
Abstract
The HIV-infected population in the United States is aging. A retrospective study of 132 patients (26 women, 106 men) ≥59 years of age was undertaken to evaluate the effect of race and sex on selected outcomes. With the exception of women being more likely to have diagnosis of depression compared with men, sex had little influence on risk for other conditions among elderly patients with HIV. In contrast, African American race was significantly associated with the risk for several selected disorders and outcomes. These results can assist in future prevention efforts among senior individuals with HIV infection.
Keywords
Introduction
By 2015, it is estimated that over 50% of persons with HIV will be at least 50 years old. 1,2 This phenomenon is likely in part due to the success of potent antiretroviral therapy (ART) since patients with HIV are now living longer with their disease. 1,3 Apart from reviews describing this epidemiologic change and management challenges in the elderly, 4–8 data are limited from actual studies describing the geriatric population with HIV. 4,9 This is the first study to evaluate race and sex associations with clinical characteristics and to study predictors for specific outcomes associated with aging among elderly patients with HIV.
Study Design
A cohort of 132 patients was retrospectively assessed within a follow-up period of 4.5 years (range 2 months to 9 years). Patient selection criteria comprised age (≥59 years by December 2008), HIV-positive status confirmed by laboratory testing, and having had at least 2 visits documented through electronic records during the observed period. Information was abstracted from patient’s electronic records in 2009 and covered clinical events through December 2008.
Most medical and all mental health disorders including depression and insomnia were clinician assessments in the electronic records. Diagnoses that were objectively diagnosed included hypertension (ever having a documented blood pressure of >140/90 mm Hg or on medication), diabetes mellitus (ever on medication), dyslipidemia (ever total cholesterol >200 mg/dL, low-density lipoprotein >130 mg/dL or triglycerides >150 mg/dL, high-density lipoprotein <35 mg/dL or on medication), and liver disease (defined as having positive hepatitis C antibody or hepatitis B surface antigen serology). All concurrent diagnosis variables were evaluated as categorical outcomes at baseline (prevalent conditions) or during the observation period (incident or newly diagnosed prevalent conditions). Selected medications and substance use were recorded as categorical variables at baseline and during observation period (ever/never initiated). Continuous variables were summarized using mean, median, or categorized as binary observations using clinically relative cut points. Square root transformation was used to reach normality. Study outcomes were newly developed mobility problems and hospitalizations in the study period.
Data were entered in an access database and was analyzed using SAS 9.2 software (Cary, North Carolina). 10 Chi-square test was used to compare proportions and 2 sample t-test for mean comparison with a level of .05. Bonferroni correction of P value was used to account for multiple comparisons (α/n). 11 Significant sex and race differences were explored after adjusting for potential confounders (age and clinical outcomes) using multivariate logistic regression. Full logistic models were built and variables were deleted from the model in a step-backward fashion aiming the parsimonious model. Models were tested for goodness-of-fitness and compared hierarchically by using the likelihood ratio test. Effect modification was explored for sex and race.
This study was done in accordance with the Louisiana State University research standards and the approval of the Institutional Review Board.
Results
A total of 132 patients (28 women and 104 men) were included in the study. Median age for the study cohort was 63 years (women 62 years and men 63 years) and 62.6% were African American (women 89.3%, men 55.3%). Non-African Americans were universally Caucasian. The subpopulation of older patients was not statistically different compared to the HOP clinic population <59 years of age in regard to sex and racial proportions. In all, 31% of the men had a risk category of male to male (MSM) sex and 5 of the men with an MSM risk were injection drug users (IDUs). Thirteen patients (9 women and 4 men) were categorized as having a heterosexual risk. Two men, but no women, were at risk because of a blood transfusion or transplant. Forty-two patients (11
Substance use other than IDU was common. Proportions of the population using legal and illicit substances at baseline or during the study period were as follows: cigarettes (49.2%), alcohol binges (18.9%), crack cocaine (8.3%), and marijuana (11.4%). Fifteen patients had a history of IDU (3 women and 12 men). No patient was identified as using crystal metamphetamines. The total number of older patients who used any type of illicit substances during the study period was 25 (19.7%). Sex and race were not associated with the use of any substance.
