
Abstract
Objectives:
To assess measurement properties of the HIV Disability Questionnaire (HDQ) among adults with HIV in the United States.
Methods:
We administered the HDQ, World Health Organization Disability Assessment Schedule II (WHODAS 2.0), and a demographic questionnaire. For internal consistency reliability, we calculated Cronbach α and Kuder-Richardson-20 (KR-20) statistics for disability and episodic scores, respectively (≥0.80 acceptable). For test–retest reliability, we calculated intraclass correlation coefficients (>0.8 acceptable). For construct validity, we tested 15 a priori hypotheses assessing correlations between HDQ and WHODAS 2.0 scores.
Results:
Of the 128 participants, the majority were males (68%), median age 51 years, taking antiretroviral therapy (96%). Cronbach α ranged from 0.88 (social inclusion) to 0.93 (uncertainty). The KR-20 ranged from 0.86 (cognitive) to 0.96 (uncertainty). Intraclass correlation coefficients ranged from 0.88 (physical, cognitive, social inclusion) to 0.92 (mental–emotional). Of the 15 hypotheses, 13 (87%) were confirmed.
Conclusions:
The HDQ demonstrates internal consistency reliability, test–retest reliability, and construct validity when administered to a sample of adults with HIV in the United States.
What Do We Already Know About This Topic?
The HIV Disability Questionnaire (HDQ) is the first known HIV-specific patient-reported outcome measure (PROM) developed and validated for use in Canada to measure the presence, severity, and episodic nature of disability experienced by adults living with HIV.
How Does Your Research Contribute to the Field?
Results from this study build on previous evidence of HDQ properties among adults living with HIV in Canada, Ireland, and the United Kingdom, to demonstrate that the HDQ possesses internal consistency reliability, test–retest reliability, and construct validity with a sample of adults living with HIV in the United States, suggesting the HDQ may be well positioned for use as a PROM to universally measure disability internationally.
What Are Your Research’s Implications toward Theory, Practice, or Policy?
Clinicians, researchers, community-based organizations, and people living with HIV may use the HDQ to document the nature and burden of disability experienced with HIV, facilitate communication among health providers and patients, facilitate goal setting, and identify the need for referrals to health services, while ongoing universal measurement of disability may contribute to tracking of episodic disability trends to more broadly inform programming and policy to promote health with HIV.
Introduction
At the end of 2015, an estimated 1 122 900 people were living with HIV in the United States. 1 In countries with access to combined antiretroviral therapy, such as the United States, more individuals are living longer and experiencing a combination of health-related challenges associated with HIV, multimorbidity, and aging, known as disability. 2 –6 The Episodic Disability Framework was derived through qualitative inquiry with adults living with HIV in Canada who conceptualized disability as multidimensional and episodic in nature and defined disability as physical, cognitive, mental, and emotional symptoms and impairments, difficulties with day-to-day activities, challenges to social inclusion, and uncertainty or worrying about future health that can fluctuate daily or over the course of living with HIV. 7 Disability has been documented among people living with HIV in the United States to include functional impairments 8 and reduced aerobic capacity, 8,9 self-reported cognitive impairments 10 and HIV-associated neurocognitive disorder, 11,12 and mental and emotional impairments such as depression 13 and anxiety, 14 which can contribute to challenges of social isolation and loneliness. 15,16 Hence, as more individuals age with HIV, it is critical to establish tools with which to measure the presence, burden, and episodic nature of the multidimensional nature of disability experienced by adults living with HIV in countries where they may experience similar forms of disability.
Measuring disability among people living with HIV is important for determining the burden of disease and for evaluating the effectiveness of treatment interventions. Using patient-reported outcome measures (PROMs) in HIV clinical practice can enhance person–provider communication, identify an individual’s needs, facilitate goal setting, and inform areas of resource allocation for future programming, thus facilitating person-centered care for people living with HIV. 17 Although a number of health status instruments exist, results of a content analysis determined that none captured the breadth and depth of disability experienced by adults living with HIV as articulated in the Episodic Disability Framework. 18 Many instruments were developed prior to the introduction of combined antiretroviral therapy and were deficient for items of social inclusion and uncertainty, which were deemed important to people living with HIV, 18 highlighting the need to develop an HIV-specific disability questionnaire.
