
Abstract
Kenya is one of 22 countries globally that account for 90% of all HIV-positive pregnant women. This study aimed to determine factors affecting uptake of prevention of mother-to-child transmission (PMTCT) services among HIV-positive pregnant women at Lodwar County Referral Hospital in Turkana County, an arid area in northern Kenya. We conducted a retrospective review of HIV-positive pregnant women attending antenatal care (ANC) and accessing PMTCT services between January 2015 and December 2016. We used infant prophylaxis as a proxy measure of PMTCT uptake, and records across programs were linked using the mother’s unique medical identification number. A total of 230 participants were included in the study. Bivariate analyses showed maternal prophylaxis (odds ratio [OR] = 45.71; 95% confidence interval [CI]: 10.35-202.00), residing in urban center (OR = 2.64, 95% CI: 1.45-4.81), and having at least one ANC visit (OR = 2.78; 95% CI: 1.25-6.17) were significantly associated with uptake of PMTCT.
What Do We Already Know About This Topic?
We know that in rural areas such as Turkana County, distance to health facilities impacts uptake of multiple health services, including HIV-related services.
How Does Your Research Contribute to the Field?
There is very little information available about the HIV epidemic and programmatic outcomes in this region; thus, this article presents an important contribution to the literature.
What Are Your Research’s Implications toward Theory, Practice, or Policy?
Retention along the PMTCT cascade is a critical indicator of success for national PMTCT programs and one of the most challenging aspects for delivery of care in local, rural, and far-flung locations like Lodwar. This study identified factors that impact PMTCT uptake and retention in care in a marginalized county of Kenya.
Introduction
Globally, mother-to-child transmission (MTCT) of HIV accounts for >90% of all new pediatric HIV infections and may occur during pregnancy, labor, and delivery or breastfeeding. 1 In the absence of appropriate interventions, rates of MTCT can be as high as 25% to 35%. Effective prevention of MTCT (PMTCT) programs can reduce MTCT to as low as 1%. 2 However, achieving lower rates of MTCT has been challenging in sub-Saharan Africa, where PMTCT service coverage remains <50%, and Kenya is one of the 22 countries that accounts for 90% of all HIV-pregnant women worldwide. 1 Kenya introduced updated PMTCT guidelines in 2012, which are putatively in practice at all public and private health facilities throughout the country. 3
In Kenya, most pregnant women (94%) attend an antenatal care (ANC) clinic at least once during their pregnancy and receive routine opt-out HIV testing and counseling. 2 Furthermore, Kenya PMTCT services referred only 56% of HIV-positive pregnant women to HIV treatment programs, which is reflected in the national MTCT rate of 8.5%. 2 HIV prevalence among pregnant women in Turkana County is 9.9%, and the MTCT rate is 9%. The MTCT rate for Turkana Central Subcounty is 1.6 times greater than the county rate at 14.5%. 2 We conducted this study in Turkana Central Subcounty at Lodwar County Referral Hospital (LCRH) to determine the factors affecting PMTCT uptake among pregnant HIV-positive women. The facility serves urban, rural, and refugee populations within the subcounty. The LCRH is one of only 2 referral hospitals in the entire county (Figure 1).

Map highlighting location of Lodwar, Turkana County, Kenya.
Methods
We conducted a retrospective review of the records of all HIV-positive pregnant women in the LCRH’s ANC, antiretroviral therapy (ART), and HIV-exposed infants (HEI) registries for calendar years 2015 and 2016. Descriptive and associative statistics were calculated with MS Excel and OpenEpi software. Using infant prophylaxis as our dependent variable and residence, ANC visit, and maternal prophylaxis as independent variables, we conducted bivariate and logistic regression analyses and calculated odds ratios (ORs) and 95% confidence intervals (95% CIs).
Ethical Approval and Informed Consent
Our study did not require ethical board approval because it did not contain human or animal trials and no contact with patients.
Results
Descriptive Statistics
A total of 230 pregnant women were included in the analyses, with a mean age of 26 ± 5.7 years, 215 (95%) were married, 113 (49.6%) were newly diagnosed with HIV, 200 (88.9%) were placed on maternal prophylaxis, and 153 (67.1%) were from the urban center (Table 1). Of the 224 infants born to the women in our study, only 161 (71.9%) were put on prophylaxis (Table 1). Most (176 [76.7%]) of the women in our study received prophylaxis during their first ANC visit. Regarding place of delivery, 78 (33.9%) of the women (40.0%) delivered at hospital, and most of those (63 [81.0%]) were ≤30 years old. Of the 223 male partners who accompanied the women to their first ANC visit, only 1 (0.5%) consented to HIV testing.
