
Abstract
Cerebral toxoplasmosis is the most common cause of expansive brain lesions in people living with HIV/AIDS (PLWHA) and continues to cause high morbidity and mortality. The most frequent characteristics are focal subacute neurological deficits and ring-enhancing brain lesions in the basal ganglia, but the spectrum of clinical and neuroradiological manifestations is broad. Early initiation of antitoxoplasma therapy is an important feature of the diagnostic approach of expansive brain lesions in PLWHA. Pyrimethamine-based regimens and trimethoprim-sulfamethoxazole (TMP-SMX) seem to present similar efficacy, but TMP-SMX shows potential practical advantages. The immune reconstitution inflammatory syndrome is uncommon in cerebral toxoplasmosis, and we now have more effective, safe, and friendly combined antiretroviral therapy (cART) options. As a consequence of these 2 variables, the initiation of cART can be performed within 2 weeks after initiation of antitoxoplasma therapy. Herein, we will review historical and current concepts of epidemiology, diagnosis, and treatment of HIV-related cerebral toxoplasmosis.
Keywords
What Do We Already Know About This Topic?
Cerebral toxoplasmosis remains the most common cause of expansive brain lesions in people living with HIV/AIDS (PLWHA). This disease presents high morbidity and mortality, particularly in low- and middle-income countries. In daily practice, clinical and neuroradiological features establish the presumptive diagnosis. Pyrimethamine-based schemes are classically preferred when available. Brain biopsy is usually reserved for patients who fail to respond to 10-14 days of antiparasitic therapy.
How Does Your Research Contribute to the Field?
This article is a critical and historical review of the terminology, epidemiology, case definition, diagnosis, treatment, and pharmacological prophylaxis of cerebral toxoplasmosis in PLWHA. In addition, an algorithm for the management of patients with suspicion of cerebral toxoplasmosis is proposed.
What Are Your Research’s Implications Toward Theory, Practice, or Policy?
This article shows the broad clinical and neuroradiological spectrum of cerebral toxoplasmosis in PLWHA. In this scenario, early treatment is key for a good outcome. If safe and feasible, polymerase chain reaction of Toxoplasma gondii on cerebrospinal fluid should be performed. Early brain biopsy should be strongly considered if there is a high index of suspicion of an alternative diagnosis to cerebral toxoplasmosis. Local algorithm is important in the management of PLWHA-related expansive brain lesions. Currently, if we consider the available evidence and the potential practical advantages, trimethoprim-sulfamethoxazole can be considered the preferred treatment of cerebral toxoplasmosis. The immune reconstitution inflammatory syndrome is not a major concern with cerebral toxoplasmosis and cART can be started within two weeks after the initiation of antiparasitic treatment.
Introduction
Toxoplasma gondii is a ubiquitous, intracellular protozoan parasite that causes cosmopolitan zoonotic infection. Acute T gondii infection is usually subclinical in the vast majority of immunocompetent individuals, and it is very rarely associated with severe clinical manifestations. 1 On the other hand, cerebral toxoplasmosis is caused almost exclusively due to reactivation of latent brain cysts 2 and can cause devastating consequences in host immunocompromised patients, particularly in people living with HIV/AIDS (PLWHA). If untreated, cerebral toxoplasmosis is uniformly fatal. 1,3
Prior to 1980, cerebral toxoplasmosis was a rarely encountered complication of immunosuppression. The first cases of cerebral toxoplasmosis at the beginning of the AIDS epidemic were described between 1982 and 1983. 4 -6 As the number of PLWHA increased, cerebral toxoplasmosis became one of the most frequent opportunistic infections and the most common causes of focal brain lesions in this population. 7 The most accepted explanation to the strong association between reactivated cerebral toxoplasmosis and AIDS is that these immunocompromised patients have a disturbed antiparasitic T-cell response and therefore fail to control this intracellular persistent parasite. 8
Despite an important decline in both morbidity and mortality from countries with widespread access to combination antiretroviral therapy (cART), the occurrence of cerebral toxoplasmosis still represents a poor prognostic determinant in the natural history of PLWHA. 9 -11
Terminology
The predominant neuropathological hallmark of cerebral toxoplasmosis in PLWHA is multifocal necrotizing encephalitis. 12,13 However, the term “toxoplasma abscess” has been used by several authors from the beginning of the epidemic 4,14 -17 to more recent years. 18,19 Brain abscess is classically defined as intraparenchymal collection of pus, 20 -22 but HIV-related cerebral toxoplasmosis does not present pus. Brain abscess development can be divided into 4 histopathological stages: (1) early cerebritis, (2) late cerebritis, (3) early capsule formation, and (4) late capsule formation, pus can be observed in the last 3 stages. 23 In addition, a significant delay in the evolution of the stages of brain abscess can occur in an immunocompromised host. 24 Thus, early cerebritis that correlates better with the necrotizing encephalitis is characteristically observed in toxoplasmosis. 23 For this reason, the terms ”toxoplasmic encephalitis,” 7,25 -27 “toxoplasma encephalitis,” 28,29 or “cerebral toxoplasmosis” 30 -33 seem to be more appropriate than “toxoplasma abscess.”
Epidemiology
Toxoplasmosis is one of the most common infections in humans with a worldwide distribution, and it is estimated that about one-third of the global population is infected with latent toxoplasmosis. 34 The prevalence and burden of T gondii infection in PLWHA shows geographic variability and usually follows the prevalence of T gondii in general population. The prevalence of coinfection in low-income countries, middle-income countries, and high-income countries is 55%, 34%, and 26%, respectively. 35 Foci of high prevalence exist in Latin America, parts of Eastern/Central Europe, the Middle East, parts of Southeast Asia, and Africa. 36
Availability of cART significantly reduced the incidence of cerebral toxoplasmosis in PLWHA from high-income countries and middle-income countries. 9,10,37,38 In Brazil, where the prevalence of HIV in the general population was 0.4% in 2014, there has been an impressive decrease in the incidence rates of cerebral toxoplasmosis (43.6/1000 people-year [PY] between 1987 and 1990 and 4.0/1000 PY between 2009 and 2012; incidence rate ratio = 0.09, 2009-2012 versus 1987-1990; P < .001) 10 and in its case fatality rate from pre-cART era (∼90%) to the cART era (∼15%-30%). 39 However, the incidence rates of cerebral toxoplasmosis observed in Brazil are higher than those observed in other studies both from other middle- and high-income countries. 10 High prevalence of T gondii infection in the general population and specifically in PLWHA explains this scenario. 40 Other variables to persistent elevated incidence rates of cerebral toxoplasmosis observed in some settings include late HIV diagnosis, nonadherence to cART, failure of retention in care, and antiretroviral drug resistance. 10,39,41
Nowadays, HIV-related cerebral toxoplasmosis continues to be the most common cause of focal brain lesion and an important cause of morbidity and mortality in PLWHA in several low- and middle-income countries. 10,11,39,41 -43
Case Definition
The use of diagnostic categories has been widely implemented in some opportunistic neurological diseases (ie, tuberculous meningitis, progressive multifocal leukoencephalopathy [PML]).
44
-46
The case definition for cerebral toxoplasmosis can contribute to the design and comparison of studies, to scientific communication, and even to the management of the disease. The following diagnostic categories are proposed:
Histology-confirmed cerebral toxoplasmosis requires a compatible clinical syndrome, identification of one or more expansive focal brain lesions by imaging, and brain biopsy (or postmortem examination) showing evidence of T gondii. Histopathological demonstration most commonly is obtained by a stereotactic computed tomography (CT)-guided needle biopsy. Hematoxylin and eosin stains can be used to demonstrate tachyzoites of T gondii, mainly in the periphery of the lesions, but sensitivity is significantly increased if immunoperoxidase staining is used.