The HIV Disability Questionnaire (HDQ) is a self-administered PROM, developed in Canada, to measure the presence, severity, and episodic nature of disability experienced by adults living with HIV. 19 The HDQ was derived from categories in the Episodic Disability Framework using community-engaged approaches, involving adults living with HIV, representatives from community-based organizations, and policy stakeholders who provided guidance on content, item phrasing, order, response options, and questionnaire instructions to enhance feasibility and relevance of the HDQ. 20 The HDQ was subsequently assessed for sensibility 21 to determine whether the HDQ was meaningful to adults living with HIV. Members of our team conducted a series of interviews with adults living with HIV to seek feedback on whether the HDQ adequately described their disability experiences, the adequacy of items and response options, readability, clarity of instructions, and format. 22 Results led to further refinement of the questionnaire.
The HDQ since has been assessed for validity and reliability for use with adults living with HIV in Canada, Ireland, and the United Kingdom. 23 –25 However, measurement properties are specific to the population and setting in which the properties of a questionnaire are established and the context in which a questionnaire is used. 26 Hence, the HDQ may not be applicable to people with HIV living in other countries with different sociocultural, health system, economic, and political contexts. For instance, in the United States, an increasing number of new cases of HIV were found in poor-resource regions with inadequate availability to health care. People living with HIV who have employer-sponsored health insurance or purchase a plan through the Affordable Care Act 27 are still required to issue co-payments. Often, these can continue to increase in amount, which can be cost prohibitive. Various limitations regarding eligibility for Medicaid is determined by a state-by-state variability. This can result in inconsistency in providing access to the most important source of HIV interventions. Although state-by-state programs may help to address these inequities, people with limited income are often left without health care. 28 Furthermore, retention in HIV care among people living with HIV was found to be lower in the United States compared to other developed countries such as Canada, 29 –31 further contributing to the distinct contextual factors experienced among people living with HIV across different environments. Hence, the extent to which the HDQ can accurately and consistently measure disability among people living with HIV in different contexts, such as the United States, is unknown. Our aim was to assess the measurement properties of the HDQ for its ability to describe disability experienced among adults living with HIV in the United States.
Methods
We conducted a cross-sectional measurement study to assess internal consistency reliability, test–retest reliability, and construct validity of the HDQ with a sample of community-dwelling adults living with HIV in the United States. We recruited adults living with HIV from Garden State Infectious Disease Associates in Voorhees, New Jersey.
We administered the HDQ, the World Health Organization Disability Assessment Schedule II (WHODAS 2.0), and a demographic questionnaire. The HDQ is a 69-item patient-reported questionnaire comprised of 6 domains: (1) physical health symptoms and impairments, (2) cognitive symptoms and impairments, (3) mental and emotional health symptoms and impairments, (4) uncertainty and worrying about future health, (5) difficulty carrying out day-to-day activities, and (6) challenges to social inclusion. 19 Participants are asked to rate the presence and level of severity of each health challenge on a given day ranging from 0 (not at all) to 4 (extreme). For each health-related challenge, participants are also asked to indicate whether that challenge fluctuated in the past week, meaning the challenge got worse or better or both (yes/no). The HDQ also includes one health classification item whereby participants are asked whether they completed the HDQ on what they would consider a “good day” or “bad day” living with HIV (yes/no). The HDQ scores range from 0 to 100, with higher scores indicating a greater presence, severity, and episodic nature of disability. 19 The HDQ demonstrated sensibility, validity, internal consistency reliability, and test–retest reliability in samples of adults living with HIV in Toronto, Canada and Dublin, Ireland. 23
The WHODAS 2.0 is a generic 36-item disability self-reported questionnaire that can measure health and disability in the general population across 6 domains: (1) cognition, (2) mobility, (3) self-care, (4) getting along, (5) life activities, and (6) participation. Participants are asked to rate the level of difficulty of each item on a scale ranging from 1 (none) to 5 (extreme). Each domain and total score can be calculated by summing the item scores and converting the summary score of each domain or total into a metric ranging from 0 to 100 (0 = no disability and 100 = full disability). 32 Given the similar concept measured by the WHODAS 2.0 (disability), domains in the WHODAS 2.0 may be considered analogous to the HDQ. (eg, For instance, cognition; mobility, self-care, and life activities; and getting along and participation subscales on the WHODAS 2.0 may be considered analogous to the cognition; difficulties with day-to-day activities; and social inclusion domains in the HDQ, respectively. Furthermore, the WHODAS 2.0 has been used with people living with HIV 33 and possesses reliability, validity, and responsiveness among people with chronic disease. 34 The WHODAS 2.0 was also used for prior HDQ construct validity assessment in Canada and Ireland. 23 Hence, we chose the WHODAS 2.0 as our generic disability criterion measure to assess construct validity of the HDQ in this study.
