
Abstract
Background:
Despite recommendations for disclosure of HIV status to children living with HIV (CLHIV), fewer than half of CLHIV at the Instituto Nacional de Salud del Niño (INSN) in Lima, Peru, have had disclosure. How and when the disclosure process for CLHIV should take place in Peru has not been studied.
Methods:
We conducted a qualitative study at INSN to explore perceptions and experiences of 6 health care providers (HCPs), 14 disclosed and nondisclosed CLHIV (8-17 years), and their 14 caregivers regarding knowledge of illness, disclosure of HIV status, and appropriate disclosure approaches.
Results:
Disclosed children wanted to be told their diagnosis earlier. Nondisclosed children expressed frustration taking medications. Caregivers and HCPs discussed motivations to disclose, including educating, honesty, improving medication adherence, and preventing secondary transmission.
Conclusion:
Culturally appropriate guidelines and training for HCPs and caregivers are needed to support disclosure of children’s HIV status and ongoing support for CLHIV.
Introduction
With the advent of and increased access to antiretroviral therapy (ART), more children living with HIV (CLHIV) are surviving into adulthood. 1 The World Health Organization and the American Academy of Pediatrics strongly recommend disclosure of HIV status to school-age CLHIV (6-12 years old) as essential for their long-term well-being. 2,3 Early proactive disclosure of the child’s HIV status is necessary in order to focus on the child’s long-term disease management, psychosocial support, medication adherence, knowledge about HIV, and prevention of secondary transmission. 2,4 However, there are few studies to provide evidence-based guidance on how or when this disclosure should take place. 4 In addition, there are inconclusive data on the outcomes of CLHIV after disclosure, especially in resource-limited countries, where it is estimated that fewer than half of school-age CLHIV have been informed of their status, as well as significant variability within and across countries. 2
Since mortality was very high in the early years of the AIDS epidemic, many providers and caregivers believed that diagnosis disclosure would not result in favorable social and emotional consequences for the infected child and that it would be better not to disclose to protect the child’s emotional health. 5 When effective ART became available, and it became clear that long-term survival would become the rule rather than the exception, disclosure began to occur with higher frequency. 6 Disclosure became particularly critical when children approached adolescence, not only as the risk of transmission of HIV and other sexually transmitted infections needed to be discussed nearing the time of sexual debut but also when caregivers were pressed to justify the need for the child to adhere to drug regimens that often are difficult to tolerate and have significant side effects. 7
Research on pediatric HIV disclosure from resource-limited settings has shown that the rate of disclosure to children is low and that there are multiple child and caregiver factors related to disclosure. Child factors that are associated with greater disclosure are older age, inquisitiveness, higher perceived level of maturity, awareness of caregiver’s HIV status, school enrollment, and increased time since HIV diagnosis and ART initiation. 4 Caregiver factors are also manifold. Pediatric HIV disease is unique because of its mother-to-child transmission mechanism and the social stigma associated with the mechanism of maternal HIV acquisition. 8 As CLHIV acquire the virus perinatally, parental guilt about transmission also distinguishes HIV from other chronic pediatric illnesses. 9 The potential consequences of children developing negative attitude toward their parents may affect the parental decision about whether to disclose the child’s and their own HIV status to their perinatally HIV-infected children. This is further complicated by the caretaker’s fear of the child revealing the diagnosis to others, which could result in stigmatization from the people to whom the child’s HIV status is revealed. 4 Disclosure of the child’s HIV status often also involves disclosure of the mother’s HIV status and mode of acquisition and other family secrets. Additionally, research has shown that many caregivers feel unprepared to disclose to their children due to lack of knowledge about HIV infection, transmission, and treatment and would like guidance on how to disclose. 4,10,11 Focus group discussions among CLHIV, health care providers (HCPs), and caregivers have highlighted the complexity and importance of the cultural context in which the disclosure takes place. 11,12
Although the HIV epidemic in Peru remains concentrated in men who have sex with men and transwomen, one-third of the people living with HIV in Peru are women who are at risk of transmitting HIV to their children perinatally, and mother-to-child transmission of HIV represents 2% of all new HIV infections. 13 As of 2012, there are an estimated 1900 to 6900 Peruvian CLHIV ages 0 to 14. 13 Free universal ART became available to children in 2004, and according to the Peruvian Ministry of Health, 586 CLHIV have been treated with ART over the last decade. Of these, it is estimated that fewer than half had been disclosed their HIV diagnosis. 14 Peruvian children are primarily infected with HIV via perinatal transmission, though there are rare cases of pediatric infection via blood transfusions and sexual abuse, as well as sexual transmission in older adolescents. 15 There are national laws in place to prevent discrimination; however, stigma and discrimination are common. 13,16,17