47
Laboratory-confirmed cerebral toxoplasmosis requires a compatible clinical syndrome, identification of one or more expansive focal brain lesions by imaging, and evidence of T gondii DNA in cerebrospinal fluid (CSF) by nucleic acid amplification assays.
Probable cerebral toxoplasmosis requires a compatible clinical syndrome, identification of one or more mass lesions by imaging, and unequivocal radiological response to 10 to 14 days of empiric antitoxoplasma therapy.
Possible cerebral toxoplasmosis requires a compatible clinical syndrome, identification of one or more mass lesions by imaging, presence of serum T gondii immunoglobulin G (IgG) antibodies, and no other alternative diagnosis.
The first two categories—histology-confirmed and laboratory-confirmed cerebral toxoplasmosis—can be considered a “definite” diagnosis. Probable cases correlate with “presumptive” diagnosis in clinical practice, considering the unnecessary use of histopathological studies in the vast majority of cases with cerebral toxoplasmosis and the unavailability of molecular diagnosis in most low- and middle-income countries. The possible cases category can be useful in some scenarios, for example, when patients eventually died or left the hospital within the first days of hospitalization without radiological control.
Syndromic Approach
The clinical presentations of neurological diseases in PLWHS are notably heterogeneous, nonspecific, and overlapping, but a correct diagnosis is essential for timely intervention. 7,48
There are at least 2 main ways to classify the AIDS-related neurological complications: (1) according to their etiological agent—primary (caused by HIV itself) or secondary (opportunistic infections or neoplasms) diseases, and (2) by their neuroanatomical localization—central nervous system (CNS) and peripheral nervous system. These 2 classifications are complementary and help order diagnostic probabilities. Among CNS diseases, brain neurological diseases can be classified according to the predominant neurological syndrome in meningitis or encephalitis. The encephalic syndrome can be classified into focal or diffuse brain lesion. Finally, focal brain lesions may or may not show expansive effect. 49 -52
Complementary to the syndromic diagnosis, 3 aspects are relevant to establish the most probable etiologies of expansive focal brain lesions in PLWHA: (1) local neuroepidemiology (ie, tuberculomas is usually more common than primary central nervous system lymphoma [PCNSL] in low- and middle-income countries) 53 -56 ; (2) degree of immunosuppression (ie, lymphocyte CD4 count <200 cells/mm3 suggests opportunistic diseases; PCNSL usually occurs with lymphocyte CD4 count <50 cells/mm3) 57,58 ; and (3) individual clinical, laboratorial, and neuroradiological features. 51
The management of expansive focal brain lesions in PLWHA in high-income countries and in some middle-income countries has undergone several changes in approaches throughout the AIDS epidemic. Initially, the main strategy was to try to perform a biopsy of all patients; subsequently, the importance of antitoxoplasma “empirical” therapy was established; finally, molecular diagnosis and functional neuroradiology were incorporated in some referral centers. 7,13,14,18,26,29,59 -61 Despite this chronology, all these tools continue to be important in managing focal brain lesions in PLWHA. However, the availability of resources is highly heterogeneous and generally scarce or absent where opportunistic diseases are most prevalent at present.
The risk of cerebral toxoplasmosis is markedly increased in PLWHA who are seropositive for T gondii IgG antibody, have a lymphocyte CD4 count <100 cells/mm3, and are not receiving regular and effective prophylaxis. 9,62 However, the absence of any combination of these variables does not rule out the possibility of cerebral toxoplasmosis. For example, between 3% and 15% of cases with cerebral toxoplasmosis are seronegative for T gondii IgG antibody, 9,47,61,63 and 10% to 25% of cases have a lymphocyte CD4 count >100 cells/mm3. 41,61,64
In clinical practice, severe immunocompromised PLWHA (lymphocyte CD4 count <200 cells/mm3) with compatible clinical and radiological findings of cerebral toxoplasmosis should receive antitoxoplasma therapy. Early suspicion and prompt treatment during the initial phase of cerebral toxoplasmosis reduce the risk of neurological sequelae and death. If no clinical and radiological improvement is seen within 10 to 14 days of antitoxoplasma therapy, alternative diagnoses to cerebral toxoplasmosis should be considered. 18,25,27,47,65 -67 Figure 1 shows a proposed algorithm for the management of suspected cases of cerebral toxoplasmosis in PLWHA.

Proposed algorithm for the management of suspicion cases of cerebral toxoplasmosis in people living with HIV/AIDS (PLWHA). This algorithm is meant as guidance, and individual clinical situation may render deviation from this algorithm preferable; expert opinion remains vital. 1 Up to 4 weeks of suggestive clinical manifestations of expansive brain lesions, such as headache, motor focal deficit, or altered mental status. 2 Most common patterns in brain computed tomography (CT) scan are ring-enhancing lesions with perilesional edema, nodular-enhancing lesions with perilesional edema, and nonenhancing lesions with expansive effect. Magnetic resonance imaging (MRI) should be obtained in patients with equivocal or negative CT scans. If available, MRI is the imaging modality of choice for evaluating PLWHA with expansive brain lesions. 3 Antitoxoplasma therapy is a tool for the diagnosis of expansive brain lesions in PLWHA. Therefore, close clinical follow-up is imperative. The absence of Toxoplasma gondii immunoglobulin G (IgG) antibodies and the negative polymerase chain reaction (PCR) in blood samples do not rule out the possibility of cerebral toxoplasmosis. 4 This step is very important to suspect early an alternative diagnosis to cerebral toxoplasmosis. The main issues to be evaluated are: local neuroepidemiology; degree of immunosuppression; and individual clinical, laboratorial, and neuroradiological features. 5 We have carefully evaluated whether there is a risk of cerebral herniation that may contraindicate lumbar puncture. A negative polymerase chain reaction (PCR) for T gondii in cerebrospinal fluid (CSF) does not rule out the possibility of cerebral toxoplasmosis. 6 The absence of T gondii IgG antibodies and the presence of a single lesion on MRI suggest an alternative diagnosis to cerebral toxoplasmosis and a brain biopsy is usually indicated. However, if the patient demonstrates clinical improvement, a new brain imaging can be performed with 1 to 2 weeks of antitoxoplasma therapy, and if there is radiological improvement, biopsy will not be necessary. 7 Clinical improvement usually precedes radiological improvement, but always consider the impact of corticosteroids regardless of the cause of the disease.