We administered a demographic questionnaire to describe participant personal and clinical characteristics such as age, gender, employment status, antiretroviral therapy use, and self-reported concurrent health conditions.
To assess construct validity, given no “gold standard” exists for disability, we assessed the accuracy of the HDQ by testing 15 a priori hypotheses about predicted relationships between scores on the generic criterion measure of disability (WHODAS 2.0) and scores of the HDQ. Hypotheses included convergent construct validity testing to predict moderate (≥ 0.50) or strong (≥ 0.70) relationships between HDQ and WHODAS 2.0 scores.
To assess test–retest reliability, we administered the HDQ a second time, 1 week later. At the second administration of the HDQ, we asked participants if they had any major changes in their health over the past week (yes or no). We chose a 1-week interval because it minimizes participant recall of the items while reducing the possibility of a true clinical change causing a different in measurement. 35
In order to detect a weak correlation (r = 0.30) from our construct validity hypothesis, with a power of 0.80 and an α of 0.05, we required at least 85 participants for the analysis. 36 To adjust for an estimated 20% of questionnaires with missing responses, we required at least 102 participants in the study.
Analysis
For the demographic data, we calculated medians and interquartile ranges (IQRs) for continuous data and frequencies and proportions for categorical data.
HIV Disability Questionnaire
We calculated disability presence, severity, and episodic scores on the HDQ. 19 Disability presence scores were calculated by summing the number of health challenges experienced for each domain and total HDQ scale and transforming them to a score out of 100. Disability severity scores were calculated by summing individual item scores from each domain and then transforming them into severity scores out of 100. Episodic disability scores were calculated by summing the number of challenges identified as episodic in each domain and then transforming them to a score out of 100. We summed the number of participants who completed the HDQ on a “good day” or “bad day” living with HIV (health classification). We computed missing response rates for the disability, episodic, and health classification sections of the HDQ accordingly. To maximize our use of the HDQ data, we performed mean (severity) and median (episodic) imputation on items with less than ≤15% missing responses. For cases with >50% of missing data on the HDQ or WHODAS 2.0 criterion measure, listwise deletion was performed.
Internal consistency reliability
We calculated the Cronbach α (severity scale) and Kuder-Richardson-20 (KR-20) (episodic scale) statistics for each domain to assess internal consistency reliability (degree to which the items within the instrument are correlated with each other; α and KR-20 >0.8 defined as acceptable for individual patients). 37
Construct validity
We determined the extent to which the HDQ relates or does not relate to the WHODAS 2.0 questionnaire using correlation analysis. We tested 15 a priori hypotheses theorizing relationships between data collected from the HDQ severity scores and criterion measures using correlation coefficients (Pearson if scores normally distributed, Spearman if not normally distributed). Our a priori hypotheses were based on the extent to which we felt domains in the WHODAS 2.0 would map onto similar or distinct domains of the HDQ, consistent with our previous construct validity assessment of the HDQ using the WHODAS 2.0. 23 For instance, for domains comprised of items that we theorized measured a similar construct, we hypothesized a strong relationship (convergent construct validity), whereas for domains with items we considered measured distinct or less similar constructs, we hypothesized a weak relationship (divergent construct validity). Correlation coefficients of | ≥ 0.30|, | ≥ 0.50|, and | ≥ 0.70| were defined as “weak,” “moderate,” and “strong,” respectively. 38 We considered the HDQ severity scale to possess construct validity if results confirmed at least 75% of the predetermined hypotheses. 26
Test–retest reliability
We calculated the intraclass correlation coefficient (ICC) of HDQ severity scores for time 1 and time 2 scores for participants who did not have a change in their health status defined as (1) indicating they did not have a change in their overall health status between time 1 and time 2 and (2) responding similarly to item #70 of the HDQ (completing the HDQ on a “good day” or “bad day”) at time 1 and time 2, 1 week later. We considered an ICC >0.80 as acceptable for demonstrating consistency of the HDQ severity scale in measuring disability over time. 35
Ethical Approval and Informed Consent
All participants provided informed written consent to participate in the study. This study was approved by the institutional review board of Rutgers University (protocol #Pro20150001442) and HIV/AIDS Research Ethics Board at the University of Toronto (protocol #32633).