There are no published studies on pediatric HIV disclosure in Peru and limited studies on pediatric HIV disclosure in Latin America. Of the manuscripts published in the last 10 years about HIV disclosure to children in resource-limited countries, all are from Brazil and the Caribbean. 4,18 –20 Research from resource-limited countries has identified many child, caregiver, HCP, and sociocultural factors unique to each cultural context that influence disclosure of a child’s HIV status. 4 However, few studies on disclosure of a child’s HIV status in resource-limited countries have included all of the 3 groups of key stakeholders: disclosed and nondisclosed CLHIV, their caregivers, and HCPs. 4,21 –23
We believe that furthering our understanding of how these 3 groups view disclosure and how and when it should take place within the unique cultural context and characteristics of the HIV epidemic in Peru will allow us to develop a disclosure protocol to support caregivers and HCPs in disclosing HIV status to CLHIV. Therefore, we designed a pilot qualitative study that explored the perceptions and experiences of disclosure of HIV status to perinatally HIV-infected children among disclosed and nondisclosed CLHIV, their caregivers, and HCPs. Our objectives were (1) to explore the perceptions and experiences of children and their caregivers regarding knowledge of their illness and ART, interface with medical care, disclosure of the child’s HIV status, and appropriate approaches for HIV disclosure and (2) to explore the perceptions and experiences of HIV clinic HCPs regarding overall HIV disclosure, advantages and disadvantages of disclosure for the different people involved, appropriate approaches for HIV disclosure, and public health systems and policies surrounding HIV disclosure to children.
Methods
Setting
This study took place in Lima, the capital city of Peru, at the Instituto Nacional de Salud del Niño (INSN), the national pediatric referral center, which offers specialized integrative HIV care. Children from Lima and surrounding provinces of Peru who attend INSN’s HIV clinic receive coordinated medical and psychosocial care every 1 to 3 months, take daily medication, and when hospitalized are roomed in a specialized ward. There are currently 218 children receiving HIV treatment at INSN, 118 (54%) ages 10-17 and 100 (46%) younger than 10. 14 Caregivers accompany children to their clinic visits and are frequently present during hospitalizations. There is currently a support group for caregivers of CLHIV, but no support group for adolescents. Comprehensive HIV care including ART is free. However, poverty is a barrier to care, and support for families who travel from outside of Lima, the capital, to cover transportation, lodging, food, and other costs is essential.
Participants
The 3 groups of study participants were (1) children perinatally infected with HIV between the ages of 8 and 17 years; (2) caregivers of the children in group 1, who were accompanying a child to the HIV clinic at INSN and whose child was also participating in the study; and (3) the HCPs of INSN’s pediatric HIV clinic. Both CLHIV and their caregivers were recruited for participation during regularly scheduled HIV clinic follow-up visits. All of the HCPs who were approached to participate agreed to participate in the study. Of the child–caregiver pairs, one refused to participate given the time requirement and already scheduled transport to return to their hometown.
Data Collection Methods
In this qualitative study, we conducted 34 in-depth interviews with the 3 participating groups: CLHIV (n = 14), their caregivers (n = 14), and the HCPs (n = 6) of INSN’s pediatric HIV clinic. Children were interviewed separately from their caregivers. Interviews were guided by a semi-structured guide that explored children’s and caregivers’ perceptions and experiences regarding knowledge of HIV and ART, interface with medical care, disclosure of the child’s HIV status, and appropriate approaches for HIV disclosure and HCPs’ perceptions and experiences regarding HIV disclosure, advantages and disadvantages for the different people involved, appropriate approaches, and the role of public health systems and policies surrounding HIV disclosure to children. Interviews lasted 30 to 60 minutes and were conducted one-on-one in a private room with a closed door where they could not be overheard. Health care providers and caregivers drew time lines of the current and ideal disclosure process for CLHIV. Participants were guided in Spanish by an interviewer who is not part of the HIV clinic team and who has extensive experience carrying out qualitative research in vulnerable populations. The interviews took place during a regularly scheduled visit, so there was no additional risk of being identified at the clinic.