Demographic Data of, and PMTCT Utilization among, HIV-Positive Pregnant Women, LCRH, 2015 to 2016.a
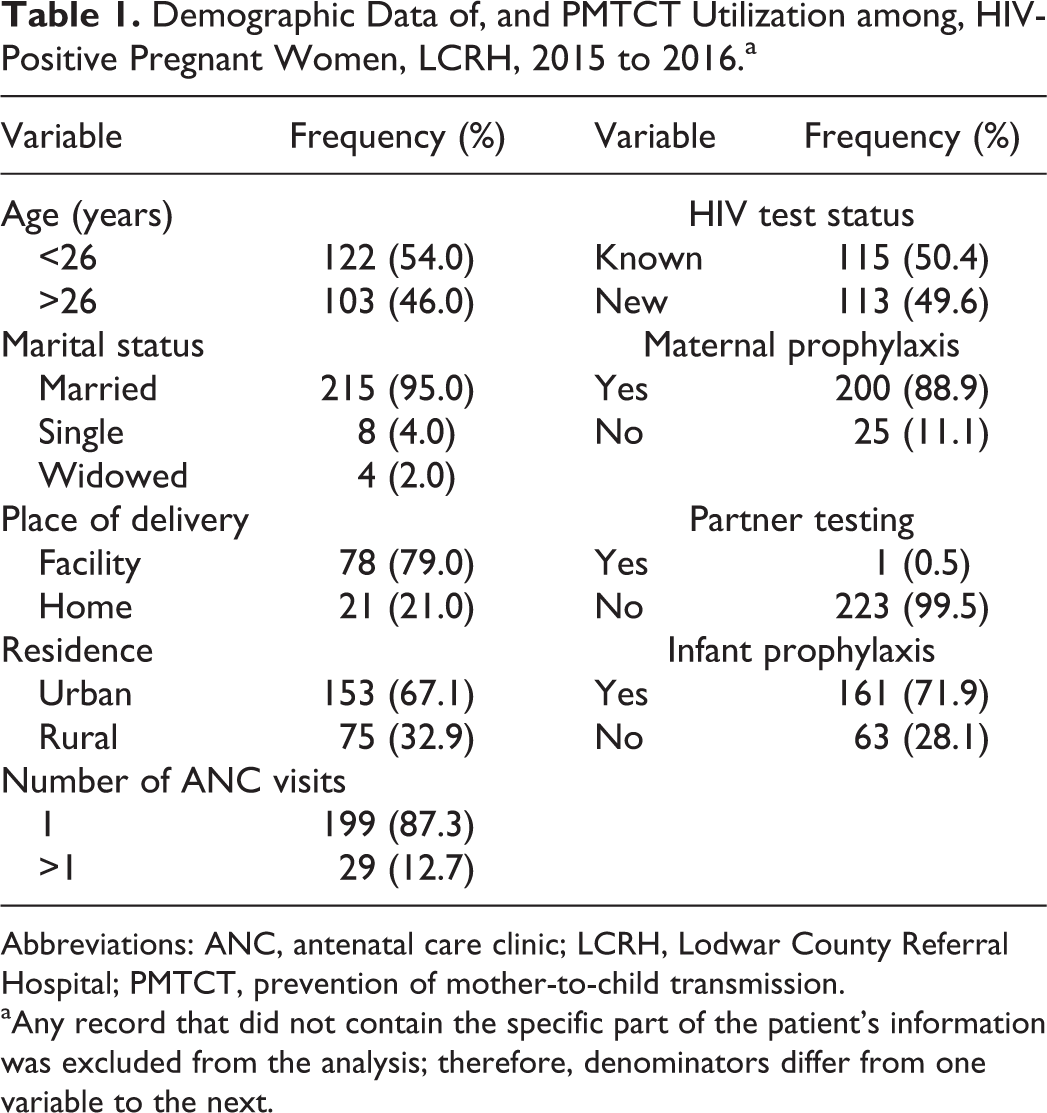
Abbreviations: ANC, antenatal care clinic; LCRH, Lodwar County Referral Hospital; PMTCT, prevention of mother-to-child transmission.
aAny record that did not contain the specific part of the patient’s information was excluded from the analysis; therefore, denominators differ from one variable to the next.