The study population baseline immunity was relatively well preserved as reflected by the relatively high mean CD4 counts, but African Americans had a significantly lower mean count compared to non-African Americans (P < .005). The proportion of patients having an HIV RNA level <400 copies at baseline was 28.8%. This study did not evaluate virologic response to ARV medications, but all patients ever on ARV medications during the study period had a nondetectable HIV RNA level (<400 copies) at least once. Women had a lower baseline mean hemoglobin compared to men, but levels were consistent with normal ranges. 12 African Americans had a significantly lower mean baseline hemoglobin and serum albumin compared to non-African Americans (P < .05), which may have reflected a more advanced HIV disease status. Renal function was similar between men and women, but African Americans had both a lower baseline creatinine clearance and a higher prevalence of proteinuria compared to non-African Americans. However, these differences did not reach statistical significance. Only 4 patients in our study population had chronic renal failure.
The mean serum aspartate amino transferase (AST) was slightly elevated for the entire cohort and was modestly higher among women and African Americans compared to men and non-African Americans, respectively. Hepatitis C infection was the only variable significantly associated with increased AST levels (P < .001, Table 1).
Selected Baseline a Laboratory Characteristics by Sex and Race (n = 132)

Abbreviations: AA, African American; AST, aspartate aminotransferase.
a Group mean.
b Mean difference P = <.05.
Frequent medical or mental health conditions present either at baseline or diagnosed during the study period are shown in Table 2. Of the 43 patients with liver disease, 37 had chronic hepatitis C infection and 5 were hepatitis B surface antigen positive. Women were more depressed compared to men, but there were no significant associations between sex and any other condition. African Americans were more likely to be diagnosed with mild liver disease, hepatitis C infection, and diabetes and less likely to be diagnosed with depression and other mental health conditions compared to non-African Americans. However, after adjusting for age, sex, and baseline body mass index (BMI), race was not associated with diabetes.
Selected Medical and Mental Health Disorders Diagnosed at Baseline and during the Study Period by Sex and Race
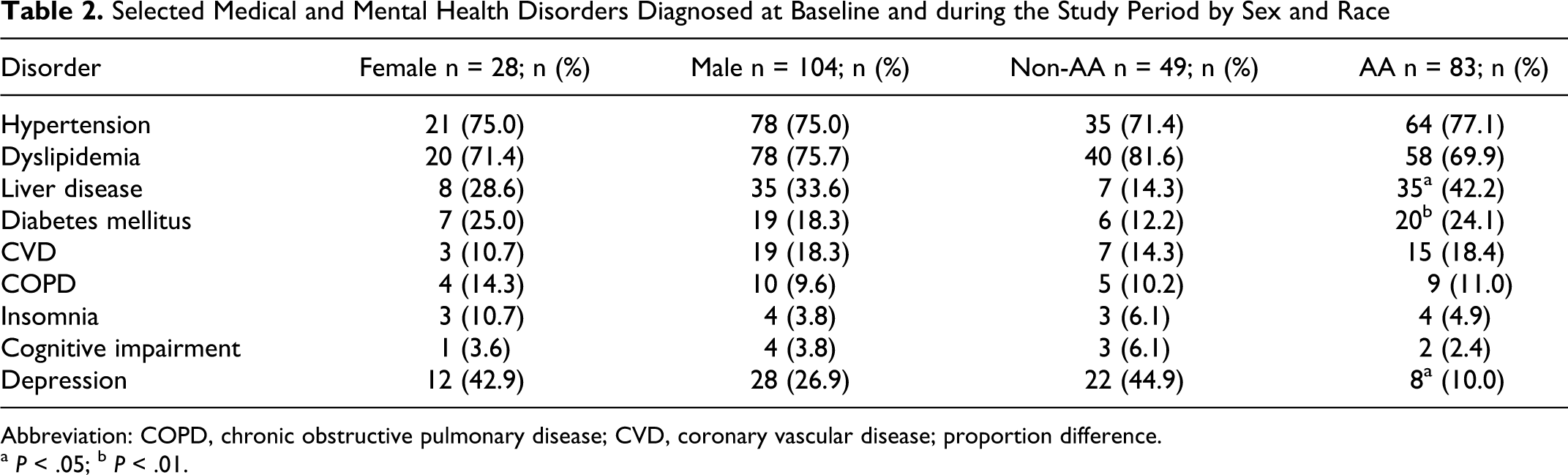
Abbreviation: COPD, chronic obstructive pulmonary disease; CVD, coronary vascular disease; proportion difference.
a P < .05
b P < .01.
