
Abstract
The study reports the response of first-line antiretroviral therapy (ART) by assessing CD4 and CD8 T-lymphocyte and viral load (VL) among Bangladeshi people living with HIV (PLHIV). This observational approach was conducted on 100 PLHIVs, grouped into therapy naive (n = 33), therapy initiators with CD4 T-cell count of <350 cells/µL (n = 33), and therapy receivers for >1 year prior to the study period (n = 34). Therapy initiators who continued the study (n = 20) were followed up after 12 and 24 weeks of therapy initiation. The CD4 and CD8 T-lymphocyte count estimation and (VL) were quantified. The mean CD4 T-lymphocyte count was significantly reduced among the therapy initiators in comparison to therapy naive and therapy receivers. Similar findings were observed for CD8 T-lymphocyte count among the study groups. The mean HIV-1 RNA VL among therapy initiators showed a significant decrease after 12 and 24 weeks, and 85% patients in this group obtained undetectable VL status indicating the good therapeutic outcome.
What Do We Already Know about This Topic?
Antiretroviral therapy (ART) has a great role in HIV suppression in blood and body fluids, thereby improving the immune status of the body to fight against opportunistic organisms.
How Does Your Research Contribute to the Field?
This research will be the first report of its kind on highlighting the response of first-line ART among the people living with HIV (PLHIV) from Bangladesh in improving immunological and virological status.
What Are Your Research’s Implications toward Theory, Practice, or Policy?
These research findings will plot further research on the therapeutic implication of other ART regimen and early detection of antiretroviral drug resistance.
Introduction
Laboratory monitoring for HIV disease is one of the key challenges in antiretroviral therapy (ART) initiation and success. The most common method for initiating ART and monitoring treatment response in resource-limited settings is the measurement of CD4 T-lymphocyte count. 1 In addition, HIV RNA viral load (VL) measurement is becoming increasingly important, not only for monitoring the response to ART but also to assess the potential for emergence of viral resistance or early therapeutic failure detection. 2 Bangladesh has a low prevalence of HIV infection since the detection of the first case in 1989. 3 At present, the overall prevalence of people living with HIV (PLHIV) among the general population is <0.1%, with a total of 6455 laboratory-confirmed HIV cases at the end of 2018 and 50% of them under the ART coverage. 4 With these low number of PLHIVs, Bangladesh is one of the 9 countries in the world where the estimated HIV incidence increased by 25% between 2001 and 2011. 5 Moreover, data from the National Surveillance of 2015 to 2016 revealed a concentrated epidemic among the male people who inject drugs in a neighborhood region of Dhaka city (the capital of the country), with a higher prevalence of 27.3%. However, it was >5% in both genders in the rest of the capital. 6
Information regarding laboratory monitoring and treatment responses among PLHIV from Bangladesh is yet very limited. Therefore, the present study evaluated the laboratory monitoring of Bangladeshi PLHIV and their response to ART by monitoring of CD4 and CD8 T-lymphocyte count and plasma VL in the context of resource-limited settings.
Methods
This observational cohort study was conducted among Bangladeshi adult PLHIV attending the daycare unit of the Ashar Alo Society, a nongovernment organization (NGO) caring for PLHIV. Estimation of CD4 and CD8 T-lymphocyte counts and HIV-1 VL measurement were performed at the Department of Virology, Bangabandhu Sheikh Mujib Medical University (BSMMU). The study population comprised of 100 purposively selected patients who were classified as therapy naive (n = 33), therapy initiators (n = 33) with baseline CD4 T-lymphocyte count <350 cells/µL of blood, and therapy receivers (n = 34) for >1 year prior to study. Patients from therapy-naive and therapy receiver groups were selected by systematic random sampling. Therapy initiators were prescribed ART following the national ART guidelines, 7 and this particular cohort was followed up after 12 and 24 weeks of therapy initiation. CD4 and CD8 T-lymphocyte counts from whole blood were performed on all patients by fluorescence-activated cell sorting (FACS) system (Becton Dickenson Immunocytometry System, San Jose, California), and the plasma HIV-1 RNA was measured by a quantitative reverse transcriptase polymerase chain reaction (AJ Roboscreen GmbH, Leipzig, Germany), as described previously. 8 HIV-1 RNA monitoring in plasma was determined on a total of 54 patients, consisting of 10 therapy naive, 33 therapy initiators, and 11 therapy receivers >1 year. Statistical analysis was performed using the SPSS 19.0 software, and the result with P < .05 was considered significant.