Bivariate Analyses
Maternal prophylaxis (OR = 45.7, 95% CI: 10.4-202.0), urban residence (OR = 2.6, 95% CI: 1.5-4.8), and attending at least one ANC visit (OR = 2.8, 95% CI: 1.3-6.2) were all significantly associated with infant prophylaxis (Table 2).
Bivariate and Logistic Regression Analyses Results, PMTCT Uptake among HIV-Positive Pregnant Women, LCRH, 2015 to 2016.

Abbreviations: ANC, antenatal care clinic; CI, confidence interval; LCRH, Lodwar County Referral Hospital; PMTCT, prevention of mother-to-child transmission.
Logistic Regression
Cox and Snell R 2 analyses showed that maternal prophylaxis explained 25.4% of the variation in infant prophylaxis. At least one ANC visit explained 3.0% of variation in infant prophylaxis, and urban residence explained 4.3% of variation in infant prophylaxis (Table 2).
Discussion
This investigation reveals factors that impact uptake of PMTCT services in a low-resource setting like Turkana County. Most clients in our study were young and married, showing results similar to other studies throughout 6 Sub-Saharan Africa (SSA) countries that marital status and age are not significant factors in determining uptake of PMTCT services. 4
Place of residence was a strong predictor of infant prophylaxis. Most clients enrolled were from the urban center compared to their rural counterparts. This finding is likely a function of distance to the health facility. Multiple studies show that in rural settings, HIV-positive pregnant women live far away from the health facilities that provide PMTCT services, thus limiting uptake of those very same services. 5
Our results showed that even just one ANC visit had an impact on infant prophylaxis and facility-based deliveries, which is consistent with studies in Zimbabwe and Nyanza Province counties in Kenya. 6,7 However, the number of deliveries conducted by a skilled health-care provider was low in our study group. The findings were similar to a study in rural Nyanza region of Kenya, and results showed that most clients did not access skilled delivery services. 7 Maternal prophylaxis was a major determinant of infant prophylaxis in our study, with results showing that clients who had prophylaxis were more likely to enroll their newborns on prophylaxis as compared to the ones who did not receive maternal prophylaxis. The findings were similar to a study done in Johannesburg, South Africa, where maternal prophylaxis was also a factor in infant prophylaxis enrollment. 8
The low uptake of HIV testing by the pregnant women’s male partners was an element of concern in our study. Findings from our study showed that only 1 of 223 of the male partners had HIV testing. This could affect utilization of PMTCT services in our setup given how important it is to involve male partners. Men have a significant influence on uptake of reproductive health services and other interventions. Multiple studies throughout SSA show that supportive male partner involvement in reproductive health issues plays a key role in improving reproductive health outcomes. 9,10 For our study, we think the low uptake of partner testing is due to the makeup of the population in Lodwar (pastoralist, immigrant, and transient). Our hypotheses are supported by other studies in Uganda, Kenya, and Ethiopia. 11 -13
This study was limited by the lack of access to more demographic data on the HIV-positive pregnant women. The analyses could have benefited from inclusion of level of education, parity, and birth order, which are factors proved to be important factors in other studies. 14,15 These data were often unavailable due to incomplete registry entries and poor data quality at the county’s health facilities. 16 Underlying reasons around poor male involvement in a setting such as Turkana County should be explored further. 17 We also recommend interventions to improve (1) clinical and community efforts to encourage hospital deliveries, (2) efforts to sensitize HIV-positive pregnant women from rural areas on the importance of PMTCT services, and (3) outreach and education efforts targeting the male partners of these women. 16,17 In conclusion, county HIV programs should develop strategies that promote consistency and adherence to PMTCT protocols related to integration in rural, low-resource settings such as Turkana County.
Footnotes
Acknowledgements
The authors thank the Ministry of Health, Turkana County, staff at Lodwar County Referral Hospital, and the Kenya Field Epidemiology & Laboratory Training Program for operational support during this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.