congestive heart failure (7, 15%), arrhythmias (including atrial fibrillation, n = 5, 10%), and pulmonary hypertension (5, 10%).
Among the staff and providers who completed surveys (n = 42, 63% of total staff and providers), 12 (80%) staff and 23 (90%) providers reported recommending 1 or more program components to patients. The majority of respondents had referred to geriatrics clinic (n = 27, 77%), brain health classes (n = 25, 72%) followed by exercise classes (n = 21, 60%), and cardiology clinic (n = 17, 17, 49%). Staff (n = 3) who did not discuss the program with patients cited time constraints (n = 1) and role responsibilities as reasons (eg, more the role of the patient’s primary care provider, n = 2). Two providers who had not referred to any program components indicated not knowing how to make a referral, being unaware of program components or not understanding what a geriatric consult provides.
In interviews with primary care providers, confusion over referral workflows to geriatrics and cardiology clinics was noted as a minor barrier to adoption. Value and perceived benefits to patients seen from prior referrals facilitated further referrals and overall adoption (Table 3).
Implementation
Overall, the program was implemented as originally planned. A few changes did occur including refocusing the Southern Point (social support) to our community partners with active support groups. Interviews supported fidelity to proposed implementation, including the flow of initial geriatrics clinic visits with the pharmacist and geriatrician (Table 3). Both providers and patients identified colocation of geriatrics and cardiology clinics at Ward 86 as helpful and important. Both groups noted lack of Spanish-language programming as a challenge. Providers noted a need for clarity regarding the role of the Golden Compass team as either providing consultation or ongoing follow-up support, with some desiring more comanagement options (eg, ongoing geriatric care).
Discussion
As the field of “geriatric-HIV medicine” evolves, improved knowledge of existing geriatric-HIV programs is needed. In this study, we evaluate the initial implementation of the Golden Compass geriatric-HIV program in San Francisco, using the RE-AIM framework. The Golden Compass program offers comprehensive services with a focus not just on consultative clinics in geriatrics and cardiology but also on classes and fostering social connections. In the first year and a half, we reached approximately 17% of older adults at the Ward 86 HIV clinic with overall fidelity to the original program design. Provider adoption of services was high with 60% and 80% of providers referring at least 1 patient to cardiology and geriatrics clinic, respectively. Overall, patients and providers found the program to be highly acceptable and were satisfied with services. Our study helps address the knowledge gap about geriatric-HIV programs by providing evaluation data including data on short-term outcomes and acceptability of services.
Use of the implementation science framework RE-AIM is a strength of this evaluation, as it allowed us to consider and analyze relevant public health dimensions such as reach and effectiveness. 29,32 Additionally, the qualitative and quantitative methods used to define the RE-AIM dimensions were complementary. For example, with regard to reach, during provider interviews, stigma against attending an “aging” program was perceived as a barrier to participation for some patients, especially those in their 50s. While we had heard that sentiment expressed by patients during program development, and intentionally omitted the word “HIV” or “geriatrics” or “aging,” it can be challenging to frame the program to patients, especially to the geriatrics clinic, without using the term “aging.” Indeed, those who did not attend geriatric clinic appointments (canceled or no-show appointments) were relatively younger compared to those who did attend (age 59 versus 64 years). Missed appointments also helps explain the high adoption rate of the Golden Compass Program through provider referrals yet lower overall reach. Provider suggestions on how to address this concern included framing the program as “staying healthy as you get older” or “living longer with HIV,” both of which we plan to incorporate in the future.
Regarding effectiveness, we focused on early implementation outcomes, including satisfaction and acceptability of services. Overall, we found a high degree of satisfaction with all program components, often ≥90% among both patients and providers. Patients retrospectively reported improvements in self-rated health after attending geriatrics clinic appointments, a measure which has been used as a single-item measure of quality of life in HIV clinics. 44 In interviews, providers and patients valued services through the program, especially addressing medications and mobility problems, although the need for greater mental health services was noted. Colocation of services was also valued. The preliminary finding of improved self-rated health and the value of geriatric assessments supports the literature on geriatric assessment being associated with quality of life in older PLWH. 18,19 The value of colocation of services supports a study of Ryan White HIV/AIDS program funded clinics, which also reported the importance of colocation of services. 45
A greater range of responses was seen in terms of knowledge, attitudes, and beliefs among providers and staff; 70% noted increases in comfort, confidence, and knowledge since program inception. Of note, initial program activities did not include specific educational outreach to staff and providers, which may explain the result. Overall implementation of the program proceeded as intended, except for the unexpected low attendance rate at the social support group, necessitating referrals to established community-based groups. Importantly, patients found support and connection through Wellness Club (exercise classes) and brain health classes offered, so may not have required an additional social support group.