Treatment Regimens
The therapy initiators and therapy receivers for >1 year were treated with the first-line regimens (combination of 2 nucleoside reverse transcriptase inhibitors and 1 non-nucleoside reverse transcriptase inhibitor) following the national ART guidelines. 7 The antiretroviral drugs were supplied and given free of cost by the National AIDS/STD Program (NASP), Bangladesh. The first-line ART regimens used in this cohort were zidovudine (ZDV)-based ART. The most frequently used regimens were (1) ZDV + lamivudine (3TC) + nevirapine (NVP) and (2) AZT + 3TC + efavirenz (EFV). Regimen (1) consisted of ZDV (300 mg), 3TC (150 mg), and NVP (200 mg) combined in single pill (twice daily), and regimen (2) consisted of ZDV (300 mg) and 3TC (150 mg) combined in single pill (twice daily) with EFV (600 mg) once daily (at bedtime).
Ethical Approval and Informed Consent
The study was approved by the institutional review board of BSMMU, Dhaka, Bangladesh (approval number BSMMU/2010/12167 (A); Date: 15/12/2010), and written informed consent was obtained from all participants at enrollment in this study.
Results
Among the 100 PLHIVs, 53% were males, 43% were females, and 4% were transgenders. The age of participants in the study population ranged from 19 to 60 years (mean [standard deviation]: 33.53 [9.07] years). The most frequent (84%) mode of transmission was heterosexual contact.
CD4 and CD8 T-Lymphocyte Counts and CD4–CD8 Ratio at Entry into the Study
The distribution of CD4 and CD8 T-lymphocyte counts and CD4–CD8 ratio of the study population at the beginning of the study is shown in Table 1. The mean CD4 and CD8 T-lymphocyte counts were 591 ± 217 cells/µL, 155 ± 127 cells/µL, and 588 ± 228 cells/µL among therapy naive, therapy initiators, and therapy receivers, respectively, at the beginning of the study. Among therapy-naive cases, none had CD4 T-lymphocyte counts <350 cells/µL, 14% had counts within 351 to 500 cells/µL, but the remaining 57% had >500 cells/µL. In contrast, all therapy initiators had CD4 T-lymphocyte count <350 cells/µL (P < .001). Among therapy receivers, only 5 (15%) had CD4 T-lymphocyte count <350 cells/µL, 8 (24%) had counts within 351 to 500 cells/µL, while 21 (62%) had counts >500 cells/µL.
