
Abstract
Thirty-day hospital readmissions, a key quality metric, are common among people living with HIV. We assessed perceived causes of 30-day readmissions, factors associated with preventability, and strategies to reduce preventable readmissions and improve continuity of care for HIV-positive individuals. Patient, provider, and staff perspectives toward 30-day readmissions were evaluated in semistructured interviews (n = 86) conducted in triads (HIV-positive patient, medical provider, and case manager) recruited from an inpatient safety net hospital. Iterative analysis included both deductive and inductive themes. Key findings include the following: (1) The 30-day metric should be adjusted for safety net institutions and patients with AIDS; (2) Participants disagreed about preventability, especially regarding patient-level factors; (3) Various stakeholders proposed readmission reduction strategies that spanned the inpatient to outpatient care continuum. Based on these diverse perspectives, we outline multiple interventions, from teach-back patient education to postdischarge home visits, which could substantially decrease hospital readmissions in this underserved population.
Introduction
Thirty-day hospital readmissions (repeat hospital admission within 30 days of discharge) constitute an important health care quality metric because they may signal adverse patient outcomes and negatively impact quality of life of patients. Moreover, they increase costs for patients, hospitals, and insurers. 1 Under the Hospital Readmissions Reduction Program of 2012, administered under the Affordable Care Act, the Center for Medicare and Medicaid Services reduces payments to hospitals with excess 30-day readmissions. 2 As a result, hospitals are now financially incentivized to identify and reduce 30-day readmissions. However, safety net hospitals encounter unique challenges in caring for disproportionately uninsured patients who often have poorer health status and fewer economic and social resources. 3 -6 Additionally, safety net hospitals themselves have fewer resources with which to serve high-need patients, contributing to higher 30-day readmission rates among safety net hospitals compared with institutions serving commercially insured populations. 7 -9 As a result, stakeholders continue to debate how to apply quality metrics equitably to diverse populations. 10,11
Patients with HIV and patients receiving care in safety-net hospitals have high rates of 30-day readmissions, many of which are potentially preventable. This study examines the perspectives of patients, their medical providers and hospital staff on the key factors that cause readmissions in HIV patients, the preventability of readmissions and how best to avoid unnecessary readmissions in this population. This research identifies the need to adjust the 30-day readmission quality metric for social determinants of health and provides a practical toolkit of strategies to reduce avoidable readmissions.What Do We Already Know about This Topic?
How Does Your Research Contribute to the Field?
What Are Your Research's Implications toward Theory, Practice, or Policy?
Studies investigating readmissions have identified several factors associated with overall 30-day hospital readmissions at the system level (eg, lack of care coordination, premature discharge), provider level (eg, inadequate discharge instructions, missed diagnoses), and patient level (eg, nonadherence to medication and follow-up). 12 -15 While 30-day readmissions have been studied in various high-risk patient populations, including chronically ill patients, 16 elderly patients, 17 postsurgical patients, 18,19 and patients with congestive heart failure 20 and chronic obstructive pulmonary disease, 21 relatively few have focused on patients with HIV. Studies report hospital readmission rates among HIV-positive populations between 19% and 25%, which is 1.5 times greater than among HIV-negative populations, even after adjusting for age, gender, race, insurance status, or diagnostic category. 1,22,23 This suggests that additional factors, including socioeconomic factors, mental illness, substance use, 1 social support, and stigma, 24,25 are likely contributing to readmissions in this population and merit further study.
Regardless of patient characteristics, hospitals should not be penalized for readmissions that are not preventable. However, preventability has proved challenging to define and measure and may need to be adjusted given diverse hospital settings and populations. In the general population, a wide range (5%-79%) of 30-day readmissions is estimated to be potentially preventable. 26 Among studies that have incorporated survey data from patients and providers, one US health system study determined that 48% of 537 medical readmissions were potentially preventable, 13 whereas a multicenter European study found that only 14% of 1398 readmissions were potentially preventable. 27 In a previous analysis of 130 HIV-positive individuals, we found that nearly 50% of readmissions could have been prevented. 23 Examining factors that contribute to readmissions among patients with HIV admitted to safety net hospitals may help refine readmission metrics for both HIV-positive patients and other vulnerable populations and may indicate avenues for intervention.
