
Abstract
Background:
There are few validated tools to measure adherence for children living with HIV. We identified questionnaire items for caregivers of Kenyan children aged <15 years living with HIV.
Methods:
Caregiver–child dyads were followed for 6 months. At monthly visits, the child’s HIV provider administered a 10-item questionnaire to the caregiver. Children were given electronic dose monitors (Medication Event Monitoring Systems [MEMS]). Correlation between questionnaire items and dichotomized MEMS adherence (≥90% doses taken versus <90%) was investigated using logistic regression models.
Results:
In 95 caregiver–child dyads, mean age of children (40% female) was 8.3 years. Items associated with higher odds of MEMS adherence in multivariable analysis included the father giving the child medication, being enrolled in a nutrition program, and the caregiver reporting no difficulties giving the child medication.
Conclusion:
Providers typically ask about missed doses, but asking about caregiver responsibilities and difficulties in giving the child medication may better detect suboptimal adherence.
What Do We Already Know about This Topic?
Adherence monitoring is an essential component of comprehensive HIV care and management, yet there are few low-cost, validated instruments to measure adherence for children and adolescents living with HIV in sub-Saharan Africa.
How Does Your Research Contribute to the Field?
We tested the validity of a short 10-item adherence questionnaire administered to children’s caregivers in western Kenya and showed that the instrument could be used by HIV providers as a screening tool for nonadherence among children living with HIV and on treatment.
What Are Your Research’s Implications toward Theory, Practice, or Policy?
Our research supports the feasibility of validated, low-cost, and routine adherence monitoring tools such as brief questionnaires for children living with HIV and on treatment as part of comprehensive HIV care and management.
Introduction
Despite significant progress in the prevention of mother-to-child transmission, there are an estimated 1.8 million children younger than 15 years living with human immunodeficiency virus (HIV), including an estimated 150 000 newly infected children in 2015. 1 Moreover, only 49% of children in need of antiretroviral therapy (ART) had access to it. 1 For those children accessing life-saving ART, consistent and long-term adherence is required to reduce morbidity and mortality and to prevent drug resistance. 2 –5 High levels of adherence to therapy are even more important for the vast majority of children living with HIV in resource-poor settings where access to second- and third-line regimens is still limited. 6,7 Children in these settings face multiple and complex barriers to access and adherence to treatment, and there are few data to inform evidence-based interventions. 8
There is no gold standard for clinical evaluation of adherence to ART. 9 Estimates of ART adherence among children are hampered by heterogeneous and untested measures. 10,11 The reliability of caregiver-reported missed doses, one of the most commonly employed adherence measures, has been evaluated in the United States 12,13 and in several sub-Saharan African countries 14 –16 and suggests that caregivers may overestimate adherence compared to other measures like pill counts, pharmacy refill, and electronic adherence monitoring (EAM), but most studies do not report on validity testing of the measure. A validated caregiver-reported adherence tool by the NIAID Pediatric Clinical Trials Group demonstrated high correlation with virologic outcomes among children in the United States, 17 but how this measure performs in resource-limited settings is unclear.
Access to accurate and low-cost tools to routinely measure adherence to ART among children living with HIV is critical to guide clinical decision-making, reduce the risk of drug resistance, and evaluate adherence interventions. 18 Previously, we examined 48 adherence questionnaire items using EAM as our external criterion for adherence among caregivers of HIV-infected children in care at clinics of the Academic Model Providing Access to Healthcare (AMPATH) in western Kenya. 19 Using the adherence items that were most associated with EAM to create a 10-item questionnaire, in this study, we test the reliability and validity of the shortened adherence measure among a new cohort of children living with HIV and on ART in Kenya.