Both sex and race were independently associated with depression. Female sex (odds ratio [OR] = 3.7, P = .012) and non-African American race (OR = 4.8, P = .001) had a significant association with depression, and independent of their age and sex, African Americans (OR = 2.3, P < .001) and IDUs (OR = 1.4, P < .04) were most likely to be diagnosed with hepatitis C.
Of the study cohort, 94% was ever on ARV medications. In addition to medications for underlying medical conditions, patients were often on pain medications during the study period (22% ever opiates, 20% ever gabapentin, and 16% nonsteroidal anti-inflammatory agents). Sex and race were not associated with either opiate or pain medication use.
Seventeen patients suffered mobility impairment including the use an aide for walking (3.0%), the use a wheelchair (2.3%), or ever having a fall (7.6%) during the study period. Results showed that age, sex, and race were not associated with all combined categories of mobility impairment outcomes described above. However, having a diagnosis of diabetes showed a trend toward significance association with the presence of mobility impairment (OR= 3.2, P = .06). A total of 48 persons were hospitalized during the study period. Multivariate analysis showed that African American race (OR = 10.4, P = .0001), cardiovascular disease (OR = 3.6, P = .003), and late HIV diagnosis (>59 years of age; OR: 4.1, P = .02) were independently associated with hospitalization. Other rare outcomes not statistically analyzed included 4 cases that were placed in a nursing home and 1 death.
Discussion
Medical and mental health conditions increase with age in the geriatric population. Not surprisingly, 92% of the study population had at least 1 comorbidity in addition to their HIV infection. The most common concurrent medical disorders described in previous studies in older HIV-infected patients are dyslipidemia, hypertension, diabetes, and cardiovascular disease. 13–16 In the current study, approximately 75% of the population had at least one of these diagnoses with hypertension and dyslipidemia as the most prevalent.
Unlike in the Spanish cohort studied by Mothe, 13 in our study, chronic renal failure was an uncommon condition. Such difference could be explained by that Mothe’s study cohort was much older than ours (mean age >70 years vs 63 years). In our study, African Americans had the lowest creatinine clearance and the highest prevalence of proteinuria; this could reflect a more advanced HIV disease status or a higher vulnerability to renal disease when compared to non-African Americans. 17,18 Unexpectedly, African American race was independently associated with the presence of mild liver disease and hepatitis C infection which contradicts with what has been previously described in the general population. 19,20
Several studies have reported a higher prevalence of cognitive dysfunction and mental health problems in HIV-infected patients compared to those uninfected. 21–24 Depression was particularly frequent in our study population with over a third having this diagnosis documented. As in the general population, non-African American or Caucasian women appeared to be at an increased risk for this condition. 25
In addition to mental health problems, substance use is disturbingly frequent among older HIV-infected patients. In a review of 50 HIV-infected patients, Carballo-Alvarez 24 found that the use of illicit substances was at a rate of 50% more than in HIV-negative patients. In another study of 1803 veteran patients (1047 HIV-positive), Justice 26 confirmed a higher prevalence of alcohol and or drug abuse and dependence among elderly HIV-infected patient compared to their non-HIV-infected counterparts. Nearly 20% of our cohort used illicit substances, with the drugs of choice being cocaine and marihuana. In addition to illicit substance use, over 20% of our cohort was on controlled opiate medications for pain control. Illicit and legal prescription drug use was equivalent in all sex and racial groups.
As the HIV-infected population in the United States ages, clinicians need to plan for care of an increasing number of elderly patients with several comorbidities. A recent review conducted in our clinic found almost thirty (30%) percent of HIV-infected patients >60 years presented with a geriatric dysfunction after initial rapid screening. 27 This study confirms the high frequency of several conditions including hypertension, dyslipidemia, liver disease, diabetes, cardiovascular disease, mental health problems, chronic pain, and substance use among seniors with HIV. Our study is the first to explore possible sex and race differences in vulnerability for selected conditions and outcomes in an elderly HIV-infected population. Although sex had little influence on the risk for most concurrent disorders or outcomes, African Americans appeared to be significantly more at risk for several conditions in this study. These results may be in part due to the more advanced disease status among elderly African Americans in our clinic as demonstrated by their lower baseline CD4 count, hemoglobin, and serum albumin compared to non-African Americans. Future prospective studies are warranted to confirm our results. Regardless, the findings from our study can help determine the need for sex- or race-targeted preventive strategies to avoid future morbidity in the senior population with HIV infection.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.