Data Analysis
Digital audio recordings were transcribed verbatim. Transcribed interviews were analyzed using grounded theory to identify themes and relationships between themes. After reading of all of the transcripts, an initial codebook was developed. Two of the authors applied the initial codes to 1 transcript and then reviewed the coding to standardize the coding approach and to develop the draft codebook. Then, 1 author carried out the remaining coding. Coding was done using Dedoose software (Los Angeles, California, USA). Data were synthesized by theme and themes were analyzed within and across participant subgroups by 3 of the authors.
Ethical Considerations
This study was reviewed and approved by local ethical committees at INSN and the Universidad Peruana Cayetano Heredia in Lima and at collaborating sites’ institutional review boards: the University of California, Los Angeles and the University of California, San Diego. All participants were assigned a numerical identification code and an alias. For children, their age, sex, and disclosure status were recorded. All caregivers and HCPs provided signed informed consent. All participants younger than age 18 provided written assent to participate, and their caregivers provided written consent for their participation. None of the assent or consent forms had the words “HIV,” “disclosure,” or “AIDS” on them and no questions were asked about these topics unless the child self-disclosed his/her status.
Results
In total, 14 CLHIV (ages 8-17 years, mean age: 12.2 years), their 14 caregivers (ages 18-65 years), and the 6 HCPs of INSN’s pediatric HIV clinic participated (see Tables 1 and 2). Younger participants were less likely to have had their HIV status disclosed. Of the 14 CLHIV interviewed, 7 were male and 7 were female; 5 had not had their HIV status disclosed, all of whom were between 8 and 13 years old. The remaining 9 had their HIV status disclosed and were between 9 and 17 years old. Seven of the caregivers of these CLHIV were their mothers, 4 were grandmothers, 2 were legal guardians from the HIV group home, and 1 was the father. All the HCPs at INSN are female. The 2 physicians, psychologist, peer educator, clinic case manager, and nurse were all interviewed.