Although it is difficult to make direct comparisons, for context on our RE-AIM findings, in terms of reach, the geriatric-HIV program in New Orleans (Mmutu Clinic) saw 60 of 160 eligible patients age ≥60 in 1 year; the Over 50 clinic in London saw 150 patients over 2 years, and the Center for Special Studies program in New York City saw 76 patients over 4 years (2800 patients all ages). 24 -26 The Center for Special Services program in New York reported that 7 of 10 providers found geriatric consultations very or extremely useful, which similar to our results suggest that providers find services valuable. 26
Another strength of using the RE-AIM framework in our evaluation is it provides a structure to organize key findings and how these findings might be applied or adapted to other settings. 29 For example, to expand the reach of geriatric-HIV programs, it is critical to not only frame services to avoid stigma from HIV but also agism. Through qualitative interviews, we learned more about the challenges of framing or advertising aging services to patients, despite our original best intentions of developing the program name, Golden Compass, to avoid “aging” or “geriatrics.” Another key finding relates to the preliminary effectiveness data, as patients reported developing new social connections through the program’s classes. This is important as more literature emerges about the hazards of isolation and loneliness on the overall health for older adults. 15,46 -48 We learned that fostering new social connections can occur through different types of programming and not just formal support groups. Also relevant to effectiveness, colocated services were valued by both patients and providers. We acknowledge that access to a colocated geriatrician may be difficult in some settings, given the limited numbers of geriatricians in the United States. Training HIV staff and interested providers in geriatric principles to conduct on-site geriatric assessments or using telemedicine consults could be adaptations, which still offer the spirit of colocated services. Furthermore, we found that the program was implemented largely as planned, which allows our program description to be reviewed by others and adapted to local resources. This is especially relevant as resources may vary between urban settings like ours and rural areas in the United States, and especially relevant to differences in resources between high- and low- and middle-income countries.
Limitations do exist in our study, especially with our definition of reach. The denominator we used to examine reach is a current estimate of patients aged 50 years or older assigned to Ward 86, many of whom may not be actively engaged in services or attending clinic during the study time frame (2017-2018). Additionally, it is unclear that everyone age 50 years or older needs or would benefit from the Golden Compass services. Determining who would benefit most from aging services, especially geriatric consultative services, remains a gap in the literature. If anything, these limitations mean our current reach may be underestimated. In terms of effectiveness, we focused on satisfaction and acceptability in survey data and less on patient-reported outcomes, which is a future focus, including geriatric assessment results and prospective assessment of measures such as self-rated health. Our current retrospective measure of self-rated health limits interpretation of this result. However, survey data were enhanced by data from the qualitative interviews. We did not specifically evaluate the “maintenance” phase of RE-AIM, but funding for the program is ongoing and we are planning to use this study to further refine processes and improve services.
Our findings have important implications for further research and policy directions in “geriatric-HIV medicine.” Our effectiveness findings, such as satisfaction with and acceptability of services, not only fill a knowledge gap regarding geriatric-HIV programs but also provide early evidence for policy makers to support development and funding of these programs. Use of implementation science frameworks such as RE-AIM for program evaluation will be an important tool to advance the field, to allow for better comparisons across programs. The addition of qualitative methodology, as used in our study, is also an important tool to improve internal program processes and provide additional program outcome data, which in turn can support ongoing funding and program maintenance. For policy makers in the United States, where our program is based, 2 of the largest HIV service providers, the Veterans Health Administration (VA) and the Ryan White HIV/AIDS Program, may be ideal settings to implement a program like the Golden Compass program. Both settings could implement colocated services and programming such as classes. The VA has a strong tradition of geriatric services such as the Geriatric Research Education and Clinical Centers and the Ryan White program already emphasizes comprehensive colocated and wrap-around services which could be extended to geriatric and other subspecialist consultants. 49 -51
A critical need exists for the development and improved understanding of geriatric-HIV programs for older PLWH, given the medical and psychosocial challenges facing this population. The Golden Compass program based at San Francisco General Hospital is an innovative program designed to address key issues facing older HIV-positive adults. This initial evaluation of the program holds key lessons for replication in other settings to serve the increasing number of older adults living with HIV.
Footnotes
Authors’ Note
All study procedures and activities were reviewed by the UCSF Committee for Human Subjects Research (study # 15-17859) and determined to be a project that includes program evaluations, quality improvement activities, or other activities which did not require further IRB oversight according to the federal regulations summarized in 45 CFR 46.102(d).
Acknowledgements
We thank our community instructors Hope Levy and Cynthia Simon, who led our Brain Health Classes and Wellness Club.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institutes of Health/National Institute on Aging (R03AG05634); Tideswell at UCSF; and the Golden Compass program has received support from AIDS Walk San Francisco, the San Francisco Department of Public Health, and Design Industries Foundation Fighting AIDS (DIFFA).