Methods
Study Design
We conducted a multistage validation study using prospective cohorts of Kenyan children living with HIV to evaluate the performance of questionnaire items to estimate ART adherence. During a previous stage, we created 48 pediatric ART adherence questionnaire items informed by literature review, expert panel consultation, and formal qualitative work including individual and group cognitive assessments of questionnaire items in this setting in western Kenya. 20,21 These adherence items, which included questions related to missed doses, doses taken by visual analog scale, adherence barriers, and other social factors such as poverty and HIV stigma, were translated into Kiswahili, one of the national languages of Kenya, with good understandability and face validity. 20 We tested the 48 items among 200 caregiver–child dyads, who were prospectively followed for 6 months with the adherence items being administered to the caregiver at monthly visits, as well as to children who were responsible for their own medication-taking (48-item adherence questionnaire included in Online Appendix). 19 Participants kept their ART in bottles containing Medication Event Monitoring Systems (MEMS; MWV/AARDEX Ltd, Seraign, Belgium, Switzerland) caps that have a microcircuit that records the time and date of bottle opening and shows good correlation with virologic outcomes. 22,23 Using a novel variable selection strategy called least absolute shrinkage and selection operator with logistic regression, we identified the adherence items best correlated with MEMS adherence. 19
In this study, we conducted a prospective assessment of the 10 best–performing adherence items from our previous study. We followed 107 caregiver–child dyads for 6 months to test the reliability and validity of the 10-item adherence questionnaire to measure children’s adherence to ART. The questionnaire was administered to caregivers at baseline and monthly visits (a total of 7 times) in Kiswahili or English (dependent on caregiver’s preference) by their child’s regular clinician (physician or clinical officer) as part of their routine monthly clinical exams. A child version of the questionnaire was also administered to children if they or their caregiver reported that the child had responsibility for their own medication-taking; however, low response rate and other difficulties precluded robust analysis (see “Discussion” section). In addition, we administered the original 48-item questionnaire (inclusive of the 10 best–performing items that are tested in this study) to caregivers at baseline, month 3, and month 6. This was done to allow comparison of caregiver responses to the same 10 adherence items at these time points based on 2 key differences: (1) a different format (ie, longer form versus shorter form) and (2) by who was administering the questionnaire (clinician or research assistant). As done in the previous study, 19 the longer 48-item questionnaire was administered to the caregiver by research personnel immediately after the child’s visit with the physician.
Participants were issued MEMS monitoring devices and instructed in their care and use during the follow-up period, with study personnel downloading and inspecting the MEMS at monthly study visits. Children had blood samples taken at month 3 and month 6 of the study to evaluate immunological status (CD4 counts and percentages).
Study Setting
This study took place at AMPATH—a large HIV treatment program in western Kenya. 24,25 The AMPATH is a partnership between Moi University School of Medicine, Moi Teaching and Referral Hospital (MTRH), and a consortium of North American academic medical centers led by Indiana University School of Medicine. The AMPATH provides free ART (first- and second-line ART regimens only), primary care services, and psychosocial and nutritional support for children and adults at over 50 health clinics in western Kenya. This study recruited participants from AMPATH’s clinic at MTRH, one of the largest referral hospitals in Kenya located in the city of Eldoret in Uasin Gishu County, Rift Valley Province.
Study Participants
Inclusion criteria for children were HIV infected, between 0 and 14 years of age, on a first-line ART regimen, and enrolled in care at AMPATH. Children’s current adherence level was not considered in their inclusion in the study—that is, we wanted to recruit children with a range of adherence levels to test the reliability and validity of the questionnaire. Caregivers were biological or nonbiological caregivers who accompanied the child to clinic, were knowledgeable about the child’s medical needs, and had at least some responsibility for administering or supervising their child’s medication-taking. The same caregiver was encouraged to come to all of the child’s study visits during the follow-up period, but we did not exclude different caregivers from completing the adherence questionnaire. Participants were recruited using convenience sampling; eligible caregiver–child dyads were identified by clinic and research personnel and referred to the study team for participation. Informed consent was obtained from all caregivers for their own and their child’s participation in the study. Assent was obtained for all children aged 10 years and older, consistent with AMPATH research protocols. A small incentive (<US$3) was provided to study participants to cover their transportation costs and time.
Data Analysis
Basic demographics are presented with means (standard deviations [SD]) for continuous variables and frequencies (percentages) for categorical variables. Demographic variables were compared by adherence groups using Student t tests and Fisher exact tests, due to low cell counts, respectively.
Electronic adherence outcomes were dichotomized as ≥90% of doses taken on schedule (defined as “adherent”) or <90% for analysis (defined as “nonadherent”). Dichotomized adherence at 90% cutoff was used alongside sensitivity analyses for a number of reasons. Continuous adherence data were highly skewed, with a prevalent ceiling effect due to children clustering around the maximal level of 100% adherence. A 90% cutoff point was chosen as it has been used in similar studies 26,27 and because of its clinical relevance; studies show that adherence rates <90% are associated with increased risk for virologic failure and drug resistance. 28 –30 Demographic and clinical characteristics of study participants were summarized by dichotomized MEMS adherence level. Individual items in caregiver questionnaire were then screened by bivariate logistic regression models of the dichotomized MEMS adherence outcome. Items associated with the adherence at P <.05 were selected for the multivariable logistic regression models. In all these analyses, within-subject correlations among repeated measures were accommodated by generalized estimating equations; odds ratios (ORs) and 95% confidence intervals (95% CIs) are reported, with an OR >1.00 indicating a higher odds of MEMS adherence.