Diagnosis
Clinical Manifestations
Cerebral toxoplasmosis usually presents neurological subacute manifestations. However, the disease can show a rapidly progressing disease and fatal diffuse encephalitis or ventriculitis without evidence of focal brain lesions in imaging studies 7,68,69 or even a stroke-like presentation. 70
Clinical manifestations of the disease depend mainly on topography and number of lesions. The most common signs and symptoms are headache (38%-93%), focal neurological deficit (22%-80%), fever (35%-88%), mental confusion (15%-52%), seizures (19%-58%), psychomotor or behavioral changes (37%-42%), cranial nerve palsy (12%-28%), ataxia (2%-30%), and visual abnormalities (8%-19%). Patients may also present intracranial hypertension syndrome and involuntary movements. 17,25,47,61,63,67,71 Patients can present any pattern of headache with or without other manifestation. A high index of suspicion is necessary, particularly when less common and isolated nonspecific manifestations are observed (ie, hemichorea, behavioral modification). Thus, a broad spectrum of clinical manifestations is possible, and brain imaging is indicated in order to evaluate empirical therapy. 72 In the absence of treatment, progression of neurological abnormalities results in stupor, coma, and death. As expected, Glasgow coma scale ≤8 in patients with cerebral toxoplasmosis admitted at intensive care units is an independently associated variable with a poor outcome. 72 Because cerebral toxoplasmosis predominantly causes encephalitis with little or no meningeal involvement, meningismus is rare. 7
Pneumonia, chorioretinitis, and evidence of other multifocal organ system involvement can occur but are infrequently diagnosed in PLWHA. In addition, toxoplasmosis with multi-organ involvement manifesting with severe diffuse bilateral pneumonia and hemodynamic abnormalities, similar to septic shock, has been reported. These cases may or may not have concomitant cerebral toxoplamosis. 73,74 Although cerebral toxoplasmosis is the most common presentation and apparently the single clinical complication in most PLWHA, autopsy studies of patients with toxoplasmosis showed 3 scenarios: (1) patients with only cerebral toxoplasmosis (∼65%); (2) patients with cerebral toxoplasmosis and extra-CNS involvement (∼25%); and (3) patients with only extra-CNS involvement (∼10%). 75
Imaging
Magnetic resonance imaging (MRI) is the preferred modality for evaluating expansive brain lesions in PLWHA. Magnetic resonance imaging has sensitivity superior to that of CT scan for radiological diagnosis of cerebral toxoplasmosis and can impact the diagnosis and treatment of a subset of patients (Figure 2). 76,77 However, CT is the most commonly available technique in most emergency department services. In this scenario, MRI should be obtained in patients with equivocal or negative CT scans. In addition, MRI does not appear to be more specific compared to CT in the differentiation of the etiologies of expansive brain lesions in PLWHA. 62

Contrast-enhanced computed tomography (CT) scan and magnetic resonance imaging (MRI) of an HIV-infected patient with cerebral toxoplasmosis (A and B). At admission, a hypodense lesion without contrast-enhancing in the left cerebellar hemisphere (A). After 3 days, an MRI showed several ring- or heterogeneous-enhancing cerebellar lesions associated with perilesional edema. Computed tomography scan and MRI of an HIV-infected patient with cerebral toxoplasmosis (C and D). At admission, a hypodense lesion without contrast enhancing in the right cerebellar hemisphere associated with perilesional edema and deviation of the fourth ventricle (C). After 5 days, an MRI showed a ring-enhancing cerebellar lesion associated with perilesional edema and lesser deviation of the fourth ventricle (D).
The typical CT and MRI findings in patients with cerebral toxoplasmosis are multiple ring-enhancing lesions in basal ganglia (48%), frontal lobe (37%), and parietal lobe (37%) with surrounding edema. 63 In addition, occipital lobe (19%), temporal lobe (18%), and brain stem/cerebellum (5-15%) can be affected. 63,78 Approximately 30% to 40% and 15% of patients with cerebral toxoplasmosis have a single lesion seen in CT and MRI studies, respectively. 41,63,78 , Cerebral toxoplasmosis is the most frequent cause of supratentorial or infratentorial single lesion in PLWHA. In CT images, despite ring-enhancing lesions with perilesional edema being the most common pattern (44%-82%), nodular-enhancing lesions with perilesional edema (3-33%) and nonenhancing lesions with expansive effect (6%-20%) can be observed. 41,63,71,78 These radiological patterns depict high sensitivity but low specificity. Less frequent findings include diffuse cerebral edema without visible focal lesions (3%-15%) and CT without alterations but MRI demonstrating focal lesions (3%). 41,61,78,79 Hemorrhagic alterations related to cerebral toxoplasmosis have been rarely reported in CT studies but are more frequent in MRI, 80 particularly when a susceptibility-weighted imaging sequence is used. 81 In most reports, cerebral toxoplasmosis showed small isolated areas of hemorrhagic foci or within the lesions and multiple cerebral ring hemorrhagic lesions. However, multiple rounded hemorrhages associated with perilesional edema can be a unique radiological finding. 82,83 Figure 3 shows the spectrum of neuroradiological findings of cerebral toxoplasmosis in PLWHA.
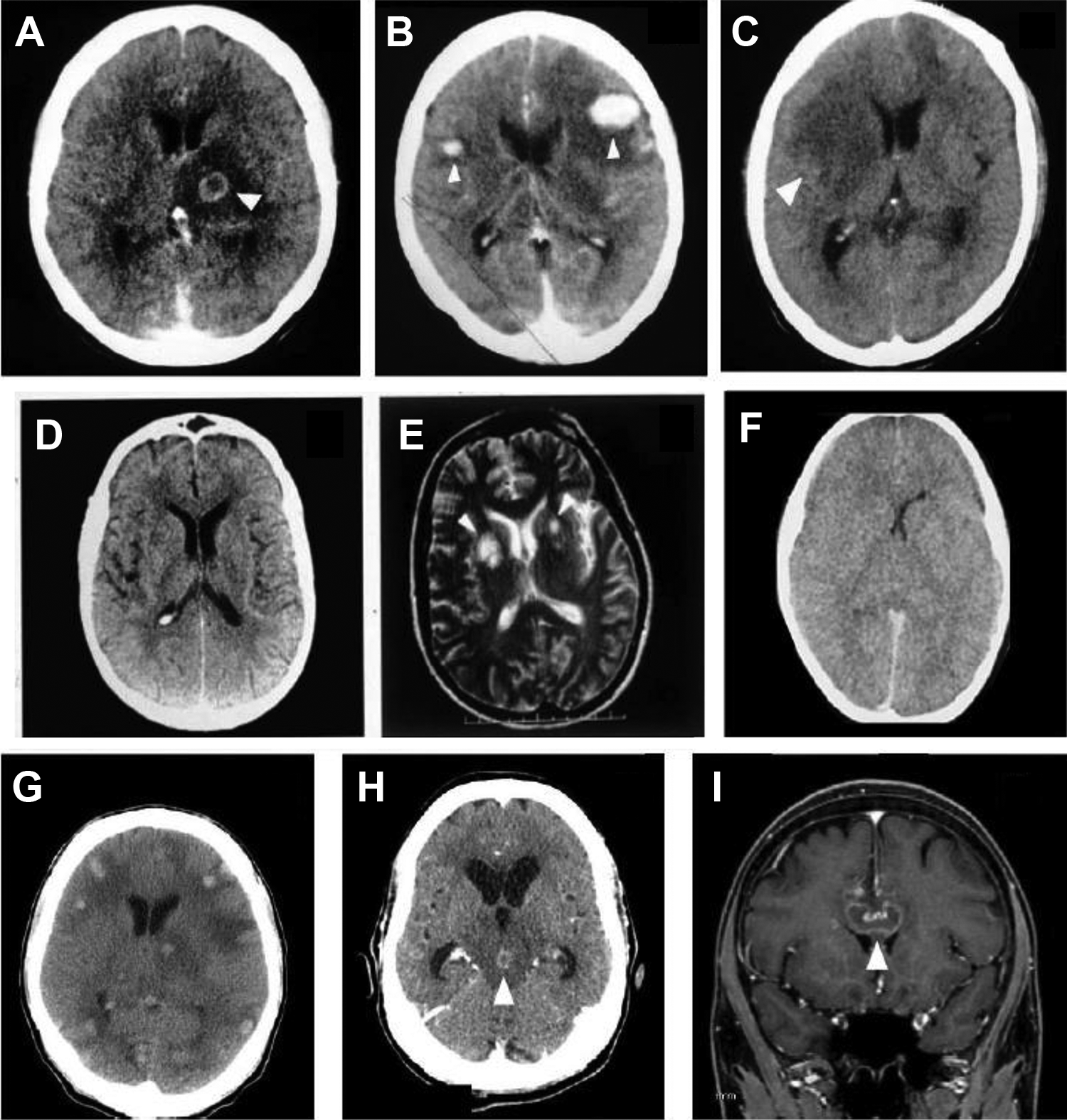
Brain computed tomography (CT) images showing the spectrum of neuroradiological findings of cerebral toxoplasmosis in people living with HIV/AIDS. Hypodense lesion with ring-enhancing and perilesional edema (A); nodular-enhancing and perilesional edema (B); expansive hypodense lesion without contrast enhancing and with mass effect (C); contrast-enhanced CT scan without abnormalities (D) and corresponding T2-weighted magnetic resonance imaging (MRI) showing multiple basal ganglia lesions, with high-intensity signals (E); contrast-enhanced CT scan showing diffuse edema (F). Non-contrast-enhanced CT scan of an HIV-infected patient showing several spontaneous hyperdense lesions associated with perilesional edema. Histopathology study confirmed the diagnosis of hemorrhagic toxoplasmosis (G). Contrast-enhanced CT scan of an HIV-infected patient showing a ring-enhancing lesion in the mesencephalon associated with perilesional edema and hydrocephalus. This lesion showed complete resolution after 4 weeks of antitoxoplasma therapy (H). Sagittal contrast-enhanced T1-weighted MRI shows a single ring-enhancing lesion crossing the corpus callosum (I). This patient underwent brain biopsy with the suspicion of primary central nervous system (CNS) lymphoma, but the histopathology study confirmed the diagnosis of cerebral toxoplasmosis. The arrows show the abnormalities.