Improving the equitable application of the 30-day readmission quality metric requires a better understanding of how readmissions occur and how stakeholders define preventability. Although large administrative data sets have been used to identify potentially preventable readmissions, 26,28 analyses have not uniformly incorporated data on patient demographics, community resources, or hospital infrastructure, limiting their relevance to safety net populations and institutions. While analyses based on billing codes may provide a global view of readmission trends, they cannot assess circumstances that may be driving readmissions, nor can they reveal strategies for reducing them. Therefore, we designed a qualitative study conducting semistructured interviews with patients, their medical providers, and hospital staff to solicit perspectives toward causes of readmissions, the nature of preventability, and specific strategies for reducing preventable readmissions to improve outcomes for HIV-positive individuals.
Methods
We conducted semistructured interviews in triads composed of an HIV-positive patient readmitted within 30 days of a previous hospital admission, plus 2 individuals: medical providers or staff. Provider and staff participants were eligible if they had met with the patient and were responsible for the patient’s care on either the index admission and/or readmission. In addition, we purposively sampled 3 long-time clinicians in HIV care who were not linked to a specific patient to obtain data from both inpatient and outpatient experiences and their perspective on the posthospital discharge care transition.
Data Collection
Patients were recruited from the electronic health record (EHR) HIV inpatient census for a large urban safety net health system. Investigators approached patients in their rooms to participate in a brief survey and interview, lasting an estimated 45 to 60 minutes, in either English or Spanish. Participants could elect to have caregivers or other persons present. Subsequently, we invited providers and/or staff members involved in the patient’s care. Providers included hospitalists (“primary team providers”) and infectious disease consults (“HIV providers”); staff were case managers and transitional care nurses. While we attempted recruitment of triads for all patients, in 4 of 29 cases, we were successful in completing only 1 provider or staff interview (ie, a dyad).
Patient interview domains included reflections on recent hospital admissions, outpatient self-care and care-seeking behaviors, medication access and adherence, perspectives on readmission preventability, experiences with HIV, other medical problems (eg, substance use, mental health), and nonmedical problems (eg, housing, social support, stigma). Provider and staff interview domains included perceptions of admission preventability, communication among patients, providers and staff, role of HIV diagnosis in readmissions, and perspectives regarding the 30-day readmission quality metric.
Three members of the research team (A.E.N., R.T.H., E.G.M.) with academic and field training in qualitative methods conducted data collection and analysis. We collected data in an iterative design to continually assess thematic content for saturation and patterns of emergent findings. Following the initial 17 interview triads, we determined that we had achieved thematic saturation among hospital staff. For triads 18 to 29, we recruited 2 physicians, ideally 1 primary team provider and 1 HIV provider. We also refined the provider interview guide to prioritize domains of inquiry that aligned with study objectives: factors related to readmission in safety net hospitals, unique medical and social factors for patients with HIV, and strategies for reducing preventable 30-day readmissions.
Data Analysis
Each interview was audio-recorded, transcribed, and assigned a participant ID indicating role (eg, HIV provider) and time of care (index or readmission). Data were analyzed using NVivo 9.0 (QSR Australia). The initial codebook used a deductive schema that corresponded to semistructured interview guide domains. Three research team members trained in qualitative methods independently coded 14 (16%) transcripts. They met after every 2 coded interviews to discuss, refine codebook definitions, add emergent codes, and resolve discrepancies by consensus. The team used a matrix to assign 2 coders to the remaining 38 (64%) transcripts. Interviews were selected for coding based on interviewer notes regarding substantive responses. The team reviewed all coded transcripts to assess themes and interpret findings. Coding concluded once thematic saturation was reached. Two team members then reviewed and selected representative quotes.
Ethical Approval and Informed Consent
Patient participants provided informed written consent prior to enrollment in our study, and nonpatient participants provided verbal consent that was audio-recorded prior to participation in accordance with our protocol approved by the medical center’s institutional review board (STU 042015-032) and safety net health system.