Children Living with HIV (CLHIV) and Caregiver Study Participants, Instituto Nacional de Salud del Niño (INSN), Lima, Peru, 2014.

Abbreviations: F, female; M, male; NA: not available.
Health Care Provider (HCP) Study Participants, Instituto Nacional de Salud del Niño (INSN), Lima, Peru, 2014.

The themes and subthemes that emerged from the 34 in-depth interviews are summarized in Table 3 and presented in the following section. Each participant quote is presented verbatim, followed by information about the participant in parentheses, using their alias.
Specific Objectives, Topics Explored, and Resulting Overall Themes and Subthemes.
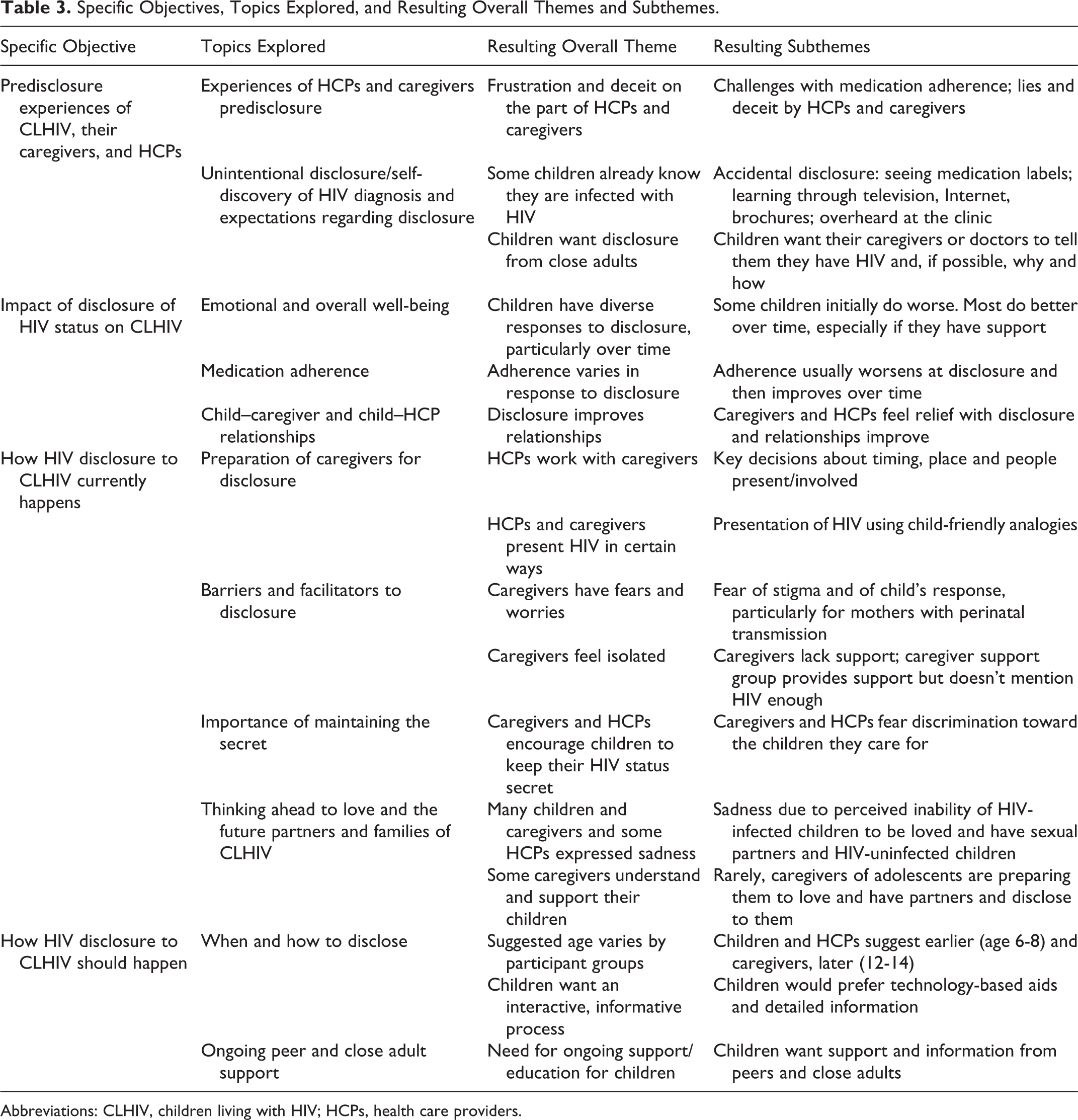
Abbreviations: CLHIV, children living with HIV; HCPs, health care providers.
Predisclosure Experiences of CLHIV, Their Caregivers, and HCPs
Frustration and deceit on the part of HCPs and caregivers
Both HCPs and caregivers expressed frustration with getting children to take their ART when their HIV status was not disclosed. Health care providers and caregivers also expressed how they have to lie to or deceive the child so as not to disclose their HIV status. Both disclosed and nondisclosed CLHIV described asking their caregivers and others about their diagnosis and not receiving complete answers. They [the children] ask…“why am I taking so much medicine? And I take it every day and never stop taking it?” They have siblings that get sick from colds and flu and they take a medicine for a few days and then stop. The child keeps taking the medicine and the mother tells him or her, “that you are anemic, or that you are suffering from heart problems, or that you are suffering from…” whatever illness they make up and that’s why they have to keep taking the medicine, but the child gets tired of it…and the mother doesn’t know what to say. (Isabella, clinic case manager)
Do you know why you take your medicines?
Yeah…to be healthy.
Have you asked someone [why you take your medicines]?
Yeah…and no one’s told me anything.
Who have you asked?