There are 2 imaging signs with low sensitivity but high specificity for the diagnosis of cerebral toxoplasmosis in PLWHA. First, the “eccentric target sign,” a ring-shaped zone of peripheral enhancement (on postcontrast CT or T1-weighted MRI) with a small eccentric nodule along the wall, is observed in <30% of cases. 84,85 This sign needs to be differentiated from the “target sign” that has been defined as a central nidus of calcification or central enhancement surrounded by a ring of enhancement and has been considered a characteristic finding of CNS tuberculoma. 86 However, the “target signal” is rarely found in other diseases, including cerebral toxoplasmosis. 86 Second, the “concentric target sign” is a recently described MRI sign on T2-weighted imaging of cerebral toxoplasmosis with concentric alternating zones of hypo- and hyperintensities. It is believed to be more specific than the “eccentric target sign” in the diagnosis of cerebral toxoplasmosis in PLWHA. 87 Figure 4 shows examples of cerebral toxoplasmosis lesions with the “eccentric target sign,” the “concentric target sign,” and the “target sign.”

Magnetic resonance imaging (MRI) of HIV-infected patients with cerebral toxoplasmosis. T1-weighted imaging showed ring-enhancing brain lesion with a small, enhancing asymmetric nodule along the wall of the lesion (the “eccentric target sign; A). T2-weighted imaging showed a lesion with concentric alternating zones of hypo- and hyperintensities (the “concentric target sign”; B). T1-weighted imaging showed ring-enhancing brain lesion with a small, enhancing central nodule (the “target sign”; C). The arrows show the abnormalities.
Although certain imaging features favor PCNSL over cerebral toxoplasmosis (ie, single lesion, periventricular lesion, subependymal spread, and homogenous rather than ring enhancement), considerable overlap occurs. Thus, the clinical and routine radiological techniques (CT or MRI) are not sufficiently specific to reliably differentiate PCNSL from cerebral toxoplasmosis. Over the past few decades, noninvasive functional nuclear imaging modalities such as magnetic resonance spectroscopy (MRS), 201 Thallium single-photon emission computed tomography (SPECT), and positron emission tomography (PET) have been used to differentiate PCNSL from other expansive brain lesions in PLWHA, but the results are variable. A recent systematic review of MRS in the diagnosis of PCNSL (3 studies, 96 patients) shows sensitivity of 50% to 100% and specificity of 27% to 84%. In this study, meta-analysis could not be performed due to a limited number of eligible studies. 88 In this study, systematic review and meta-analysis of 26 studies evaluated the performance of SPECT (18 studies, 667 patients) in the diagnosis of PCNSL in PLWHA. The pooled sensitivity and specificity were 92% and 84%, respectively. 88 Figure 5 shows examples of MRS in cerebral toxoplasmosis and SPECT in PCNSL. Interestingly, CSF Epstein-Barr virus (EBV) polymerase chain reaction (PCR) shows sensitivity of 83% to 100% and specificity of 93% to 100% in patients with PCNSL but does not have high diagnostic accuracy to identify PCNSL. 89 Neither SPECT nor CSF EBV PCR is able to separately identify PCNSL in PLWHA. In contrast, a study evaluated the combined use of SPECT with CSF EBV PCR for the diagnosis of PCNSL in PLWHA. When the SPECT was compatible with PCNSL and CSF EBV PCR was positive, the results of sensitivity, specificity, positive predictive value, and negative predictive value were 100%, 89%, 87%, and 100%, respectively. The authors concluded that combined SPECT and CSF EBV PCR showed a very high diagnostic accuracy for PCNSL in PLWHA. 60 The systematic review of PET in the diagnosis of PCNSL (6 studies, 108 patients) showed a sensitivity of 100% and a specificity of 75% to 100% (4/6 had specificity of 100%), but meta-analysis could not be performed because no false negatives were reported for any of the 6 studies. 88 Positron emission tomography seems to be superior than isolated SPECT but has less supporting clinical data and is more expensive. 88
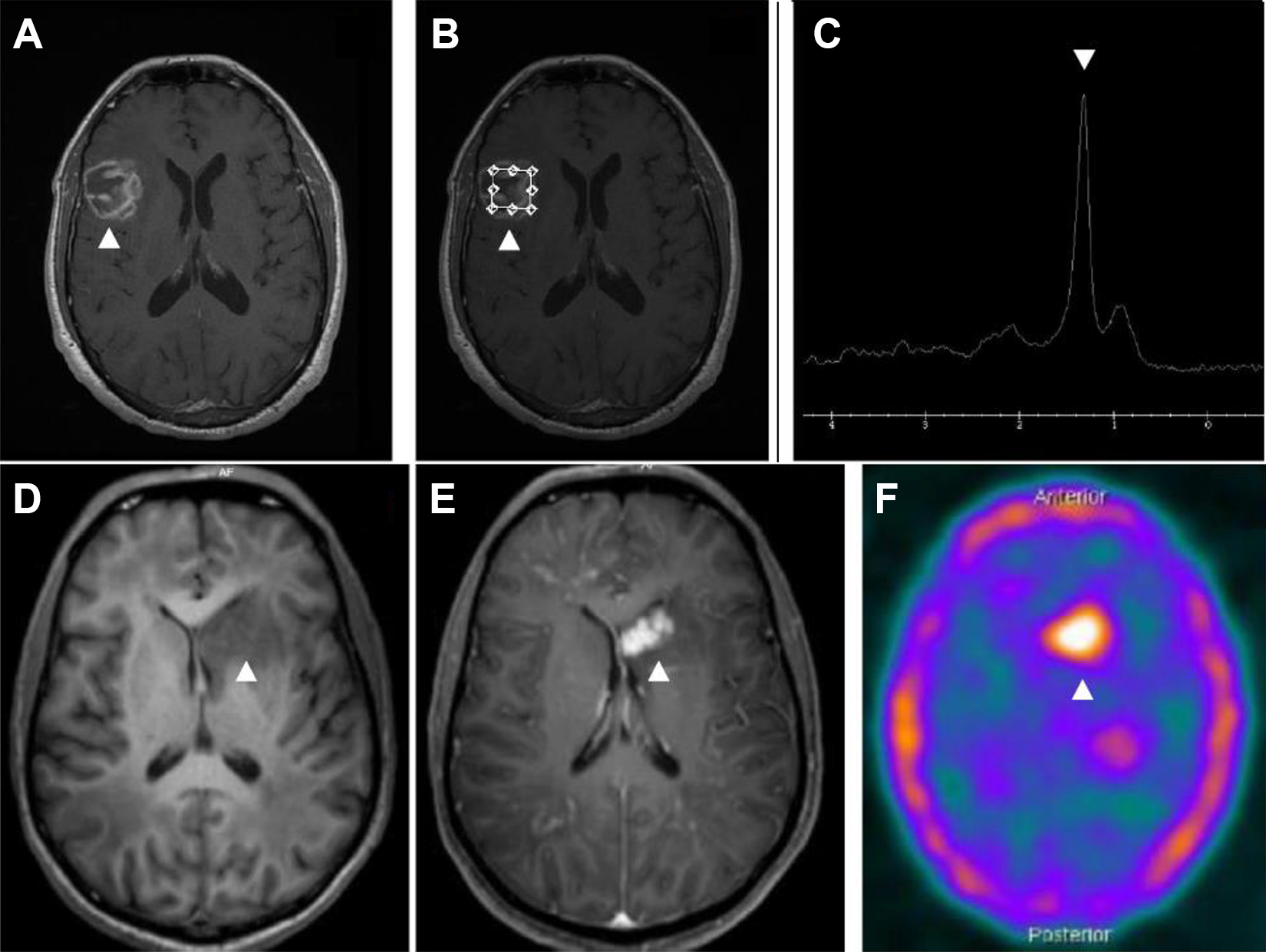
Magnetic resonance imaging (MRI) and spectroscopy of an HIV-infected patient with cerebral toxoplasmosis (A-C). Gadolinium T1-weighted imaging showing a heterogeneous ring-enhancing brain lesion in right temporoparietal region (B). Spectroscopy image showing increased lipid peak and diminution of other metabolic activity corresponding to the known lesion (C). Magnetic resonance imaging (MRI) and 18F-fluorodeoxyglucose positron emission tomography–computed tomography (18F-FDG PET-CT) image of an HIV-infected patient with histopathologically confirmed primary central nervous system lymphoma (D-F). Gadolinium T1-weighted imaging showed irregular and nodular-enhancing brain lesion in left nucleocapsular region (E). 18F-FDG PET-CT image showing foci of increased metabolic activity corresponding to the known lesion (F). The arrows show the abnormalities.