Results
Of the 132 participants who were recruited, 128 completed the HDQ at time 1 and 87 (68%) completed the HDQ at time 2. The majority of participants were male (68.3%), with a median age of 51 years (55.6% were ≥50 years) and a median of 16 years since HIV diagnosis. The majority were taking antiretroviral therapy (96.0%) and 93.7% had an undetectable viral load (Table 1). Participants were living with a median of 5 concurrent health conditions in addition to HIV (IQR: 2, 7); 88.3% of participants reported living with at least 1 concurrent health condition and 75.8% with at least 2 or more concurrent health conditions. The most common concurrent health conditions were joint pain (56.9%), muscle pain (49.6%), hypertension (47.1%), and mental health condition, such as anxiety or depression (40.3%; Table 1).
Characteristics of Participants.a
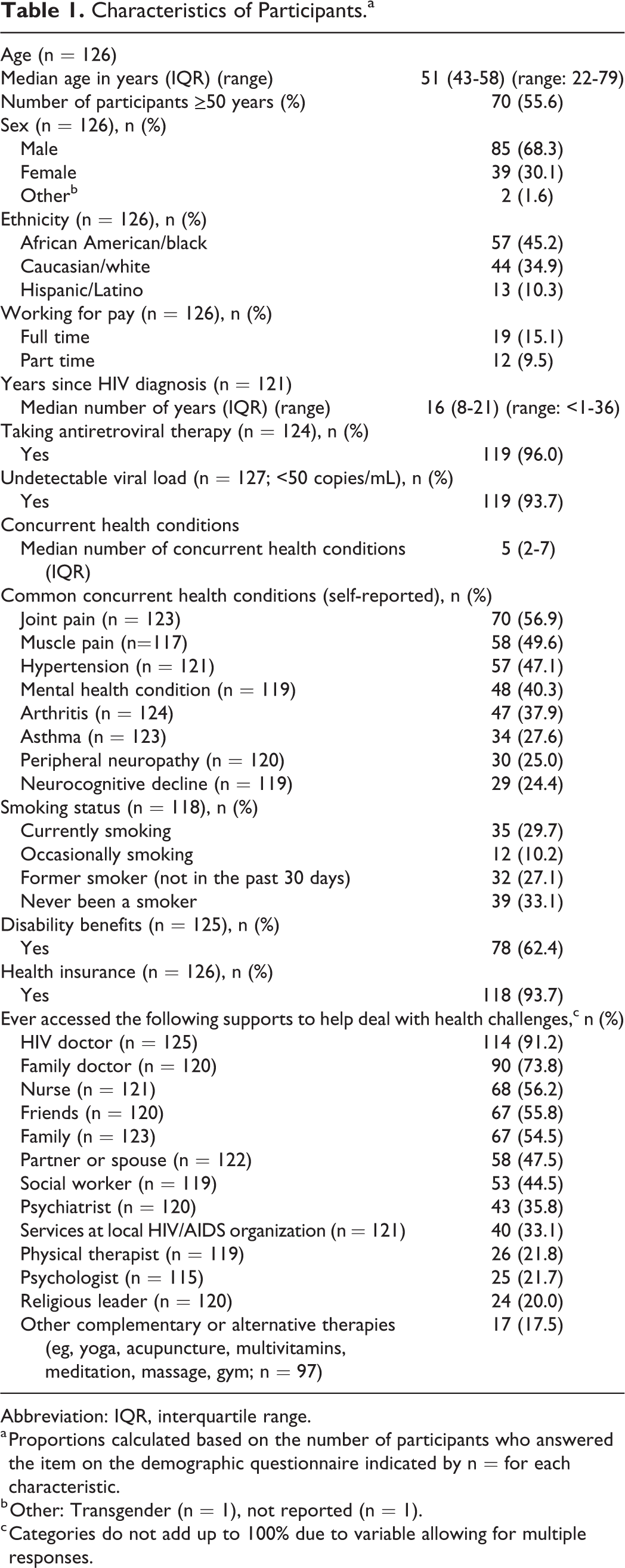
Abbreviation: IQR, interquartile range.
a Proportions calculated based on the number of participants who answered the item on the demographic questionnaire indicated by n = for each characteristic.
b Other: Transgender (n = 1), not reported (n = 1).
c Categories do not add up to 100% due to variable allowing for multiple responses.