Distribution of CD4 and CD8 T-Lymphocyte Count and CD4–CD8 Ratio of Study Population at Beginning of the Study.
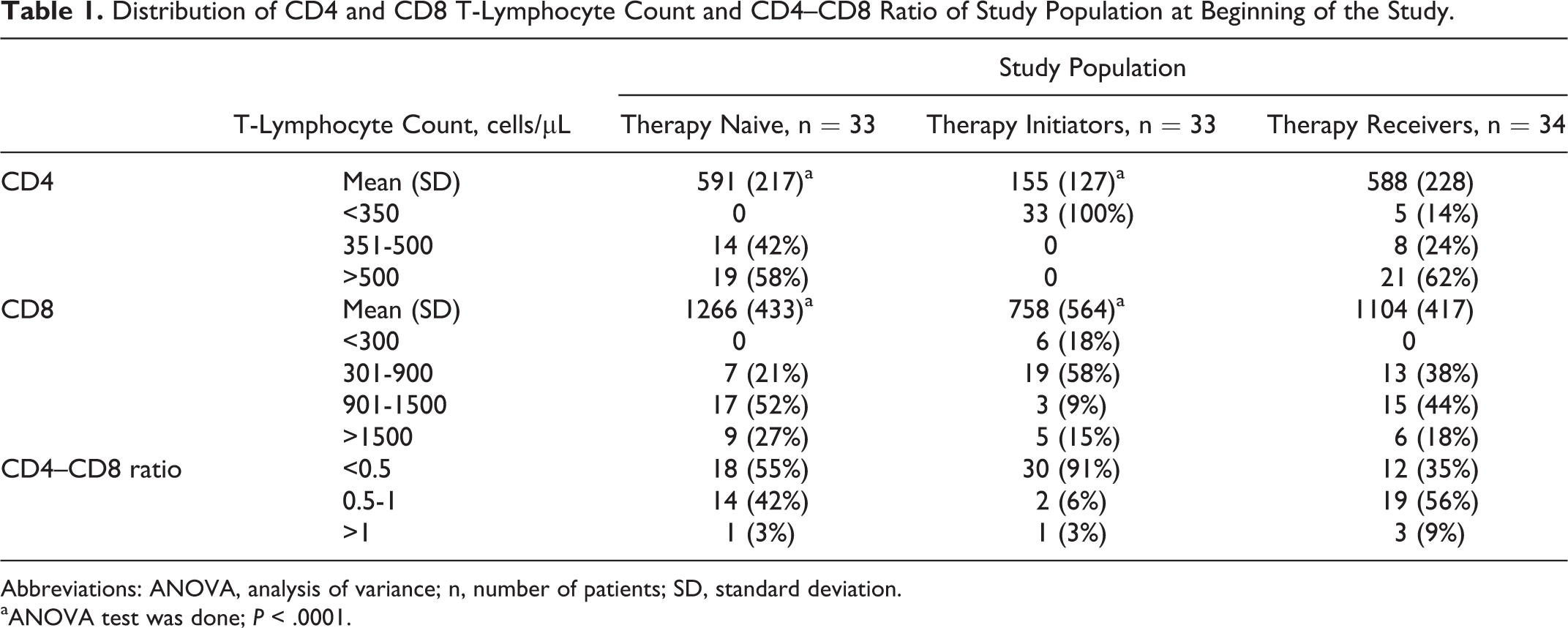
Abbreviations: ANOVA, analysis of variance; n, number of patients; SD, standard deviation.
aANOVA test was done; P < .0001.
The mean CD8 T-lymphocyte count was significantly higher among therapy naive and therapy receivers at the beginning of the study in comparison to therapy initiators (P < .001). Among therapy naive and therapy receivers, none had CD8 T-lymphocyte count <300 cells/µL. A mean CD8 T-lymphocyte of <900 cells/µL was observed among 25 (76%) therapy initiators, with 6 (18%) having counts <300 cells/µL and 19 (56%) with counts within 301 to 900 cells/µL. Mean CD8 T-lymphocyte of <900 cells/µL was also observed among 7 (21%) therapy naive and 13 (38%) therapy receivers. In contrast, CD8 T-lymphocyte counts of >1800 cells/µL were observed among 20% of the study population.
The CD4–CD8 ratio among 12 (42%) therapy naive and 19 (56%) therapy receivers ranged from 0.5 to 0.99. Among therapy initiators, CD4 T-lymphocyte count was significantly lower causing the ratio to be more inverted when compared to the other 2 groups. A ratio of <0.5 was observed in 30 (91%) therapy initiators, 55% of therapy naive, and 35% of therapy receivers.
Plasma HIV-1 RNA VL Concentration at Entry Into the Study
The results of VL determination performed on all 33 therapy initiators, 10 (30.3%) therapy naïve, and 11 (33.3%) therapy receivers at the beginning of the study are shown in Table 2. Among the therapy receivers, significantly lower level of VL (0.63 ± 1.21 log10 copies/mL, [range: <0.48-3.45]) was observed in comparison to the therapy naive and therapy initiator groups (P < .0001). However, all the therapy initiators had higher VL (5.43 ± 1.32 log10 copies/mL [range: 2.19-7.38]) than therapy-naive (4.87 ± 0.92 log10 copies/mL, [range: 3.02 to 6.11]) patients.
Distribution of HIV-1 VL Status of Study Population at the Beginning of the Study.

Abbreviation: VL, Viral load.