Results
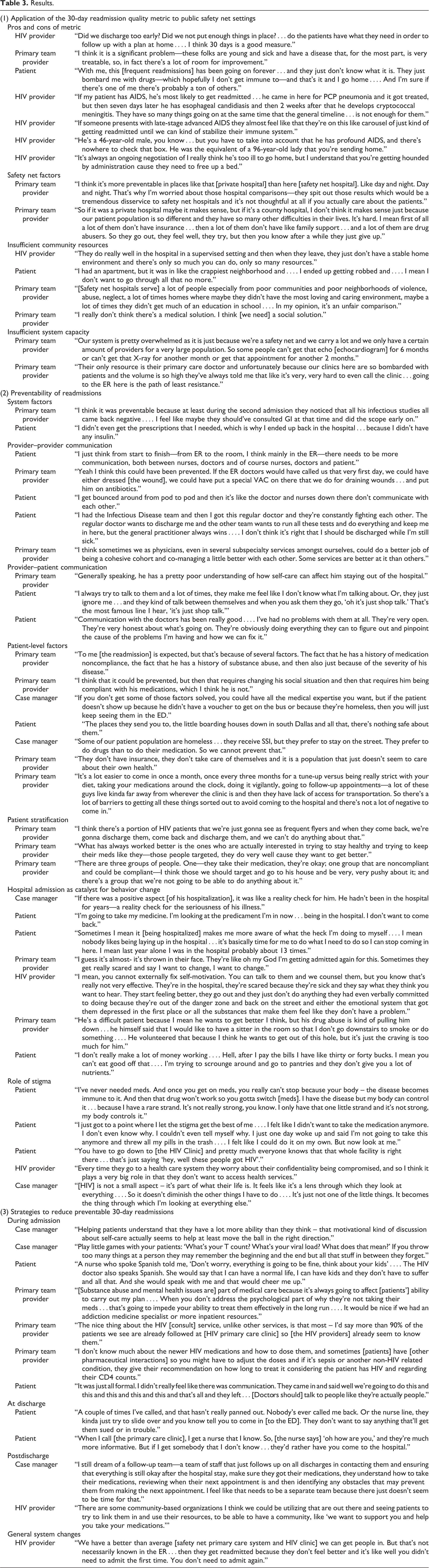
We conducted 86 total interviews: 29 patient interviews, 38 provider interviews, and 19 staff interviews; demographic characteristics are presented in Tables 1 and 2. All 29 patient interviews were unique individuals. Of the 36 unique providers, 8 were infectious diseases specialists (attending physicians or fellows) and 28 were inpatient primary team providers (attending physicians, residents, or hospitalists). For 25 of 29 patients, we completed triad interviews (patient, provider, and staff or patient and 2 providers); for 4 patients, only 1 provider was available to participate in an interview. Table 2 shows provider and staff participants by timing of reference event. Table 3 includes participant quotes that informed our results, with suggested strategies for reducing readmissions organized in Table 4.
Patient Participant Characteristics.a,b

Abbreviations: IDU, injection drug user; MSM, men who have sex with men; NH, New Hampshire.
a N = 29.
b Source for all data is patient electronic health record (her), except for language, which is listed by patient preference.
c IDU trumps other categories if more than one risk factor.
Provider (n = 38) and Staff (n = 19) Participant Characteristics.

Results.
Strategies to Reduce Preventable 30-Day Readmissions.a
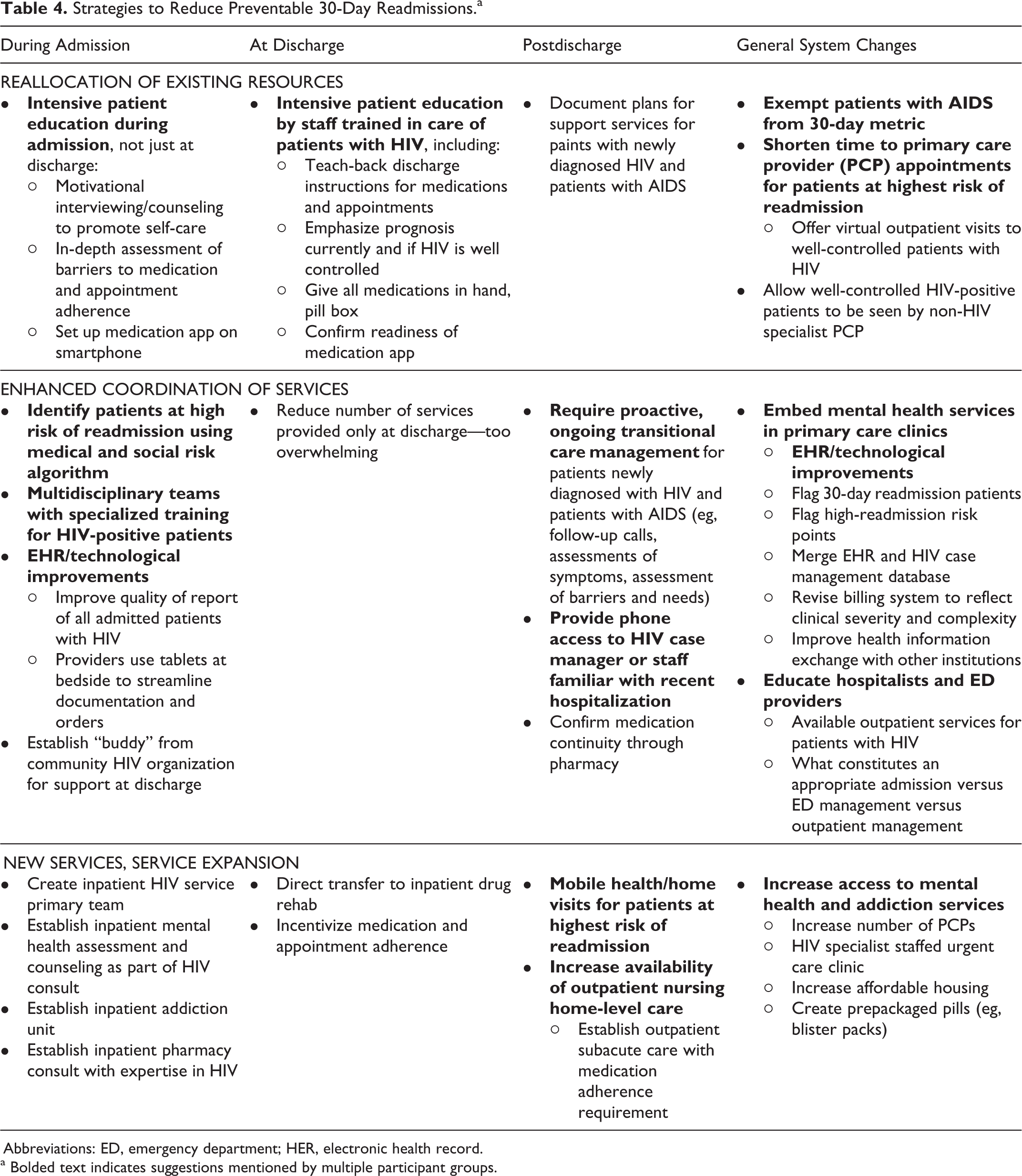
Abbreviations: ED, emergency department; HER, electronic health record.
a Bolded text indicates suggestions mentioned by multiple participant groups.
Application of the 30-Day Readmission Quality Metric to Public Safety Net Settings
Pros and Cons of Metric