HIV Disability Questionnaire
The proportion of missing responses at the item level was <4% for the severity scale and <12% for the episodic scale. There were 10 (7.8%) missing responses for the “good day/bad day” item on the HDQ. The highest HDQ disability presence score was in the uncertainty domain, followed by cognitive symptoms, physical symptoms, difficulties with day-to-day activities, mental–emotional health symptoms, and challenges to social inclusion. Highest disability severity score was in the uncertainty domain, followed by physical symptoms, challenges to social inclusion, mental–emotional symptoms, and difficulties with day-to-day activities and cognitive symptoms. Physical symptoms had the highest episodic score (Table 2). The number of participants who identified as completing the HDQ on a “good day” living with HIV was 97 (82%).
HIV Disability Questionnaire Summary Scores.a

Abbreviations: HDQ, HIV Disability Questionnaire; IQR, interquartile range.
a n = 128. Bold results indicate the highest score across the domains.
Of the 124 participants who completed the WHODAS 2.0 questionnaire, domain scores ranged from 0 (IQR: 0-20) on the self-care subscale to 33 (IQR: 8-52) on the participation subscale, with a median WHODAS 2.0 total score of 25 (IQR: 8-42).
Internal Consistency Reliability
Cronbach α for the entire HDQ severity scale was 0.97 (95% confidence interval [CI], 0.96-0.98) and ranged from 0.88 (0.85-0.92) in the social inclusion domain to 0.93 (0.92-0.95) in the uncertainty domain. The KR-20 statistic for the entire episodic HDQ scale was 0.98 (0.97-0.99) and ranged from 0.86 (0.80-0.93) in the episodic cognitive domain to 0.96 (0.94-0.97) in the episodic uncertainty domain (Table 3).
Internal Consistency Reliability and Test–Retest Reliability of the HIV Disability Questionnaire.a

Abbreviations: CI, confidence interval; HDQ, HIV Disability Questionnaire; ICC, intraclass correlation coefficient.
a n = 128.
b Median imputation of episodic scores; ICC analysis included 61 participants.
Test–Retest Reliability
Sixty-one participants reported having no major change in their health status and reported no change in the type of day they completed the HDQ (good day/bad day) between time 1 and time 2 and were included in the test–retest reliability analysis. The HDQ scores were consistent over time, with ICC values ranging from 0.88 (95% CI, 0.72-0.94) in the physical, cognitive, and social inclusion domains to 0.92 (95% CI, 0.82-0.96) in the mental–emotional domain (Table 3).
Construct Validity
Of the 15 construct validity hypotheses examining associations between HDQ and WHODAS 2.0 subscale and total scores, 13 (87%) were confirmed (Table 4).
Construct Validity Analysis of the HIV Disability Questionnaire.a,b

Abbreviations: CI, confidence interval; HDQ, HIV Disability Questionnaire; WHODAS, World Health Organization Disability Assessment Schedule II.
a n = 124.
b All correlation coefficients significant (P < .0001).
c Construct validity hypothesis confirmed: 13 of 15.
Discussion
The HDQ demonstrated internal consistency reliability, construct validity, and test–retest reliability with a community-dwelling sample of males living with HIV in the United States. Internal consistency reliability was achieved with Cronbach α and KR-20 statistics >0.80 across all domains and total episodic and severity HDQ scores. This suggests that the HDQ items within each of the 6 domains are homogenous in measuring a given domain concept and, together, collectively measure the broader construct of disability. 35 Construct validity was achieved as demonstrated by 87% (13/15) of hypothesized relationships confirmed between the HDQ and WHODAS 2.0 criterion measure scores, which surpassed the recommended 75% threshold for construct validity. 26 The HDQ demonstrated consistency in measuring disability over time as demonstrated by ICCs ≥0.88 across all HDQ domains. Our results build on previous evidence demonstrating reliability and validity of the HDQ when administered to adults living with HIV in Canada, 23,24 Ireland, 23 and the United Kingdom 25 and provide the first assessment of HDQ measurement properties among adults with HIV in the United States.