My mother. (David, 9-year-old male, not disclosed)
Unintentional disclosure/self-discovery of HIV diagnosis and expectations regarding disclosure
Prior to the disclosure event, many CLHIV already knew their diagnosis, even though their caregivers and HCPs had not told them, by recognizing the names of their medications on television, looking up the names of their medications on the Internet, being told by other CLHIV, overhearing their diagnosis in the hospital, or by reading pamphlets in the clinic. However, even the children who knew their HIV status still wanted their caregivers or doctors to tell them and they wanted to know more about why or how they became HIV infected. My aunt…told me that I was already big enough to know what I have and she told me that the medications that I take are for my health and I asked her what I have, but I already suspected from before because I had seen some prescriptions that said HIV…She told me that I had HIV but then I got sad because, why did I have this infection?…but she told me that my mom also had it, but she [didn’t explain how…she] only told me that I had this illness, that I had to take my medications, that I not forget. (Raquel, 12-year-old female, disclosed) I listened in on other people’s conversations…in the clinic room where they give medicine. I was there and I heard them talking about how everyone here has HIV…At the time I didn’t understand. (Gustavo, 15-year-old male, disclosed)
Impact of Disclosure of HIV Status on CLHIV
Improved Emotional Health and Quality of Life over Time, When Support is Available
There were diverse initial reactions by the CLHIV to the first disclosure event. Some children initially did worse and became depressed or acted out, and then with support, gained perspective and knowledge about their illness. Even with this perspective, however, they continued to view HIV as a challenge. I feel good. I feel at peace, because they didn’t tell me in a bad way, in a malignant way. They told me what I have, that I can control it, that nothing’s going to happen to me if I take [my medication]. I feel at peace, knowing why I take it…they told me in the correct way I think…I think that [having HIV] is a challenge. And it makes you a better person. It makes you better, you have reasons to succeed. Like saying, “I beat you, or I will not let you beat me,” something like that. And for me, it’s a challenge. (Emilio, 15-year-old male, disclosed) Some have improved their personal care. That is, they are aware that their medication is not because I want to give it to them, but because it’s necessary for their lives. Others, there is a complete rejection of their family. Of the parents. Of the father who infected the mother and the mother who infected the child. Some have even gotten in their mother’s face and asked, “if you knew, then why did you have me?”…They reject the world, not just their parents, but everyone else too. Until they come to accept it. But there are some who continue rejecting, and they don’t take their medication. (Sara, HIV physician) When the child processes the information one way or another, they accept it and that changes them, changes their self-esteem really. Then this is what we’ve seen, because we’ve given them a lot of support…[They say] “look how I am, I’m more beautiful, look, I’m healthier”…[We as staff say] “yes, you look beautiful”…We work under this parameter, of giving the child information. (Sofia, psychologist)
Other children continued to have poor emotional health and quality of life postdisclosure, especially if they had low levels of support. One child described the disclosure event when he was 13 years old as feeling alone and with minimal support from others at the hospital. He also explained how no one ever talked about his diagnosis again. One year ago…I was alone, it was just me…[my mother] was outside with my brother…and [the doctor] told me that I had a blood illness that was really serious and nothing else…I didn’t [talk] with anyone else…and my mom said, “so you already know?”…and my mom already knew but didn’t want to tell me. (Ernesto, 14-year-old male, disclosed)
Improved Medication Adherence over Time
Some children, caregivers, and HCPs reported worsening in medication adherence immediately after the disclosure event, which then improved over time. All participants expressed improved longer term medication adherence after disclosure. However, CLHIV stated a need for ongoing overall support and medication reminders. In response to a question about whether their lives have changed after finding out they have HIV, the following adolescent participants responded: I have to be more responsible…I have to take my medications at the right time every day. (Marina, 13-year-old female, disclosed) Before, yes, [I needed a reminder]. Sometimes my aunt would remind me…Now they say I’m older and I have to be responsible for my pills…and in some ways they are right. But sometimes I don’t want to take them…and so I don’t. (Emilio, 15-year-old male, disclosed)
Improved Child–Caregiver and Child–HCP Relationships
Health care providers and caregivers described that following disclosure of children’s HIV status, caregivers felt relief at not having to lie anymore. The majority of parents that have told their child say the child accepted it and the child already knew and they just wanted their mother to tell them or the doctor to tell them, so the [parents] feel at peace…because…they don’t have to lie or feel badly anymore. (Sara, HIV physician) I felt more relaxed, with whatever is coming up, I have the confidence to tell the two of them…to not hide things from them…Why would I hide things from them because my older son is always asking…“How is my brother?…How is his CD4?” (Alma, mother of Andrés, 9-year-old male, disclosed)
How HIV Disclosure to CLHIV Currently Happens
Preparation of Caregivers for Disclosure