Providers and staff participants highlighted both positive and negative implications of the 30-day readmission metric. Some felt that implementing the metric revealed gaps in services and highlighted the need for additional resources, such as increasing substance use and mental health services for patients with HIV. Others noted that measuring readmissions has encouraged existing quality improvement efforts, such as improved patient education at discharge, review of medications, and the assessment of home resources. However, most provider and staff participants felt that the 30-day readmission metric inadequately adjusted for patients with HIV or for safety net institutions, given the greater proportion of patients with severe medical (eg, AIDS-related illnesses) and psychosocial (eg, homelessness, lack of social support, addiction) needs.
Medical Factors
From a medical standpoint, providers noted that HIV-positive patients, particularly those with advanced disease, often had an erratic clinical course resulting in recurring readmissions, as if on a “carousel.” A 30-day window was not sufficient for immune recovery in patients with advanced HIV, despite appropriate therapy. Similarly, other hospital policies, such as a clinical stability checklist prior to discharge, may not apply to this population. Immunosuppression may belie illness severity, resulting in premature hospital discharge and predisposing to readmission. Patients with AIDS, due to their younger age and lack of immune response, may look well enough for discharge even when they are clinically very fragile. “He’s a 46-year-old male…but you have to take into account that he has profound AIDS…. He was the equivalent of a 96-year-old lady that you’re sending home” (HIV provider).