Changes in CD4 and CD8 T-Lymphocyte Counts and HIV-1 VL among Therapy Initiators Before and After ART Initiation
Of the 33 therapy initiators, 6 patients dropped out after 12 weeks and another 7 patients dropped out after 24 weeks of the study. The reason for dropout was that PLHIVs moved to another NGO for their necessary care and support. As such, only 20 (60.6%) patients who completed the whole period of the study were included in the final analysis. Among the 20 therapy initiators who were retested after 12 and 24 weeks, there was a progressive biphasic increase in mean CD4 and CD8 T-lymphocyte counts from baseline values after 12 and 24 weeks of ART initiation (Table 3). A significant increase in CD4 T-lymphocyte count from 177 ± 127 cells/µL (range: 2-349) to 368 ± 181 cells/µL (range: 90-750; P < .0001) was observed after 12 weeks, and this significant increasing trend persisted after 24 weeks when the CD4 T-lymphocyte count increased to 452 ± 183 cells/µL (range: 157-875; P < .0001). However, the increase in mean CD4 T-lymphocyte count after initiation of ART was more apparent after 12 weeks. Similar patterns of increase in CD8 T-lymphocyte count from baseline values was observed after 12 and 24 weeks of ART initiation (901 ± 650 cells/µL, 1085 ± 393 cells/µL, and 1121 ± 372 cells/µL, respectively) from baseline to week 24, but this trend of increase was not statistically significant (P > .05). Following ART initiation among the 20 therapy initiators who followed up the entire study period, a significant decrease in VL was observed over time (P < .001), and after 12 weeks, 15 (75%) of these 20 therapy initiators attained undetectable VL (P < .0001). After 24 weeks of ART, the remaining 5 patients with detectable VL (3.40 ± 1.57 log10 copies/mL [range: 1.44-5.83]) were retested, whereby 2 (10%) more patients were found to attain undetectable VL (Table 3).
Results of CD4 and CD8 T-Lymphocyte Count and HIV-1 VL among Therapy Initiators Before and After ART Initiation.a

Abbreviation: VL, Viral load; SD, standard deviation.
aVL < 0.48 log10 copies/mL (<3 copies/mL) denotes VL below the level of detection. VL = 0.48-9.70 log10 copies/mL (3-5 × 109 copies/mL) denotes positive VL.
bPaired t test done, P < .0001.
CD4 and CD8 T-Lymphocyte Counts, CD4–CD8 Ratio, and HIV-1 VL among Therapy Initiators Who Did Not Achieve Undetectable VL Status at the End of the Study
The CD4 and CD8 counts, CD4–CD8 ratio, and HIV-1 VL of 3 therapy initiators who did not achieve undetectable VL status are shown in Table 4. The CD4 T-lymphocyte count of patient 1 did not vary very much (323-355 cells/µL) during the study period. However, CD4 T-lymphocyte count of patients 2 and 3 increased from 144 to 511 and 331 to 560 cells/µL during the study period. Similarly, CD8 T-lymphocyte count of all the 3 therapy initiators were also found to increase from the baseline, and among them, a sharp increase was noted in patient 2 (548-1006 cells/µL). In case of VL count, all the 3 therapy initiators showed declining trends of VL status from baseline to final evaluation. Patient 3 showed increased VL count (3.37 log10 copies/mL) at 24 weeks from VL count (1.44 log10 copies/mL) at 12 weeks, although both counts were lower than the baseline VL (4.50 log10 copies/mL). Despite having a narrow increase in CD4 T-lymphocyte count in patient 1, VL count decreased to 3.22 log10 copies/mL from the baseline (6.75 log10 copies/mL), whose baseline VL was the highest among the 3 therapy initiators.
CD4 and CD8 Count and CD4–CD8 Ratio and HIV-1 VL among Therapy Initiators Who Did Not Achieve Undetectable VL Status After the End of the Study.
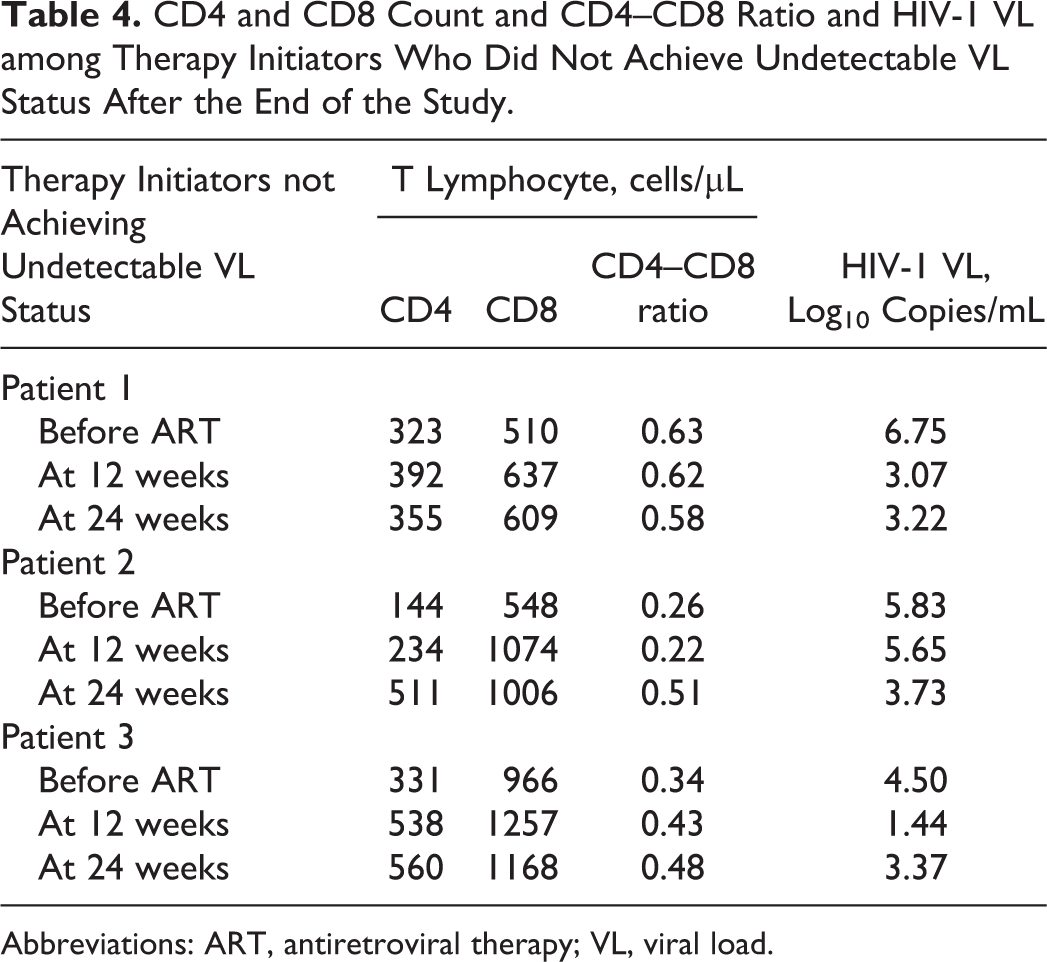
Abbreviations: ART, antiretroviral therapy; VL, viral load.
Discussion