Health care providers described providing integrated team support and preparation for the caregivers in the disclosure process, often having to pressure the caregivers over time until it actually happened. The HCPs allowed the caregivers to decide where and how the disclosure process would take place: if it would happen in the clinic or at home and if the HCPs or the caregiver would be the one to tell the child. Yeah, a lot of them [caregivers] refuse. They think that the kids are going to blame them…are going to do many things that have happened—they’ve run away from home, they’ve wanted to die, cursed their caregivers…Adolescence…is the time when they fall in love, the time in which they tire of taking [their medications]…And so for the caregivers you have to keep preparing them…tell them you have to keep talking little by little to your child, tell them the importance of taking their medications…The [kids] are depending on them, while they are with their parents and caregivers, in the group homes. (Isabella, clinic case manager) If the children ask, what is HIV?…I’ve explained to some of them, look, what happened is that you were born with a little bug inside your body…This little bug needs to be asleep and so that this little bug doesn’t continue growing. The only way to keep it asleep is to take this medication, every day, because if you don’t take this medication, these little bugs start multiplying, multiplying…One day there are going to be lots of them and the medication won’t do anything, and they are going to be everywhere in your body and we’re not going to be able to control them if that happens. (Ximena, nurse)
Barriers and Facilitators to Disclosure
There was reluctance from the caregivers to disclose to their children, as they feared HIV-related stigma toward and from their child and the child’s response in the form of anger or depression. Mothers were reluctant to discuss their own behavior that resulted in their child’s HIV infection. Mothers especially felt guilt and sorrow about perinatal transmission of HIV. It is something [your child to have HIV] you do not want as a mother of her children, right? But everything is already done…the only thing left to do is to keep fighting for him and giving him the best I can and continuing on, nothing else, but to look for and give all the best possibilities for my son…As a mom, I see it is very painful to tell a child what they have…because one day he will come to love another person, that person won’t accept him. The rejection will be toward me, he will blame me: “it was your fault, look at my life,” all these things…If I had waited [to tell him] until he was an adolescent, he would have blamed me even more, right? (Blanca, mother of Rubén, 17-year-old male, disclosed) I don’t see any of my old friends any more…Mostly here the people are afraid to speak, that is…I always see everyone quiet and I don’t ask them anything because I could make them feel bad. (Eugenia, mother of Ernesto, 14-year-old male, disclosed) Although it’s a support group…we focus on some specific task, like a handicraft or jewelry or handmade quilts…Usually we don’t talk about those topics [related specifically to our kids having HIV]. We do talk about our worries as parents…one [child] got sick…he’s getting better…we also try to support one another…(Alejandra, grandmother of Diego, 9-year-old male, not disclosed)
Importance of Maintaining the Secret
The topic of secrecy formed an important part of the disclosure process. After CLHIV were told their diagnosis, all were encouraged by caregivers and HCPs to keep their diagnosis a secret. Caregivers were worried about discrimination by family members, neighbors, and people at school. Health care providers also worried about discrimination, especially at school. They [the children] say, “can I tell my friend, my best friend?”…I tell them that you can’t be sure that they are going to accept you for who you are…that it might be painful for you…I tell them to keep their secret and…learn a little more about the topic…and if this is really a friend who wants the best for you…but this we cannot know, so…it’s better to avoid it. (Isabella, clinic case manager)
What do you think after having heard that you have HIV?
I don’t think about it so much; more I’m thinking about other things…like Facebook.
And do you have a group that you can talk with about HIV topics?
No. I don’t tell anyone about that. That stays with me. (Rubén, 17-year-old male, disclosed)
In his case, I’ll tell him, “you know, you have HIV and I love you, and I’m asking you please don’t go and tell anyone because the other kids can marginalize you and they can kick you out of school because they don’t understand, and they’re afraid.” He will understand and pay attention, and I know him, he’s a very mature boy. He’s going to do it for me, he won’t tell…But I’m not doing it, because like I told you before, he doesn’t understand anything because of his neurological status, [he doesn’t understand] how severe HIV is, and that’s why I don’t tell him. (Alejandra, grandmother of Diego, 9-year-old male, not disclosed)
Thinking Ahead to Love and the Future Partners and Families of CLHIV
Many CLHIV, their caregivers, and some HCPs expressed sadness at the perceived inability of CLHIV to be loved and to eventually have sexual partners and have HIV-uninfected children. I feel worried because I’m not like the others…I can’t have kids. (Gustavo, 15-year-old male, disclosed) There are children that say, “why should I live because no one is going to love me.” We have adolescents who suddenly fall in love and what they do suddenly is create their own barriers because they say, “no one is going to want to kiss me, no one is going to want to hug me”…We tell them that it’s important to communicate their diagnosis…if this is really a person that you can confide in…(Sofia, psychologist) I’m afraid…about what he has…that he can’t have a partner because of the consequences of being together, because he has this illness. (Alicia, grandmother of Samuel, 8-year-old male, not disclosed) Yeah, he’s told me, he’s been in love, but I always tell him, “son, before you make a mistake, think first. You’re not going to hurt anyone, the girl, look, it’s true you and I have this diagnosis, but…it’s not something that we asked for, to live with this, and I don’t want you to harm anyone else…He understands these things. (Blanca, mother of Rubén, 17-year-old male, disclosed)