Selected caregiver items were then used to form an adherence barrier scale. We assessed the classification accuracy of the scale using Cox-Snell R 2 values. These were calculated at both visits 3 and 6, as well as both visits combined. To increase the robustness of the analysis, sensitivity analyses were conducted at different MEMS adherence cutoff points at 80% and 95% adherence levels. 31 Statistical analyses were performed using R 3.0.1 (Vienna, Austria) and SAS v9.4 (SAS Institute, Cary, North Carolina). P values less than .05 are considered statistically significant.
Research Ethics and Informed Consent
This study was approved by the institutional review board at Indiana University School of Medicine in Indianapolis, Indiana (IRB study number: 0904-67) and by the Institutional Research and Ethics Committee at Moi University School of Medicine in Eldoret, Kenya (IREC study number: 2009/61).
Results
Participant Characteristics
We recruited 107 caregiver–child dyads, of which 95 attended all study evaluations and had complete adherence and clinical data. Of these 95 caregiver–child dyads, mean age of children was 8.32 years (SD: 3.27) and 40.4% were female (Table 1). From baseline, the child’s most recent mean CD4 percentage (CD4%) was 27.76 (SD: 10.16) and the majority of children had advanced clinical disease (67% of children were diagnosed at World Health Organization stage 3 or 4 disease). A small minority of children (14%) knew their HIV status. There were no significant differences in child characteristics in the adherent (MEMS ≥90% doses taken) compared to the nonadherent group (MEMS <90% doses taken). On average, nonadherent children were on ART for longer duration (6.7 years compared to 3.6 years), but this was not statistically significant (P = .08). The majority of caregivers who participated in the study were the biological mother of the child (59%), while an uncle, aunt, or cousin was the second most common type of caregiver (15%). The biological mother was also the one most often responsible for giving the child his or her medicines (55%), although 17% also reported that the child is responsible for his or her own medication-taking.
Caregiver–Child Dyad Characteristics by MEMS Adherent Group at Baseline Visit.

Abbreviations: AMPATH, Academic Model Providing Access to Healthcare; ART, antiretroviral therapy; MEMS, Medication Event Monitoring Systems; WHO, World Health Organization.