Cerebrospinal Fluid
HIV-related cerebral toxoplasmosis usually has little or no meningeal involvement. For this reason, basic CSF characteristics are usually not relevant and only subtle abnormalities such as cell count and protein values normal or mildly elevated are described. 90,91 Interestingly, eosinophils can be occasionally found in the CSF of patients with cerebral toxoplasmosis, 92 and only one case of eosinophilic meningitis has been reported. 93
Molecular Assays
The first PCR assay for T gondii detection was established 3 decades ago as an alternative to the more time-consuming and less direct procedures used at that time. 94 -96 However, the contribution of molecular techniques in the diagnosis of HIV-related cerebral toxoplasmosis is lower compared to other clinical situations caused by T gondii (ie, congenital toxoplasmosis) 52,97 or other opportunistic neurological diseases (ie, PML or CNS cytomegalovirus). 89
In patients with suspicion of cerebral toxoplasmosis, a lumbar puncture should only be performed if safe and feasible. 98 Sensitivity of detection of T gondii DNA in the CSF of PLWHA shows results between 11% and 100% (∼50%-60%), specificity of 96% to 100%, positive predictive value of 100%, and negative predictive values of 71% to 92%. 61,96,99 -109 Despite its moderate sensitivity in most studies, the high specificity and positive predictive value of PCR assay has made it a useful tool in the diagnosis of cerebral toxoplasmosis. A positive CSF T gondii PCR assay result establishes the diagnosis of cerebral toxoplasmosis, but a negative result does not exclude it. Therefore, a negative result does not contraindicate the introduction or indicate discontinuation of antitoxoplasma therapy. Antiparasitic treatment significantly reduces the sensitivity of molecular diagnosis, 100,110 and the first week is the period with the best performance. 100,111 Although there is little information about it in the literature, CSF T gondii PCR seems to be useful in monitoring treatment efficacy. 109 Simple anti-T gondii primary prophylaxis did not seem to reduce the sensitivity of PCR assay. 112
In PLWHA with expansive brain lesions that contraindicate lumbar puncture, T gondii PCR assay in blood samples may be an alternative tool. However, the DNA concentration of T gondii is very low in the blood of patients with cerebral toxoplasmosis, and this feature appears to affect the sensitivity of the test. 113 The sensitivity of T gondii PCR assay in blood samples of PLWHA shows a broad range of results between 1% and 86% (∼ 30%-50%). 96,110,113 -124 The performance of the T gondii PCR assay in blood samples of HIV-related cerebral toxoplasmosis seems to increase with the number of expansive brain lesions and particularly in the most severe forms with altered levels of consciousness. 113,123 Although controversial, some T gondii strains may have a higher capacity of dissemination in blood, which may enhance the sensitivity of PCR in this compartment. 124,125 In addition, the concomitant performance of CSF and blood sample of T gondii PCR seems to increase the individual sensitivity of each assay. 118,126
Most molecular diagnostic studies of HIV-related cerebral toxoplasmosis were conducted in the 1990s with conventional PCR (nPCR), 96,127 and this technique continues to be used as in-house assays in several laboratories. However, real-time quantitative PCR (qPCR) assay is currently the state-of-the-art molecular technique. Although nPCR and qPCR appear to show similar performances, the advantages of qPCR include rapid DNA detection, less risk of laboratory contamination with amplicons (which is an important source of false-positive reactions), robustness, reproducibility, and DNA quantification of T gondii. 128 -131 The use of commercial PCR kits appears to be an attractive approach, as they tend to be generally easy to use and standardized. 132 However, commercial PCR assays generally exhibit equivalent or inferior performances to carefully developed laboratory tests (nPCR or qPCR). 132 -134 Thus, the proficiency of the laboratory performing the molecular diagnosis and the need for optimization of PCR conditions are crucial. 135
Brain Biopsy
Histopathological diagnosis obtained by stereotactic brain biopsy is the classical and standard procedure for the etiological identification of focal brain lesions in PLWHA. 61,136 The number of biopsies declined dramatically in the cART era, 137 but this procedure still has relevant uses.