Valeria represented an exceptional case in that her HIV diagnosis was made public in the media as a small child and in that her grandmother was preparing for her to disclose her HIV status when she falls in love in a very positive manner. Since I’m already 16 years old, my grandmother tells me that the moment is going to come in which you fall in love and you have to face this person and tell them what you have, and if this person leaves you it’s because they didn’t love you. She tells me, “if the person is really in love with you, they have to accept you for who and how you are, with what you have” She tells me and I listen to her, from 11, 12 years old she’s told me the same thing, up until today. (Valeria, 16-year-old female, disclosed)
How HIV Disclosure to CLHIV Should Happen
When and how to disclose
Children suggested starting the disclosure process from the age of 6 to 7 years, when children in group homes were usually told they have HIV. Health care providers suggested closer to 8 years old and many caregivers suggested in adolescence, between 12 and 14 years old. Health care providers discussed the difference between disclosing to older and younger children and that older children had more difficulty accepting their diagnosis. Children suggested having a more interactive disclosure process that might include videos, games, and audiovisual aids to help their understanding of HIV (Figure 1). The children that live in the group homes know their diagnosis very early on and they accept it naturally, but as they grow, they start to have difficulties and they get depressed or rebel. Some children cry, others say, “but I already knew”…We talk about, how much do you know? Do you know the importance of your medication?…Because that is what we stress the most…that life continues, that life is beautiful, that not everything is finished. [They ask] “Can I study?” Yes, that everyone studies…that you have to carry on, that there are kids in the university. (Isabella, clinic case manager)
[I would like to] watch videos about it [HIV]…to know a little more…because I didn’t understand very much…
Did you ask the doctor anything when she told you?
No.
Later on did you talk to your mom?
Yes…My mom only said to me, “you know now?” and I said, “yes…the doctor told me.” (Ernesto, 14-year-old male, disclosed)

Summary of suggested pediatric HIV disclosure time line by children living with HIV (CLHIV), caregivers, and health care providers (HCPs).
Children who lived in HIV group homes were told by the staff of their HIV status when they were around 7 years old, and they liked being told at a younger age. Since all of us had it [HIV], it was normal for me. It wasn’t anything out of this world…They told me “you have to take this medicine because if you don’t you will get sicker”…it didn’t make us scared and we didn’t worry about it. (Emilio, 15-year-old male, disclosed) Once I ran into a kid…here [at the hospital]. He was 16 and he said to me, “what, your son doesn’t know?…you should tell him because…I am 16 and I found out recently and sometimes I’ve wanted to kill myself…You won’t like it if it affects your son like that…I’m going to give you some advice, ma’am, tell him starting now [when her son was 5]…I’m really furious with my mother because of how late she told me”…So I started preparing myself to tell him…[with] the psychologist…and then the three of us talked together. (Alma, mother of Andrés, 9-year-old male, disclosed)
Ongoing Peer and Close Adult Support
Child participants expressed the need for peer support groups and ongoing support from caregivers and HCPs. This support would include general support for their physical, emotional and overall well-being, relationships with family members, and clarification of information about HIV transmission, pregnancy, and other topics as they arise, always in an age-appropriate manner. One CLHIV also expressed a desire to educate others to dispel misinformation around HIV. We talked about the illness, if our defenses were okay…Yeah, I liked the meeting [with the other kids with HIV] because it distracted me a lot and I got to know more friends. (Raquel, 12-year-old female, disclosed) When we were just little guys, they told us “so you don’t transmit HIV, you have to use a condom when you have sexual relations.” And for us, we thought that was really funny then…because we didn’t know anything about what sex was, nothing…we were eight, nine years old…I think if we all got together, those of us who are the same age, together with the doctors and the people we know here in the hospital, we could organize a going away party [for when we transition to adult care]. I also believe they need to inform us more…A lot of times people my age are confused…they think you can’t talk with others, or kiss others, and that you have to maintain a distance so you don’t get infected…[Also] “How can I have a better relationship with my family?”…[I would like to find this out] with the other kids, with others that have had the same thing happen to them as to me. (Emilio, 15-year-old male, disclosed)
Discussion
Peruvian CLHIV who had been disclosed, their caregivers, and HCPs all agreed it was essential to disclose the child’s HIV status in order to tell the truth, improve antiretroviral adherence, and prevent secondary transmission. Parental guilt, stigma, and perceived inability for children to understand all contributed to a delayed disclosure. Our results revealed a spectrum along which each group felt was the ideal age at which to disclose: CLHIV were more likely to suggest an earlier start to the disclosure process, beginning around 6 to 7 years old, while HCPs suggested closer to 8 years old and many caregivers suggested disclosure in early adolescence, between 12 and 14 years old. It is important to note the presence of this age discrepancy, so that it can be taken into account and incorporated into caregiver guidance procedures, in particular those who desire to continue postponing the start of the disclosure process. Children living with HIV expressed preference for a more interactive and ongoing process that includes peer support and multimedia strategies.