Regular patient evaluation by laboratory monitoring is important for HIV care, especially upon commencement to care, during follow-up prior to initiation of ART, before and after ART is initiated, or any regimen changes. Currently, the evaluation of the progression of HIV infection is estimated by 2 important surrogate markers, the CD4 T-lymphocyte count and HIV VL measurements. The introduction of ART has significantly improved survival rates among HIV-infected individuals through an increase in the CD4 T-lymphocyte count and reduction in HIV VL to undetectable levels. 9 In response to worldwide demand and increased funding, implementation of ART is proceeding rapidly in the developing world and has greatly contained the AIDS epidemic in resource-poor countries. However, the use of laboratory monitoring of patients taking ART remains a challenge in low-income settings. 10
Bangladesh being a country with low prevalence for HIV, it remains extremely vulnerable due to poverty, overpopulation, gender inequality, high mobility of the population within the country, and high levels of transactional sex. Migration to other countries for employment is also very common, particularly among younger people. Stigma and discrimination against PLHIV is prevalent in this country and inhibits both the physical and mental well-being of those carrying the HIV and often many adverse consequences among the general populations, such as delay in HIV testing, the restricted adoption of preventive programs, and preventative behaviors such as condom use and HIV status disclosure, barriers in a normal socioeconomic livelihood, and so on. 11 The National AIDS Committee is the highest decision-making body on issues related to AIDS and other sexually transmitted infections and acts as an advisory body responsible for formulating major policies and strategies on HIV and AIDS, and the NASP is the body working under the Ministry of Health and Family Welfare to manage and coordinate the National AIDS Program in the country. In Bangladesh, treatment, care, and support services for PLHIV have been provided through designated government hospitals through collaboration with NGOs dealing PLHIVs. 12 From 2011, the Department of Virology of BSMMU, Dhaka, which is the National HIV Reference Laboratory, started monitoring CD4 and CD8 T-lymphocyte counts and HIV VL among PLHIVs in addition to their ongoing HIV screening and confirmation services for the general populations. 13
Our study observed a significant reduction in CD4 T-lymphocyte count among all therapy initiators in contrast to therapy-naive and therapy receiver groups. Similar findings have been reported in a previous study from Bangladesh 8 and from other countries in this region. 14,15 A considerable increasing trend of CD4 T-lymphocyte among the study cohort was observed after 12 weeks of ART initiation, which continued even after 48 weeks. This finding indicates the beneficial effect of ART on limiting the progression of HIV infection. 16,17 It is suggested that in the initial period, ART is efficacious in reducing VL rapidly, and the immune system of the body quickly generates CD4 T-lymphocytes to combat HIV infection. 18
In contrast, the mean CD8 T-lymphocyte count was high among all the 3 study groups, with higher values among therapy naive and therapy receivers. However, a significantly low mean CD8 T-lymphocyte count (<900 cells/µL) was observed among 76% therapy initiators, 38% therapy receivers, and 21% therapy-naive patients. Low absolute CD8 counts correlate with poor survival outcomes in both ART-naive and experienced patients. 19,20 A low CD4–CD8 ratio was observed among 60% of our study population but was predominant among the therapy initiators (30/33), signifying a gradual worsening of their immune response.