A recent meta-analysis (19 studies, 820 PLWHA underwent stereotactic brain biopsy) found a diagnostic success rate of 92%. 138 This rate for brain biopsy compares favorably to other patient populations. Another meta-analysis (26 studies, 1209 PLWHA underwent stereotactic biopsy—24 studies, open brain biopsy—1 study, or both techniques—7 studies) showed a diagnostic success rate significantly higher in the post-cART than the pre-cART era (97.5% versus 91.9%, respectively, P = .047). 139 This finding may be secondary at least in part due to improvement in surgical techniques, but probably the change in HIV-related disease epidemiology by introduction of cART is an important explanation for this difference. 139 The rates of morbidity and mortality of PLWHA who underwent stereotactic brain biopsy are 5% and 0.7%, respectively. 138 Management change was 60% and clinical improvement was 34%, presumably as a direct result for new information obtained from stereotactic brain biopsy. 138
The 3 most common diagnoses obtained from stereotactic or open brain biopsies of focal brain lesion in PLWHA are PCNSL (15%-28%), PML (21-22), and cerebral toxoplasmosis (19%-20%). 138,139
Stereotactic brain biopsy is a safe and effective way of diagnosing focal brain lesions in PLWHA and has therapeutic and clinical impact. The outcomes of brain biopsy are usually better in centers with higher technical expertise. Barriers to use of biopsy include clinical condition of the patients, topography of the lesion, its invasiveness, elevated costs, and structural requirements. 62,140
The American Academy of Neurology published guidelines for the evaluation and management of AIDS-related intracranial mass lesions in 1998, which have not been revised since then. 59 These guidelines recommend brain biopsy in adult patients having (1) large lesions with mass effect and impending brain herniation; (2) a combination of a single contrast-enhancing lesion and negative anti-T gondii IgG antibodies; (3) a cerebral lesion and increased uptake of 201 Thallium SPECT; and (4) failure to respond after 10 to 14 days of antitoxoplasma therapy, indicated by persistence or worsening of either clinical symptomatology or the mass lesions observed in CT or MRI. Nowadays, there is some disagreement about these recommendations. First, this algorithm was devised as a means to indicate the need for early biopsy in a patient most likely to have PCNSL, 141 the most common differential diagnosis of cerebral toxoplasmosis in high-income countries but not in most low- and middle-income countries. As a consequence, the elaboration of specific algorithms is necessary for the function of local neuroepidemiology and of the diagnostic tools available. Second, there is anecdotical evidence of decompressive craniectomy in HIV-related cerebral toxoplasmosis with impending brain herniation. In this situation, the postsurgical outcome seems to be almost uniformly fatal, and clinical management with neurointensive care may be a better option. Third, in settings with high prevalence of toxoplasmosis in the general population, patients with cerebral toxoplasmosis can present a single lesion and negative anti-T gondii IgG antibodies. Thus, antitoxoplasma therapy can be an initial approach in this scenario. Fourth, isolated SPECT showed lower specificity and lower positive predictive value for PCNSL diagnosis in the cART era. 88,142 However, compatible SPECT associated with positive CSF EBV PCR had excellent accuracy for PCNSL diagnosis. 60
Differential Diagnosis
Historically, the 2 leading causes of expansive focal brain lesions in high-income countries were cerebral toxoplasmosis and PCNSL. In low- and middle-income countries, tuberculomas are common and PCNSL is rarely reported. A myriad of etiologies may occasionally present with expansive brain lesions in PLWHA: Nocardia species, varicella zoster virus, Aspergillus species, Listeria monocytogenes, Treponema pallidum, Histoplasma capsulatum, and Cryptococcus neoformans. Eventually, bacterial, 52,143 mycobacterial, 144 or fungal 145 abscesses, particularly in early stages of evolution in CT scan, may be misdiagnosed as cerebral toxoplasmosis. However, neuroradiological features of brain abscess are usually well characterized, and immediate neurosurgical evaluation is imperative. 19
Although some features of lesions can suggest the presence of PCNSL (ie, a single bihemispherical lesion involving the corpus callosum) or CNS tuberculomas (ie, multiple nodular-enhancing lesions in a patient with pulmonary tuberculosis), clinical and radiological characteristics do not discriminate well enough in most cases between cerebral toxoplasmosis, PCNSL, and tuberculomas. The presence of typical and atypical presentations of cerebral toxoplasmosis is challenging, particularly in countries with a high incidence of T gondii infection. In this line, it is important to note that a common presentation of a rare disease is less likely than a rare presentation of a common disease. 146 Early initiation of “empirical” anti-T gondii therapy is an important diagnostic tool in the management of expansive brain lesions in PLWHA. Figure 1 shows a proposed algorithm for the management of suspected cases of HIV-related cerebral toxoplasmosis.
Concomitant Neurological Diseases in PLWHA
Concomitant neurological diseases in PLWHA is a challenging subject that has not been sufficiently discussed in the literature. In some reports, the frequency of coexistence of neurological diseases in PLWHA ranged from 5% to 35% in neuropathological studies 16,78,147 -152 and between 9% and 24% in clinical studies. 27,153 -156 These clinical studies were carried out in referral centers of low- and middle-income countries, had different case definitions, and the access to diagnostic tools was heterogeneous. 153 -156 It is well known that there is a dramatic decrease in the incidence of AIDS-defining neurological diseases in the cART era in middle- and high-income countries. 10,38 As expected, although information is scarce, the frequency of concomitant neurological diseases also appears to have decreased in the cART era. In a high-income country, the frequency of multiple concomitant neurological diseases due to different infectious agents and/or tumors decreased from 21% between 1984 and 1992 to 11% between 1996 and 1999. 150 In addition, 2 prospective cohort studies carried out in a referral center from São Paulo, Brazil, found similar frequencies of concomitant neurological diseases, 14% in 2007 and 15% in 2017, 157,158 showing the persistence of this problem at least in some settings. Subsets of PLWHA with prolonged and severe immunodepression (ie, late presenters, patients discontinuing cART, or drug resistance) seem to reflect a condition to concomitant neurological diseases. Spectrum of local neuroepidemiology, detailed neurological evaluation, close follow-up, and appropriate diagnostic tools seems to be other important aspects involved in the management of concomitant neurological diseases in PLWHA. This coexistence may have implications for the diagnosis, treatment, and outcome of PLWHA.
Treatment
Over the last 3 decades of the AIDS epidemic, approximately 50% to 90% of patients with cerebral toxoplasmosis demonstrate response with antitoxoplasma regimes. 3,9,41,159 -163 Nowadays, ∼80% to 90% of patients receiving antitoxoplasma therapy demonstrate clinical and radiological improvement. Case fatality rate of HIV-related cerebral toxoplasmosis significantly decreased in the cART era. For example, during hospitalization, case fatality rate varied from >90% in the pre-cART era to ∼30% in recent years in São Paulo, Brazil, and was ∼15% at a tertiary referral center in this state. 39 These different results suggest the heterogeneity of results among the several facilities. The most important outcome variables seem to be severe neurological manifestations at admission, timely diagnosis and treatment, greater experience in managing this disease, and availability of appropriate resources (eg, imaging, intensive care unit). 41,72 Nevertheless, the long-term outcome is challenging, 9,64 and the rate of neurological sequelae due to cerebral toxoplasmosis continues to be high in the cART era (∼30%-40%) 41,72 and has important impact in the quality of life of PLWHA. 64
The median time of neurological response to HIV-related cerebral toxoplasmosis is 5 days. 3 Of the patients who eventually improve, 86% show clinical improvement by day 7 of treatment and 95% show radiographic improvement by day 14 of treatment. 3,63 Figure 6 shows examples of cerebral toxoplasmosis lesions during antitoxoplasma therapy.