Safety Net Factors
In addition to these medical considerations for patients with HIV, many providers and staff felt it was unfair to compare socially vulnerable safety net hospital patients to commercially insured populations served by other hospitals. “It’s like day and night…[the comparison] does a tremendous disservice to safetynet hospitals.” Specific sociobehavioral and socioeconomic factors, such as substance use, lack of social support, lack of health insurance, poverty, and homelessness, were cited by both providers and patients as contributing to readmissions. One primary team member described the social isolation of one patient: “no family member, no close relatives, nobody care[s] about them…lonely and homeless, no money.” Lack of social and financial support among safety net patients may impact their ability to care for themselves, engage in outpatient care, and avoid unnecessary readmissions.
Insufficient Community Resources
Providers also felt that there were insufficient resources to care for socially vulnerable individuals after discharge. The environment and local communities in which people live were cited as contributors to readmissions in safety net populations. Patients noted that a lack of safe, affordable housing (“I had an apartment but it was in…the crappiest neighborhood”) posed a significant barrier to care. Existing community services, such as a local counseling center that also provides linkage to housing, were praised, but these services do not meet the level of need. Given the substantial barriers faced by safety net patients, providers suggest that reducing 30-day readmissions and improving outcomes in safety net populations require more than a medical intervention and needed to incorporate “a social solution.”
Insufficient System Capacity
In addition to limited community resources, the safety net hospital system has insufficient capacity to provide outpatient medical care required for this population. Providers cited the overburdened outpatient system (“our clinics are bombarded with patients”), which leads to more emergency department (ED) visits (“the path of least resistance”), and due to concerns about adequate follow-up or the need to expedite a time-sensitive evaluation, results in unnecessary admissions and readmissions.
Preventability of Readmissions
Overall, providers and staff generally shared the perspective that factors over which they had some control (eg, care transition procedures, communication) were more preventable than other factors, such as patient-level behavior change (eg, medication adherence, dietary restriction) and stigma, which providers and staff had less ability or resources to influence.
System Factors
Several participants identified system-level issues, such as delays in inpatient diagnostic workups, interruptions in medications at discharge, and limited ability to directly transfer patients to other facilities, as contributors to preventable readmissions. Other examples include inadequate resources to meet the high demand for specialists and timely follow-up with primary care providers, restrictive voucher systems for providing free medications at the time of discharge, and limited availability of services such as substance use disorder treatment for uninsured patients.
Provider–Provider Communication
Patients and providers also largely agreed on provider-level issues contributing to preventable readmissions, such as inadequate communication among providers at various transitions during the patient’s admission. In a busy ED, it may be more time efficient for the doctor to admit a patient to the hospital than to contact a specialist who may be able to intervene in the ED and prevent a readmission. The ED is often the first phase of a hospital admission and can be a chaotic first step in the inpatient care continuum. One patient reported feeling “bounced around” from location to location within the ED, with insufficient communication between staff and providers.
Once admitted to the hospital, handoffs and transitions among care teams and staff were associated with incomplete transfer of information. Specifically, shift providers sometimes lacked detailed knowledge of the patient’s clinical and social circumstances including HIV disclosure status, resulting in interruptions in the treatment plan and inadequate discharge planning. Communication between primary team providers and HIV consult providers was also a point of conflict and inefficiency, “my regular doctor wants to discharge me and the other team wants to run all these tests” [patient].
Provider–Patient Communication
Several participants described ineffective education about prognosis, medications, and postdischarge self-care tasks. A patient with newly diagnosed cirrhosis who had been readmitted with fluid retention felt that doctors didn’t explain he was not supposed to drink too much water. The provider taking care of this patient acknowledged that the patient “has a pretty poor understanding of how self-care can affect him staying out of the hospital.” Similarly, a patient described how doctors ignored him during interactions with each other and feeling dismissed when a doctor told him, “oh it’s just shop talk.”
Patient-Level Factors
Unlike system- and provider-level factors in preventable readmissions, participants generally did not agree on the preventability of readmissions due to patient-level factors, such as medication adherence, substance use, or social circumstances such as lack of housing or transportation. Participants also differed on the modifiability of these factors. For example, one primary team provider felt the readmission was “expected…because of several factors…medication noncompliance…history of substance abuse, and…the severity of his disease.” Another primary team provider, speaking about a different patient, identified similar barriers but felt the readmission “could be prevented, but then that requires changing his social situation.”