Internal consistency reliability results in this US sample were similar for HDQ severity and episodic domains among adults living with HIV in Canada (α range: 0.87-0.93; KR-20 range: 0.81-0.95), 23 Ireland (α range: 0.84-0.92; KR-20 range: 0.84-0.94), 23 and the United Kingdom (α range: 0.85-0.93; KR-20 range: 0.74-0.91), 25 suggesting the ability of the HDQ to measure disability in different high-income contexts among adults living with HIV and multimorbidity with an undetectable viral load. The HDQ also possessed test–retest reliability for its consistency in measuring disability among adults with HIV who did not report a major change in health over the past week as demonstrated by ICCs >0.80 across all domains. Similar results were reported in the test–retest assessment of the HDQ with a Canadian sample living with HIV (n = 99), with an ICC ranging from 0.80 (cognitive domain) to 0.89 (challenges to social inclusion). 23 Finally, the HDQ demonstrated construct validity for its ability to measure disability for adults with HIV as indicated by our confirmed a priori hypothesized relationships between HDQ and criterion measures (87%), which is similar to results in Canada (80%) 23 and the United Kingdom (83%). 25 However, we used 1 criterion measure in this study as opposed to other assessments that used different numbers and types of criterion measures (Canada assessment used 3 including the WHODAS 2.0 23 and the UK assessment used 9 that did not include the WHODAS 2.0) 25 , resulting in different types and number of hypothesized relationships. Hence, it is not possible to directly compare the construct validity of the HDQ across settings.
Although the HDQ overall demonstrated validity and reliability for use among this sample of adults with HIV in the United States, variation in HDQ scores and properties can exist across different cultural contexts. Diversity in clinical and demographic characteristics among sample populations, recruitment procedures, and mechanisms in which the HDQ and criterion measures were administered may account for differences in HDQ scores and measurement property coefficients. Among assessments of the HDQ measurement properties to date, participants in this study appeared most analogous to the Canadian sample of adults living with HIV, which similarly comprised of mostly men living with an HIV diagnosis for a median of ≥15 years and median of 4 self-reported concurrent health conditions in addition to HIV, with less than one-third (21%-25%) working for pay. 23 In contrast, participants in the Ireland and UK HDQ samples tended to be more employed, younger (median of 41 years in Ireland, 40 years in the UK), and living with fewer median number of concurrent health conditions. 23,25 Collectively, the HDQ appears to demonstrate properties of validity and reliability among community-dwelling adults living with HIV in high-income settings. 23 Nevertheless, properties of PROMs are specific to the target population and context in which it is assessed 26 ; hence, future research should examine the cross-cultural validity of the HDQ.
Findings from this study indicated that uncertainty or worrying about the future was the most present and severe domain of disability experienced among this sample of adults living with HIV in the United States. These results are consistent with previous studies that similarly reported uncertainty as the most prevalent and severe domain of disability experienced by adults with HIV 23,25 and a strong predictor of mental health symptoms and challenges to social inclusion. 39 Uncertainty may be experienced by younger adults newly diagnosed with HIV 40 and older adults diagnosed with HIV in the precombination antiretroviral therapy era 41 –44 who may worry about HIV age-related uncertainty, such as sources of health challenges, knowledge of health providers, financial uncertainty, transition to retirement, and worrying about appropriate long-term care and housing aging with HIV. 43,45 Strategies used by people living with HIV to cope with uncertainty may include utilizing social support networks 43,46 and self-management skills, as well as focusing on self-acceptance to gain a sense of control. 40,42,47 In our study, the highest episodic scores indicating the most fluctuating types of disability were physical symptoms and impairments, similarly observed in Canada, 23 Ireland, 23 and the United Kingdom. 23 Further exploration is needed to examine potential strategies to mitigate uncertainty living with HIV and the episodic health challenges experienced over the longer term across the life course among adults aging with HIV in the United States.