Adherence by MEMS increased significantly over the duration of the study; at month 1, mean and median adherence by MEMS was 83% and 94%, respectively, while by month 6, this had increased to 91% and 96%, respectively (P = .005). The increase in adherence over time was more marked in the group of patients with <90% MEMS, as illustrated in Figure 1. Still, when MEMS adherence was calculated over the course of the study, just over half of participants (52%) achieved ≥90% of doses taken.
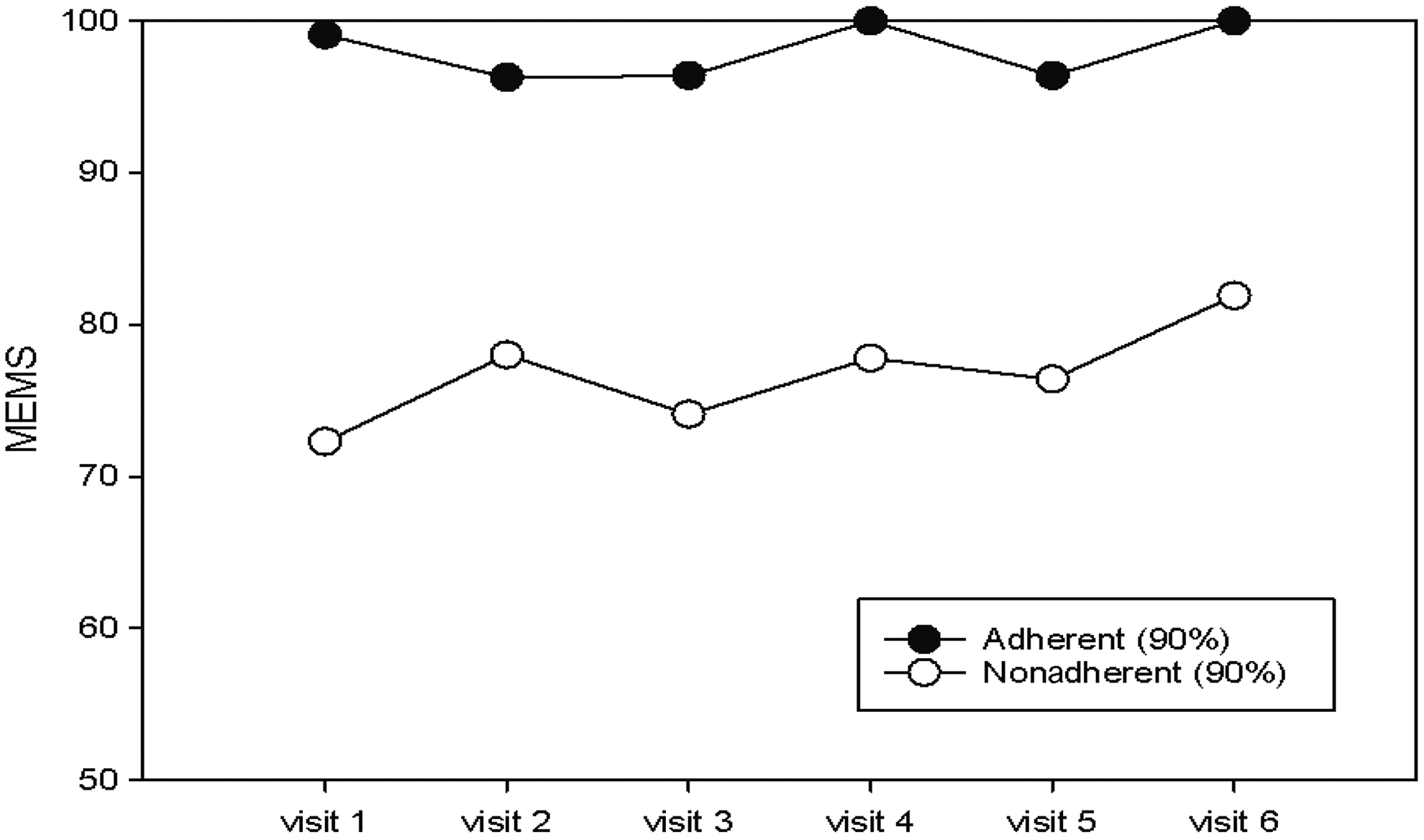
Adherence by Medication Event Monitoring Systems (MEMS).
Validation Testing of Questionnaire
The short-form adherence questionnaire performed well. Intraclass correlation coefficient analysis showed that the intraclass correlations were similar between the short-form adherence questionnaire items used in this study and the long-form adherence questionnaire tested previously, indicating no significant loss of information. Intraclass correlations were 0.316 at 3 months and 0.322 at 6 months, with overlapping CIs. Cox-Snell R 2 values were also similar (visit 3: 0.037 versus 0.005; visit 6: 0.020 versus 0.011; both: 0.002 versus 0.008, for short form versus long form, respectively). Likelihood ratio tests indicate the values are not significantly different when comparing the short form to the long form.
In bivariate analysis, most of the questionnaire items were significantly associated with dichotomized MEMS adherence including items directly related to missed doses and problems with adherence as well as items related to the type of caregiver and who was responsible for giving the child his or her medication (Table 2). In subanalyses, we found that items performed similarly well between children who received ART from their mother versus those who received ART from a different caregiver. In children who received ART from their mothers, reporting the child was disclosed to was significantly associated with a lower odds of MEMS adherence (OR: 0.66, 95% CI: 0.59-0.73), while in children who received ART from someone other than their mothers, it was nonsignificantly associated with a higher odds of MEMS adherence (OR: 1.32, 95% CI: 0.91-1.92).
Unadjusted Associations between Questionnaire Items and Medication Adherence Measured by MEMS.

Abbreviations: AMPATH, Academic Model Providing Access to Healthcare; ART, antiretroviral therapy; CI, confidence interval; MEMS, Medication Event Monitoring Systems; OR, odds ratio.