While some placed the responsibility squarely on the patients, others suggested that additional resources to promote medication adherence, self-efficacy, and social support services after discharge would improve outcomes. Per one case manager, “They receive supplemental security income/disability (SSI), but they prefer to stay on the street. They prefer to do drugs than to do their medication. So we cannot prevent that.” In contrast, another case manager stated, “if you don’t get some of those factors solved, you could have all the medical expertise you want, but…you will just keep seeing them in the ED.”
Patient Stratification
Patient characterizations by providers often took the form of strict categories (eg, adherent or not, socially stable or not, HIV-related admission or not). Certain primary team providers who stratified patients by perceived risk for readmission felt that resources should only be directed at patients who were motivated to get well and not spent on those who they labeled “beyond the fix of any physician.” Most providers who labeled patients spoke in binary terms; however, one provider identified a third category of patients “who are noncompliant and could be compliant…those we should target and go to [their] house and be very, very pushy about it.”
Hospital Admission as Catalyst for Behavior Change
Many patients and providers identified hospitalization as an inflection point in the patient’s health trajectory. Patients who may have been in denial of their illness or the progression of their disease may be forced to consider the consequences of not regularly attending medical visits or taking medications, a “reality check,” as one case manager described it. Hospitalization itself served as a potential catalyst for behavioral change for patients who did not like being hospitalized and became motivated to not be readmitted.
Nonetheless, numerous providers recognized that stating a desire to change behaviors did not necessarily lead to behavior change; many other factors—relationships, mental illness, and substance use—constitute ongoing obstacles, particularly among safety net patients. One primary team provider identified that even patients who may be motivated to change behaviors were overwhelmed by the tasks required to maintain their health, stating “they don’t have…the executive function to be able to comply with all these rules to take care of themselves.” Patients found that despite a desire to change unhealthy habits, they may not be able to implement these changes due to inadequate access to needed services, such as eating a healthy diet. “After I pay the bills I have like 30 or 40 bucks. I mean you can’t eat good off that.”
Role of Stigma
The stigma surrounding HIV and denial of disease was frequently cited by patients and providers as contributing to readmissions. One patient with advanced AIDS voiced inaccurate beliefs about the nature of HIV and treatment, convinced that she had a “rare strand” of the disease that was keeping her from becoming ill. Some patients recognized the role of stigma and denial in their worsening clinical status resulting in hospitalization. One patient said, “let stigma get the best of me” when he threw all his medication in the trash. Beyond medication adherence, stigma may also impact patients’ willingness to engage in care; some are reluctant to attend clinic visits or go to the hospital for fear of being recognized as an HIV-positive person. “Pretty much everyone knows that that whole facility is right there…that’s just saying ‘hey, well these people got HIV.’”
Strategies to Reduce Preventable 30-Day Readmissions
Here, we present principal thematic findings at various stages of care: during admission, at discharge, postdischarge, and suggestions regarding overall system-level changes (ie, not related to a discrete phase of care). In addition, Table 4 summarizes all suggestions made by participants, highlighting in bold strategies mentioned by multiple participant groups and categorized by level of resources required to implement them.
During Admission
Providers, staff, and patients all recommended enhanced patient education during the hospital admission: education about the relationship of HIV to other medical problems using “teach-back” strategies, motivational interviewing to enhance medication adherence, and in-depth assessments about individual barriers. Moreover, participants felt that repeated, engaging education sessions, rather than a single episode at discharge, were key to advancing patients’ knowledge and motivation to adhere to vital self-care tasks (such as healthy eating and infection prevention measures).
As part of more patient-centered education, some providers and staff described a desire to help patients put their HIV disease in context, that is, although HIV is a chronic condition, it doesn’t have to be a terminal illness. One of the case managers stated, instead of HIV being “a lens through which they look at everything,” more individualized patient education might be able to help patients “get to a place where it becomes one of the smaller things that I’m working on in my life and it’s not everything.” It’s also important that patient-centered education be delivered in the patient’s language. One Spanish-speaking patient, newly diagnosed with HIV, shared that her Spanish-speaking doctor explained to her “that I can have a normal life, I can have kids…and that would cheer me up.”
Several hospitalist providers talked about the value of the multidisciplinary HIV service with medical specialists, nurses, and case managers trained and experienced in caring for patients with HIV. Some HIV providers felt that the HIV team should be the primary inpatient team, rather than serving as consultants, given their clinical expertise and familiarity with patients, and that this would mirror the existing outpatient care model where HIV providers serve as both specialist and primary care provider. Several patients expressed greater comfort interacting with the inpatient HIV team, whom they felt were more sympathetic and personal in tone and behavior than non-HIV providers. “[Doctor’s should] talk to people like they’re actually people.” HIV providers also suggested physically “cohorting” infectious disease patients on one floor of the hospital to promote multidisciplinary communication and coordination of patient care.