Evidence assessing disability among people living with HIV in the United States to date has focused primarily on individual domains of disability. For instance, physical disability among adults with HIV was reported in the form of reduced exercise tolerance, balance and gait impairments, 8 and reduced physical function as measured by the self-reported SF-36 physical function domain. 48,49 Alternatively, health-related quality of life is commonly conceptualized and measured as multidimensional, as demonstrated by the patient-reported quality of life HIV questionnaire developed to assess physical, mental, and social impairments among adults with HIV. 50 Multidimensional forms of disability have been assessed using the generic WHODAS 2.0 questionnaire in the South African context with adults with HIV. 51 –53 However, the HIV-specific HDQ goes beyond existing questionnaires and is the first to consider uncertainty as a dimension and the episodic nature of disability among adults with HIV.
Establishing the HDQ as a valid and reliable self-reported PROM of disability has important implications for future clinical practice and research. Clinicians, researchers, community-based organizations, and people with HIV may be able to use the HDQ as a universal screening tool to document the nature, extent, and burden of disability aging with HIV, facilitate communication among patients and providers, assist with goal setting, and help guide referrals to health services, such as rehabilitation. 54 Physical therapy and occupational therapy interventions include goal-oriented and individualized approaches to preventing or reducing disability experienced by people living with HIV and multimorbidity. 55,56 While few have access to formalized rehabilitation services, 57 many adults with HIV adopt living strategies in order to deal with their disability. 40 These include engaging in regular physical activity and social interactions to mitigate uncertainty, physical, and mental–emotional health challenges with HIV. 40,58,59 When administered cross-sectionally at one point in time, the HDQ is limited to capturing episodes of disability that occur on a daily basis as measured by the episodic portion of the scale, which asks whether a given health-related challenge fluctuated in the past week. Items in the social inclusion domain tend to pertain to employment or relationships, which are less likely to fluctuate within a given week, whereas items in the physical symptoms and impairments domain (eg, pain, headaches, fatigue) may fluctuate daily, or even sometimes within the course of day. Standardized ongoing clinical measurement of disability may contribute to future longitudinal tracking of episodic disability trends to help inform health services resource allocation and support the need for flexible income and employment programs and policies to enhance social inclusion for people with HIV.
Although we followed guidelines for assessing measurement properties of health status instruments, 60 our study is not without limitations. First, the sample comprised primarily middle-aged community-dwelling males living with multimorbidity and well-controlled HIV in southern New Jersey. Our study builds on others that demonstrated HDQ validity and reliability among similar samples in Canada, 23,24 the United Kingdom, 25 and Ireland, 23 strengthening the case for our ability to use the HDQ in high-income settings. Nevertheless, these properties may not translate to other contexts, highlighting the need for further property assessment in low- to middle-income settings among adults living with HIV. Second, we used only 1 criterion measure to assess construct validity, which may have resulted in the high number of confirmed hypotheses subsequently overestimating the construct validity of the HDQ. Third, 68% of participants returned for the time 2 HDQ administration, a lower completion rate compared to the test–retest time 2 administration in Canada (100%). 23 Although we did not ask participants details about why they did not return for the time 2 administration, we expect reasons may have been attributed to challenges securing transportation or the inconvenience returning to the clinic on a day when otherwise not attending for a medical appointment. Next, assessment of the meaning of HDQ scores (interpretability) and the ability of the HDQ to detect change in disability when change occurs (responsiveness) is in underway 61 ; hence, these scores should be interpreted cautiously. Lastly, to date, the HDQ has primarily been used in research contexts. Future inquiry should examine the utility and feasibility of the HDQ in clinical practice.
In conclusion, the HDQ possesses internal consistency reliability, test–retest reliability, and construct validity across domain scores when administered to adults living with HIV in the United States. Results are specific to a community-dwelling sample of adults living with HIV and multimorbidity. Future research should examine HDQ interpretability of scores, its ability to detect clinically important changes in disability, and its utility in clinical practice.
Footnotes
Acknowledgments
The authors acknowledge Rutgers, School of Health Professions, Dean’s Office, Voorhees Infectious Diseases (Jefferson Health), Voorhees, NJ, and study assistants Adam Huynh and Megan Meszaros from Rutgers.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was partially funded by the Dean’s Office, School of Health Professions at Rutgers. This research was undertaken, in part, thanks to funding from the Canada Research Chairs program. Kelly K. O’Brien is supported by a Canada Research Chair in Episodic Disability and Rehabilitation.