Magnetic resonance imaging (MRI) of an HIV-infected patient with cerebral toxoplasmosis (A-C). At admission, single lesion was observed in the left parietal lobe (A). After 2 weeks of antitoxoplasma therapy without corticosteroids, partial reduction in both size and perilesional edema was observed (B). After 6 weeks of antitoxoplasma therapy, marked decrease in lesion size and perilesional edema was seen (C). Contrast-enhanced computed tomography (CT) imaging of an HIV-infected patient with cerebral toxoplasmosis (D-F). At admission, extensive single lesion in the left basal ganglia causing brain herniation was seen (D). After 4 weeks of antitoxoplasma therapy with corticosteroids, marked reduction was observed in both size and perilesional edema (E). After 8 weeks of antitoxoplasma therapy, another CT scan showed residual alterations only (F). The arrows show the abnormalities.
Pyrimethamine plus sulfadiazine (P-S) has been used since the first described cases of cerebral toxoplasmosis in the AIDS epidemic. 6 At that time, P-S had shown to be significantly more active on T gondii than trimethoprim-sulfamethoxazole (TMP-SMX) in experimental models (in vitro and in vivo), 164 but there were no data on the use of TMP-SMX in human cerebral toxoplasmosis. In this scenario, P-S was consolidating as the preferred scheme for treating cerebral toxoplasmosis in PLWHA.
Pyrimethamine plus sulfadiazine acts synergistically by inhibiting T gondii proliferation and survival through inhibiting the folate metabolic pathway. The drugs inhibit dihydrofolate reductase and dihydropteroate synthase, respectively, and consequently block the synthesis of tetrahydrofolate, which is required by the parasite for DNA synthesis. Trimethoprim-sulfamethoxazole presents a similar mechanism of action. However, trimethoprim, unlike pyrimethamine, is a highly selective inhibitor of dihydrofolate reductase of T gondii. This feature explains the lower hematological toxicity caused by trimethoprim compared to pyrimethamine and why the use of folic acid is only necessary with the latter drug. 165 -167 Clindamycin, a lincomycin, inhibits T gondii by an unknown mechanism that involves the parasite organelle apicoplast. 168
The preferred initial therapy for cerebral toxoplasmosis in Department of Health and Human Services of the United States, 98 European AIDS Clinical Society, 169 and British HIV Association 170 guidelines is the combination of P-S. For patients with a history of sulfa allergy, sulfa desensitization should be attempted. If desensitization is not possible, pyrimethamine plus clindamycin (P-C) is the preferred alternative regimen in most guidelines 98,169,170 although it is less effective in preventing relapses compared to P-S. 159,161 Trimethoprim-sulfamethoxazole usually appears as alternative in these 3 guidelines, but other recommendations include TMP-SMX in the first-line therapies. 171 -173 In clinical practice, however, TMP-SMX is infrequently used when P-C and P-S are available. In contrast, TMP-SMX is the first choice in Africa and in other low- and middle-income countries, particularly where pyrimethamine-based regimens are not available or where there is experience with TMP-SMX.
Pyrimethamine-based regimens are beset by important limitations, including, adverse events, poor tolerability, complex posology, and the absence of parenteral formulations, a major problem in patients with alteration in mental status. 174,175 Case series and clinical trials reported toxicity led to discontinuation of pyrimethamine-based regimens in approximately one-third of patients. 63,159,161 A systematic review of adverse events associated with P-S or P-C in the treatment of toxoplasmosis (7 studies: 2 randomized clinical trials, 4 retrospective cohort studies, 1 prospective cohort study; 687 patients) reported 11% to 32% of discontinuation or change in pyrimethamine-based therapies because of adverse events. Bone marrow suppression and dermatologic complications were the most frequent adverse events. 174
Recently, a systematic review and meta-analysis of relative efficacy and safety of treatment regimens for HIV-related cerebral toxoplasmosis (9 studies: 5 randomized clinical trials, 3 retrospective cohort studies, 1 prospective cohort study; 692 patients) was performed. In comparison to P-S, treatment with P-C or TMP-SMX was associated with similar rates of partial or complete clinical response, radiological response, and drug discontinuation because of adverse events. 175 The current evidence fails to identify a superior regimen in terms of relative efficacy or safety for the treatment of cerebral toxoplasmosis. Real-world considerations are relevant when TMP-SMX is evaluated as a preferred treatment for cerebral toxoplasmosis. Potential advantages of TMP-SMX over P-S or P-C include (1) the convenience of the lower pill burden and dosing frequency and the availability of intravenous formulations; current guidelines suggest the option of intravenous TMP-SMX as initial treatment in severely ill patients 98 ; (2) the availability of several generic TMP-SMX formulations with the consequent impact on cost-effectiveness and increased accessibility; (3) prevention of Pneumocystis jirovecii pneumonia, other bacterial infections, and malaria 98,176 ; and (4) the convenience of use simplifying the early initiation of cART, which is associated with increased survival of HIV-infected patients with most opportunistic diseases.
There is no randomized clinical trial evaluating the efficacy of adjunctive steroids in HIV-related cerebral toxoplasmosis, but observational data showed no benefit with these drugs to treat cerebral edema in severe disease. 72 Despite these limitations, the recommendation is to use steroids only when cerebral toxoplasmosis lesions have significant mass effect or when diffuse brain edema is observed. 67 A suggestion can be to administer 1.5 mg/kg/d prednisone or dexamethasone equivalent for approximately 2 to 3 weeks and then steroid taper (if more than 2 weeks was used). The indiscriminate administration of steroids may result in a transient improvement in lesions of other etiologies, for example, PCNSL or tuberculomas, and complicates the evaluation of the response to anti-T. gondii treatment. Anticonvulsivants should be administered in the occurrence of seizures, but its prophylactic use should be discouraged. 67
Immune Reconstitution Inflammatory Syndrome
The spectrum of immune reconstitution inflammatory syndrome (IRIS) includes: (1) paradoxical IRIS: worsening of symptoms of a previously diagnosed opportunistic infection for which the patient is receiving treatment, and (2) unmasking IRIS: diagnosis of a new opportunistic infection with inflammatory characteristics after the initiation of cART. 177,178 Unmasking IRIS is difficult to differentiate from a classical presentation of cerebral toxoplasmosis. In paradoxical IRIS, alternative explanations for the worsening include failure of opportunistic disease treatment, failure of cART due to lack of adherence or drug resistance, and onset of other disease.
The incidence of IRIS varies with each pathogen, and its influence on the immune system is specific. Tuberculous meningitis, cryptococcal meningitis, and PML present the higher rates of CNS-related IRIS in PLWHA. 179 In contrast, T gondii is an unusual cause of IRIS probably due to the mechanisms of immune evasion by this parasite. 2,180,181 The first clinical case of cerebral toxoplasmosis–related IRIS was published in 2001, 182 and the first pathological-proven case was reported in 2009. 183 There are few case reports and 2 epidemiological studies about cerebral toxoplasmosis–related IRIS. In the first, 3 (4.6%) of 65 cases of cerebral toxoplasmosis were classified as unmasking IRIS, 184 and no cases of paradoxical IRIS were reported. In the second, 5 (3.5%) cases of paradoxical IRIS of 143 cases at risk of paradoxical IRIS were identified, and 8 (0.4%) cases of unmasking IRIS of 2228 patients who started CART while having a CD4 count <200 cells/mL were described. 185 Considering the abovementioned information, cerebral toxoplasmosis–related IRIS is rare but should be considered in the appropriate clinical and laboratory context.