At Discharge
Many participants suggested enhanced patient education throughout the patient’s admission. Providers (primary team and HIV), case managers, and patients stressed the importance of medication education by staff trained in HIV-related care, rather than the floor’s general “discharge nurse.” Providers and case managers further recommended that patients receive all medications in-hand before they leave the hospital. Other strategies included providing patients with pill boxes and teaching patients how to download and use mobile phone medication management apps. Patients suggested that, instead of including a general phone line on discharge paperwork, patients receive the number of a case manager or hospital staff familiar with their recent hospitalization to ensure more individualized advice. One patient described how, when calling the nurse line after discharge, they will just “tell you to come in [to the ED].”
Postdischarge
Patients, hospital staff, and providers felt strongly that a posthospitalization follow-up team dedicated to HIV-positive patients would reduce preventable readmissions. Such a team would contact patients postdischarge to review their symptoms, ensure that they received their medications, understand how to take medications, provide appointment reminders, and proactively identify potential obstacles to outpatient care. Some further recommended a mobile team that could conduct home visits for patients at highest risk of readmission. Other noteworthy suggestions included embedding mental health and addiction medicine services in all HIV primary care clinics, shortening time to follow-up with outpatient providers, and increasing partnerships with community-based organizations to enhance patients’ support system.
General System Changes
Overall, patient and provider suggestions for general system changes to reduce preventable readmissions focused on increasing patient-centered services at various points in the continuum of care. Many of the proposed system-level changes address challenges that are inherent in the resource-limited safety net system. Multiple strategies were offered at the primary care level: (1) increase the number of providers to address lack of timely access to outpatient appointments, (2) increase the number of virtual visits (ie, telephone appointments) for well-controlled HIV-positive patients to free up outpatient appointment times for postdischarge and poorly controlled patients, and (3) establish a noninfectious disease primary care option for well-controlled HIV-positive patients.
Some providers and staff offered EHR-based strategies to identify and streamline care for complex patients: (1) merge case management data with EHR data, making important social factors more accessible to providers; (2) flag patients who are at high risk for readmission in the EHR; and (3) improve communication of EHR data across other hospital systems.
Many providers felt that inappropriate admissions from the ED contributed to higher readmission rates among people with HIV. They suggested that ED providers be educated about resources available to HIV-positive patients, what constitutes an appropriate admission, and when HIV status is a relevant factor in decisions about admission.
Discussion
Our interviews with patients, medical providers, and staff yielded novel findings pertaining to (1) stakeholders’ perceptions of 30-day readmissions as a quality metric in patients with HIV and in safety net hospitals, (2) preventability of readmissions in patients with HIV, and (3) strategies to reduce readmissions. Overall, participants felt that 30-day readmissions could be a reasonable quality metric because it promotes care optimization for a vulnerable population but was inappropriate for patients with AIDS-defining illnesses due to the severity and unpredictability of their disease. Interviewees felt that applying a universal metric to a socioeconomically disadvantaged, medically needy population from an underresourced community who access care in an overburdened system is unfair and inequitable.
Regarding preventability, although many agreed on modifiable system- and provider-level factors (ensuring medication availability and interprovider communication), participants disagreed about whether patient-level behavioral factors (medication adherence, diet, abstinence from drugs and alcohol) were modifiable and the extent of the health care system’s role in reinforcing positive health behaviors. Many providers stratified patients by risk for readmission based on their perceptions and patients’ expressed desire for behavior change; some felt that admissions themselves were an essential moment to catalyze change. Overall, the majority of participants recognized multiple challenges and the need for additional community resources (social support, home health care, substance use treatment) to effect meaningful change in reducing preventable readmissions.
Both patients and providers identified multiple strategies for reducing readmissions among patients with HIV, ranging from reallocating existing resources (eg, intensive patient education by HIV staff), enhancing coordination of existing services (eg, providing a contact familiar with a patient’s hospitalization for postdischarge communication), and service expansion (eg, inpatient addiction team). Few suggestions focused on the discharge phase, which is an important finding given that most studies implement interventions at this time point. This further emphasizes the need for multimodal, multitemporal strategies along the inpatient-to-outpatient care continuum. Our study results provide a practical toolkit for hospitals aiming to improve outcomes along this care continuum, which can be implemented with varying levels of available resources.