In multivariate analysis, the biological father (OR: 1.4, 95% CI: 1.2-1.7) or a nonbiological family member (OR: 1.3, 95% CI: 1.2-1.5) being responsible for giving the child ART were both significantly associated with high odds of being in the MEMS adherent group (Table 3). Being enrolled in the AMPATH nutrition program was also associated with higher odds of being in the MEMS adherent group (OR: 1.3, 95% CI: 1.0-1.6). Finally, the caregiver reporting problems getting the child to take ART (OR: 0.7, 95% CI: 0.6-0.8) and reporting problems giving ART on time (OR: 0.9, 95% CI: 0.8-1.0) were associated with lower odds of being in the MEMS adherent group. While the caregivers reporting that the child took a dose more than 1 hour late (P = .0002) and that the child missed at least 1 dose in the past 7 days (P = .0078) were significant in bivariate analysis, late and missed doses in the past 7 days did not remain significant in the multivariate model.
Adjusted Associations between Questionnaire Items and Medication Adherence Measured by MEMS.

Abbreviations: AMPATH, Academic Model Providing Access to Healthcare; ART, antiretroviral therapy; CI, confidence interval; MEMS, Medication Event Monitoring Systems; OR, odds ratio.
Discussion
The 10-item adherence questionnaire administered to caregivers of children living with HIV performed well when validated against EAM. Of the 10 questionnaire items, 7 were significantly associated with dichotomized MEMS adherence in bivariate analysis, while 4 of these items remained statistically significant in multivariate analysis. While low-cost and routine adherence monitoring has been highlighted as a critically important part of comprehensive HIV care, there have been few studies that have rigorously validated adherence questionnaire items in low-income settings, particularly for children living with HIV. This study adds to the limited research base and offers a set of potential adherence questionnaire items to be evaluated in other resource-limited settings. We are currently evaluating the performance of this 10-item adherence questionnaire at an additional site in western Kenya, as well as at sites in South Africa and Thailand.
As in previous work, 19 we found that a broad range of questionnaire items were associated with children’s adherence. While most routine self-reported adherence assessment items ask about missed doses during a specific period (eg, in the past 3, 7, or 30 days), 10 our analysis showed that questions other than missed doses may be a better indication of potential problems with adherence, particularly for assessing the adherence of children living with HIV who are often not responsible for their own medication-taking. This includes questions related to who in the household is responsible for giving the child ART. Our findings indicated that when the child’s father or nonbiological caregiver was responsible for giving the child ART, the child was more likely to have MEMS adherence ≥90%. We also found that when a child’s mother was responsible for giving the child ART, the child knowing his or her HIV status was significantly associated with lower odds of MEMS adherence ≥90%, but for a child who was given ART by any other type of caregiver or responsible for their own medication-taking, knowing his or her HIV status was associated with higher odds of MEMS adherence ≥90%, although this was not statistically significant. Qualitative inquiry in this setting will shed light on why caregiver type impacts children’s adherence in western Kenya; however, for clinicians and other providers, the important finding here is that questions related to the caregiver should be part of the adherence assessment. In previous work, we found that if a child’s primary caregiver was employed outside the house, the child was more likely to have poorer adherence, further suggesting caregiver-related dynamics in adherence behaviors for HIV-infected children. 31
In addition, we found that questions related to general problems with giving a child ART and problems related to medication timing were more likely to be associated with suboptimal adherence by electronic monitoring versus questions directly related to missed or late doses over the past 7 or 30 days. This finding may reflect caregiver unwillingness to admit suboptimal adherence to providers due to fear of stigma, embarrassment, or punishment. Studies from various settings have illustrated the importance of a positive patient–provider relationship in facilitating good adherence, 32 but there has been less work done among caregivers of young children living with HIV. 33 Caregivers may feel additional social pressure to report adherence to providers. Another possibility is that the caregiver answering the questionnaire is not the sole person responsible for giving the child ART, and thus, while the caregiver might be knowledgeable about general problems, he or she may not have knowledge about specific instances of missed doses.