Although monitoring of VL is critical for assessing the efficacy of ART, findings from multiple studies support the association between greater virological suppression and sustained the virological response to ART. 21,22 Guidelines define virological failure as either a failure to achieve an undetectable HIV-RNA (<50 copies/mL) after 6 months or a sustained HIV-RNA >50 copies/mL or >400 copies/mL following suppression below this level. 21 A greater than 3-fold increase in VL has been associated with an increased risk of clinical deterioration, and this value is recommended to guide therapeutic regimen change in the developed world. 23,24 Several studies have shown a significant correlation between HIV-RNA >10 000 copies/mL and increased mortality and morbidity. Thus, therapeutic switching is suggested prior to this point. Accordingly, the World Health Organization recommends that this level should be considered as the definition of virological failure in resource-limited settings. 25
Our study revealed efficacious viral suppression among the 85% of therapy initiator cohort after ART initiation. A similar pattern of study from India showed the good therapeutic response of more than 85% individuals experiencing complete viral suppression. 26 Incomplete viral suppression noted among the 3 therapy initiators in our study has raised the issues related to clinical and immunological failure due to a failing ART regimen or probable amplification of drug resistance. 27 It is to mention here that detection of drug resistance in those patients was beyond the scope of the facility, and we had to rely on the patients’ statement regarding regular drug intake during the follow-up sessions of the study period. However, the decreasing trend of VL from their initial status indicates that these 3 patients were slowly achieving sustained virological control over HIV-1 RNA, 28 demonstrating good first-line ART response among the Bangladeshi HIV-infected population. Thus, it can be assumed that, if these patients could be followed further, they may have eventually achieved undetectable VL status. Furthermore, the minor increase in VL at week 12 in patient 3 may possibly be due to nonadherence to therapy, holding therapy for the development of metabolic toxicities or any others unnoticed possibilities. 29 None of these 3 patients need to switch or modify therapy due to interaction with other coadministered drugs. Nevertheless, with the good VL response in our study through commonly available and cost-effective first-line ART regimens, the findings of our study need to be interpreted with caution considering the low number of the study cohort.
Overall, our study observed that an increasing trend of CD4 T-lymphocyte count was associated VL suppression in patients on ART. The benefits seen in this study appeared to apply irrespective of whether viral suppression was continuous or episodic. The results of our study delivered evidence of immunological and virological benefit for timely initiated ART when the patient’s CD4 T-lymphocyte count was <350 cells/µL.
Expansion of both treatment and prevention activities is a major achievement in the global response to HIV/AIDS. However, late presentation of many HIV-infected individuals to ART programs in resource-poor countries firmly suggests the importance of HIV testing and counseling to promote earlier ART initiation. Thus, efforts are required to establish easily accessible PLHIV care and support centers with the provision of cost-effective laboratory monitoring facilities in the context of resource-limited settings. Furthermore, an introduction of simple, low-cost, and easy-to-use laboratory monitoring assays should be actively promoted in these settings, since the benefit of the scaling up of ART seems to be largely dependent on adequate laboratory monitoring. Hopefully, these efforts will lead toward substantial progress in winning the battle against HIV, not only by preventing further transmission but also by maximizing clinical benefits to the patients.
Footnotes
Acknowledgments
The authors acknowledge the Bangabandhu Sheikh Mujib Medical University (BSMMU) research grants committee for funding this project. The authors also like to acknowledge the kind support from Ashar Alo Society (AAS), a leading nongovernment organization dealing with PLHIV of Bangladesh during the recruitments and follow-up of the study participants. Lastly, the authors like to thank the study participants to contribute into this research work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: Financial support from the BSMMU research grants.