No clinical trials are available on the management of IRIS-related cerebral toxoplasmosis. However, similar to other IRIS-related neurological opportunistic infections, steroids are the mainstay of therapy since they restore the blood–brain barrier, decrease T-cell activation, and prevent influx of inflammatory cells. 186 Dosage and duration of steroids are partially based on clinical experience and extrapolated from other diseases. 187 A recommendation can be (1) for mild forms of IRIS: 1 mg/kg/d prednisone (or dexamethasone equivalent) for 1 to 2 weeks; (2) for moderate forms of IRIS: 1.5 mg/kg/d prednisone (or dexamethasone equivalent) for 2 weeks followed by 2 weeks of 0.75 mg/kg/d (or dexamethasone equivalent) and then steroid taper; and (3) for severe forms of IRIS (severe edema or impending herniation): 1 g methylprednisone for 3 to 5 days followed by oral steroid taper. In patients who reside or have lived in endemic areas of Strongyloides stercoralis, empirical eradication with ivermectin before high corticosteroid regimens should be strongly considered. 178 Discontinuation of cART is not a standard approach in the management of IRIS and should be considered only in life-threatening cases or following poor response to steroids. 178
Timing of ART Initiation
A substantial reduction in risk of HIV-related cerebral toxoplasmosis was reported from the pre-cART to the cART era, demonstrating the importance of cART in the burden of this opportunistic disease. 10,64,188 -190 However, when this opportunity is lost and cerebral toxoplasmosis occurs, the next step is to decide when to start cART. There is no conclusive information regarding this issue. 191,192 A randomized controlled trial of 282 patients with opportunistic infections other than tuberculosis (∼5% with cerebral toxoplasmosis) showed that early cART (median 12 days after initiation of opportunistic infection therapy) versus deferred initiation of cART (median 45 days after initiation of opportunistic infection therapy) had significantly lower incidence of AIDS progression or death (a secondary study end point). 193 As discussed earlier, IRIS is not a major concern with cerebral toxoplasmosis, and a study demonstrated that there is no relationship between the timing of cART initiation and the occurrence of cerebral toxoplasmosis–related paradoxical IRIS. 185 In contrast to cryptococcal meningitis 194 or tuberculous meningitis, 195 many physicians would start cART within 2 weeks after the initiation of cerebral toxoplasmosis treatment. More controlled data are needed to address this controversial issue.
Pharmacologic Prophylaxis
Primary Prophylaxis
Current recommendations indicate primary prophylaxis for cerebral toxoplasmosis in Toxoplasma IgG-positive patients with lymphocyte CD4 count <100 cells/mm3 or <200 cells/mm3. 97,168 Because ∼25% of cases with cerebral toxoplasmosis occur with lymphocyte CD4 count >100 cells/mm3, in some reports, 42 <200 cells/mm3 could be a more appropriate threshold. Patients with lymphocyte CD4 count >200 cells/mm3 for >3 to 6 months in response to cART are recommended to discontinue primary prophylaxis. 169,196 -198 Patients with lymphocyte CD4 count between 100 and 200 cells/mm3 and HIV viral load below limits of detection can be considered for discontinuing primary prophylaxis. 199 The minimal period with undetectable viremia is not clear, but >3 to 6 months seems reasonable. 98 For patients with lymphocyte CD4 count between 100 and 200 cells/mm3 with HIV viral load above detection limits, primary prophylaxis should be reintroduced. 98 Daily TMP-SMX is the preferred regimen. 200 If patients cannot tolerate TMP-SMX, the alternative regimens are dapsone-pyrimethamine plus leucovorin or atovaquone with or without pyrimethamine/leucovorin. 201 -203 All these options are also effective against pneumonia for Pneumocystic jirovecii.
Secondary Prophylaxis
Because all antitoxoplasma therapies used in clinical practice are active against the tachyzoite form of T gondii, but not on the tissue cyst form, discontinuation of therapy after the induction phase of treatment usually results in recrudescence of the disease. 7 Current preferred recommendations for secondary prophylaxis of cerebral toxoplasmosis consist of a combination of pyrimethamine with sulfadiazine and leucovorin. 98 Pyrimethamine combined with clindamycin is commonly used for patients with intolerance to sulfa drugs, but this scheme does not provide protection against pneumonia due to P jirovecii. Typically, sulfadiazine should be taken every 6 hours. However, in patients with adherence difficulties, an alternative regimen includes the same daily total dose of sulfadiazine every 12 hours, 204 but the clinical experience of this scheme is limited. 205 On the other hand, a dose of 600 mg clindamycin every 8 hours is recommended because of the high failure rate observed with lower doses. 161
Similarly, with initial therapy of cerebral toxoplasmosis, TMP-SMX is an interesting alternative to secondary prophylaxis. Systematic reviews and meta-analysis of secondary prophylaxis for the prevention of HIV-related cerebral toxoplasmosis relapse using pyrimethamine-based therapy (24 studies—5 randomized clinical trials, 19 observational studies; 1596 patients) 206 and TMP-SMX (6 studies—1 randomized clinical trial, 5 observational studies; 235 patients) 207 found a similar relapse rate. Despite few studies and limited clinical experience with TMP-SMX in developed countries, this combination has been used in settings without pyrimethamine (ie, several African countries) and in some centers in Brazil where pyrimethamine is available. Interesting, a French cohort study of 83 patients with HIV-related cerebral toxoplasmosis treated with TMP-SMX reported effectiveness of 85.5%, with a relatively low incidence of side effects (22%; 7.4% requiring treatment interruption). Relapse occurred in 30% of the patients, but the most important risk factor for a new episode of cerebral toxoplasmosis was poor adherence to secondary prophylaxis with TMP-SMX. Despite this, patients with relapses received TMP-SMX, and the treatment was effective in 91% of cases. 208 The recommended dose of TMP-SMX for secondary prophylaxis is 50% of a daily initial dosage taken every 12 hours. 162,169 Patients with lymphocyte CD4 count >200 cells/mm3 for >6 months in response to cART are recommended to discontinue secondary prophylaxis. 98,169,198,209,210 Patients with lymphocyte CD4 count <200 cells/mm3 should restart secondary prophylaxis regardless of the HIV viral load. 98
Conclusion
The introduction of cART markedly decreased the incidence of cerebral toxoplasmosis in PLWHA. However, this disease remains the most common cause of expansive brain lesions and causes high morbidity and mortality in persons with advanced immunosuppression, particularly from low- and middle-income countries. Cerebral toxoplasmosis presents a wide spectrum of clinical and neuroradiological manifestations and a timely high index of suspicion is vital. Antitoxoplasma therapy is an important component of the diagnostic approach to expansive brain lesions in PLWHA. Local neuroepidemiology, the degree of immunosuppression, and individual clinical, laboratory, and neuroradiological features are important for the timely evaluation of alternative diagnoses. The use of local algorithms is important. Trimethoprim-sulfamethoxazole can be used for primary prophylaxis, initial therapy, and secondary prophylaxis of HIV-related cerebral toxoplasmosis. Currently, early initiation of cART is possible because more effective, safe, and friendly therapeutic options are available.
Footnotes
Acknowledgments
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.