The study protocol called for administering the adherence questionnaire items to children who had responsibility for their own medication-taking. As this was a younger cohort, the total number of children who responded to questionnaire items was low, which precluded robust analysis of child-reported items and their association with EAM. In addition, there was difficulty in assessing whether a child had responsibility for his or her medication-taking, which was also related to the child’s disclosure status; asking children questions about ART, even generally, may be considered risky or inappropriate by caregivers or clinicians when the child does not know they are HIV infected. Additional work is needed on how to solicit child perspectives in adherence assessment, including among younger children who may not know their HIV status or have sole responsibility over their medication-taking. One study among youth aged 7 to 16 years living with HIV found that self-reported adherence, including missed doses in the past 7 days, was significantly correlated with viral load. 34
This study had a number of important strengths. Electronic adherence monitoring was used as a reference standard, as has been done in other studies evaluating adherence assessment. 13,26 Compared to adults, there are fewer data using EAM technology among children living with HIV in resource-limited settings, including using MEMS to validate potential low-cost assessment tools such as adherence questionnaires. 15,26,35 These data help to guide adherence measurement in settings where EAM is not feasible. Children participating in this study were able to achieve high rates of adherence to ART, which is consistent with previous studies we have conducted in Kenya 16 as well as data published among children living with HIV using MEMS in Uganda 26 and Zambia. 15 Although the high rates of adherence among children in sub-Saharan Africa are encouraging, 36 there are few intervention studies to improve adherence to ART among this population. 37 This study was also strengthened by the fact that the adherence questionnaire was delivered by providers during routine clinical encounters with children. In discussions with providers in this setting, it was important that they had a simple tool that was both accurate and brief, as caring for a high patient load prohibits lengthier adherence assessments in the clinic setting. The adherence items identified as significant in this study may be integrated into the routine clinical examination form as screening-type questions, with patients referred for further adherence assessment or counseling based on their responses.
There are a number of limitations of this study to consider. First, convenience sampling was used to recruit participants, which introduced potential selection bias. Although current adherence was not considered for inclusion into the study, it is possible that children who had poorer adherence than average or children who had better adherence were more likely to enroll; however, this bias would not have impacted the validation of items. Second, although EAM is often considered the gold standard adherence measure, there are potential limitations to using this technology that have not been adequately explored in this population and in this setting. 38,39 Misclassification bias is a limitation whereby participants might remove more than 1 dose from the bottle at a time (“pocket dosing” in an example of this misclassification) or open the bottle without actually removing any medication (“curiosity event” is an example of this misclassification). In a previous study in a different cohort of child–caregiver dyads using MEMS in this setting, we found that most caregivers (88%) liked having the MEMS and would recommend it to others, while 21% reported that they did have concerns using it including that it was noticeable, difficult to carry, and fears of the device breaking. 40 To address some of these potential barriers, study participants were given training by study personnel on how the MEMS device works and how to care for it. Third, given that the participants knew that we were measuring their adherence using MEMS, this could have influenced their adherent behaviors. We did see an increase in adherence during the course of the study, and the procedures of the protocol likely had some positive intervention effects on patients’ level of adherence; however, this should not have impacted the validation analysis of questionnaire items. Finally, the study design did not allow evaluation of the effects of the questionnaire length and the person administering the questionnaire. Providers were trained on the administration of the questionnaire and were experienced in routine adherence monitoring, but there could have been provider-level differences that affected the validity of the questionnaire or individual items.
Conclusion
We provide evidence for the validity of a brief, 10-item adherence questionnaire administered to caregivers of children living with HIV on ART. Several questionnaire items related to who gives the child medication and caregiver-reported problems giving medication were significantly and independently associated with EAM over the course of the study, thus providing potential valuable tools for providers to quickly and accurately screen for suboptimal adherence and identify patients who may need further adherence evaluation and intervention.
Supplemental Material
Supplemental Material, Vreeman_Appendix._CAMP_Long-form_(Phase_3) - Validation of a Short Adherence Questionnaire for Children Living with HIV on Antiretroviral Therapy in Kenya
Supplemental Material, Vreeman_Appendix._CAMP_Long-form_(Phase_3) for Validation of a Short Adherence Questionnaire for Children Living with HIV on Antiretroviral Therapy in Kenya by Rachel Christine Vreeman, Michael Lawrence Scanlon, Wanzhu Tu, James Slaven, Samuel Ayaya, and Winstone Nyandiko in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Footnotes
Authors’ Note
The views expressed in this article are those of the authors and do not necessarily represent the view of the Indiana University School of Medicine or the Moi University School of Medicine. The primary author had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Acknowledgements
First and foremost, we would like to thank the families that sacrificed their time and energy to participate in this study. We also acknowledge the study’s coordinators and research assistants for their efforts, particularly Caroline Watiri, Judithi Toromo, Silas Wakoli, Ananda Roselyne, and Josephine Aluoch, as well as the nurses and clinicians who assisted in recruitment and testing of the adherence questionnaire. This research was supported by a grant to Dr. Rachel Vreeman from the US National Institute of Mental Health (1K23MH087225).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported in part by a grant (1K23MH087225) to Dr Vreeman from the US National Institute of Mental Health and AMPATH Plus with support from the US Agency for International Development as part of the President’s Emergency Plan for AIDS Relief (PEPFAR).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.