Findings also indicate that patients with HIV warrant particular attention due to stigma and the need for a specialized approach to provide comprehensive care. Stigma plays a significant role in medication adherence and utilization of inpatient and outpatient services. 29,30 Patients who experience stigma often present with more advanced stages of HIV disease and related complications, contributing to both admissions and readmissions. 31 Adjusting to an HIV diagnosis and accepting that it is a chronic, manageable disease is critical to improving patient outcomes. These findings underscore the need for adopting a more patient-centered approach that employs a multidisciplinary care team composed of medical providers and case managers specifically trained in the health and emotional challenges patients with HIV face.
Taken together, our findings confirm and extend the literature on 30-day readmissions among HIV-positive patients. Like other studies, we identified multiple factors related to 30-day readmissions in people with HIV, including medical severity and socioeconomic and behavioral variables. 1,32 Our data support prior quantitative findings that safety net hospitals have higher readmission rates, 33 that current methods do not adequately account for this variability, 33 and that unadjusted readmission measures would disproportionately penalize safety net hospitals. 34 The main area of disagreement among participants involved determinations of preventability among patients who lacked the motivation and/or resources to avoid hospital readmission. Provider categorizations of patient engagement and openness toward intervention support a readmission reduction strategy of patient risk stratification to match resources to level of need 35,36 and consider individual context. 37 Many participants offered intervention strategies supported by the literature: improved identification of high-risk patients, 38,39 nurse- or social worker–driven patient navigation and care coordination, 40,41 use of multidisciplinary care teams, 36,42,43 differentiated care, 44 enhanced medication counseling by pharmacists or other inpatient staff, 45,46 and postdischarge calls or home visits. 47,48 Participants also highlight the inpatient stay as an opportune “teachable moment” for enhancing patient activation and engagement. 49,50 Participants also advocated routine and comprehensive attention to substance use and mental illness in both inpatient and outpatient settings. 51 -53
Our study is not without limitations. We conducted interviews in a single, large integrated county system, which may limit generalizability. However, given disproportionate rates of HIV incidence in the South and in large urban centers, and higher rates of uncontrolled HIV in Southern states, 54 our findings may inform other organizations caring for similarly affected populations. We were unable to interview patients who were cognitively impaired or too ill to participate; this may have limited our study’s assessment of patients who rely on caregivers.
Conclusion
We present results of a large qualitative study of diverse participants about 30-day hospital readmissions among HIV-positive patients. Our study confirms quantitative findings from the general and HIV readmissions literature and provides nuanced information about the contribution of social determinants of health. Participants supported the idea of measuring readmissions as a quality indicator but highlighted concerns about comparing readmissions among HIV-positive patients in safety net hospitals to other settings and patient groups. Our findings also underscore the challenge of identifying preventable causes of readmissions, particularly patient-level factors and HIV-related stigma. Participants supported the need to identify high-risk patients with modifiable barriers to care and develop patient-centered interventions that match patients’ risk for readmission. Our findings contribute a toolbox of practical strategies for reducing avoidable readmissions at different stages of care and varying levels of available resources.
Footnotes
Authors’ Note
This is the authors’ original work; they own the rights. This manuscript is not under consideration by any other journal at this time. This manuscript has not already been published. The authors have obtained and can supply all necessary permissions for the reproduction and copyright works not owned by them (not applicable). All authors meet all required conditions of authorship under the International Committee of Medical Journal Editors (ICMJE) guidelines. All procedures were performed in accordance with our protocol approved by the UT Southwestern Medical Center’s institutional review board (STU 042015-032) and Parkland Health & Hospital System, and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by National Institutes of Health (NIH) (1K23AI112477; Nijhawan); Agency for Healthcare Research and Quality (AHRQ) (R24 HS022418 to the UT Southwestern Medical Center, Center for Patient-Centered Outcomes Research); NIH/NIDA (T32DA013911; Tiruneh); NIH (P30AI042853 to the Providence/Boston Center for AIDS Research; Tiruneh); and NIH/NIMH (R25MH083620; Tiruneh).