There is currently no formalized pediatric HIV disclosure strategy in Peru, and both caregivers and HCPs suggested the need for support and training surrounding the process. This finding is similar to findings reported in disclosure studies in other countries. 21,24 There were not strong feelings about whether the disclosure event should happen at home or at the clinic; however, CLHIV, caregivers, and HCPs all suggested that supportive people that the child knows and trusts should be present. Caregivers reported strong feelings of guilt and sadness around disclosing their child’s diagnosis; however, many then told of a feeling of relief that they could tell the truth.
Caregivers and HCPs were more likely to disclose or recommend disclosing to a child who was older, more inquisitive, and with the perceived maturity and ability to understand. Barriers identified by caregivers in disclosing to children included feeling unprepared, fearing negative repercussions of disclosing such as stigma if the child told others, and wanting to keep the HIV diagnosis a secret. All of these factors are in support of prior research. 4,11,12,21 Culturally appropriate guidelines for caregivers and HCPs on appropriate implementation of the disclosure process, answering potentially challenging or embarrassing questions, and addressing fears of resentment and shame could help to overcome these barriers to disclosure. 4,21 Additionally, there could be a role for disclosed CLHIV to discuss their disclosure experiences with caregivers who are reluctant to disclose to their children.
Both HCPs and caregivers discussed lying and deceiving the child before the disclosure event surrounding the child’s illness, need for medication, and clinic visits and hospitalizations. Children living with HIV reported unintentional disclosure of their diagnosis through a variety of mechanisms, including overhearing their diagnosis in clinic, despite efforts at secrecy by caregivers and HCPs. Even these CLHIV who discovered their diagnosis still wanted to be told of their diagnosis by their caregivers.
Literature has emphasized that disclosure of HIV status to children is not a one-time event but a process of gradually providing information over time based on the child’s developmental stage. 4,12,18,21,25,26 Disclosed children expressed a need for ongoing education and support, especially in adolescence. Although most children came to a place of acceptance with their diagnosis and had improved medication adherence and responsible health behaviors, others remained depressed or continued to rebel. Unstable home situations and difficult economic circumstances contributed to the stress of the caregiver and the CLHIV. In particular, CLHIV expressed a lack of information and resources surrounding sexuality, HIV transmission to potential sexual partners, and vertical transmission. Culturally appropriate guidelines and training for HCPs and caregivers are needed to support disclosure of a child’s HIV status as a process starting at an appropriate age, with ongoing support for adolescents as they transition to adult HIV care.
There are limitations to this research study. The sample size is small and not randomly selected. These data are from self-reports of those individuals’ experience. Children with significant intellectual disability were unable to participate in the guided interview, so their experiences and their caregivers are not included. The identity of the primary caregiver is, however, representative of the CLHIV cared for at INSN, based on a 10-year chart review: 51% lived with their mother or father, 20% with a relative, and 24% were from an HIV group home. 15 The strengths of the study include the diversity of perspectives represented including those of disclosed and nondisclosed CLHIV, caregivers, and HCPs, as well as being the first to examine pediatric HIV disclosure in Peru.
Conclusion
Among those caring for nondisclosed perinatally HIV-infected children, there was perceived difficulty with antiretroviral adherence and fear of potential secondary transmission. Disclosed children require ongoing education and support. Culturally appropriate guidelines and training for HCPs and caregivers are needed to support disclosure of a child’s HIV status as a process starting at an appropriate age. Qualitative data from diverse perspectives may help in the development of these guidelines.
Footnotes
Acknowledgments
The authors are grateful to the children, their caregivers, and the dedicated HIV clinic staff at INSN for their time in sharing with us and participating in this project. The authors also acknowledge Dr Debra Murphy for her review of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the South American Program in HIV Prevention Research (SAPHIR), NIH R25 MH087222.