
Abstract
Combination prevention efforts are now recommended toward reducing HIV incidence among men who have sex with men (MSM). Understanding the perceptions of both MSM and service providers is critical to informing the development of prevention packages and ultimately improving intervention effectiveness. This study assessed the preferences of MSM and health service providers in the administration of HIV-prevention efforts. Qualitative data were gathered from a series of separate MSM and health care provider focus groups in 2 South African cities. Participants discussed HIV-prevention services and MSM client experiences within South Africa and identified the 3 most important clinic characteristics and 3 most important HIV-prevention services for MSM clients. Priorities indicated by both MSM and health care providers were confidentiality of visit, friendly staff, and condoms, while discrepancies existed between MSM and providers regarding provider consistency and the provision of pre-exposure prophylaxis/post-exposure prophylaxis (PrEP/PEP) and lubricant as prevention methods. Effective interventions must address these discrepancies through the design of intervention and provider training to optimally accommodate MSM.
Keywords
Introduction
Approximately 6.8 million South Africans are estimated to be living with HIV, with an estimated adult prevalence rate of 18.8% (range: 17.9%-19.9%). 1 In the 1980s, the HIV epidemic in South Africa was originally attributed to homosexual transmission among white men and for several years was thought to be primarily affecting this group, with the expectation that HIV would remain a concentrated epidemic similar to epidemics witnessed in Europe and the United States. 2,3 However, a second pattern of HIV transmission emerged: a larger, growing epidemic among black heterosexual South Africans. 4,5 As the epidemic has long been characterized by heterosexual sex as the dominant transmission mode, 6 national HIV programs have largely focused on preventing heterosexual and mother-to-child transmission, with limited attention to other at-risk populations. 7 Recently, in South Africa, there has been evidence of a growing epidemic of HIV among men who have sex with men (MSM). 8 Although in South Africa the nationally representative data for MSM are not available, the HIV prevalence estimates derived from observational studies of urban MSM range between 10% and 50%, 9 –13 and the HIV prevalence among MSM has been estimated to be more than twice that of other men of reproductive age. 14 –16 Similar to the HIV epidemic in the United States, 17 it has been found that black MSM and those that identify with a sexual-minority community label are particularly vulnerable subpopulations. 10,18 It is estimated that nearly one-third of MSM living with HIV may be unaware of their serostatus. 19
There is also emerging evidence that South African MSM experience specific barriers to accessing HIV-prevention services. 20 –22 These barriers include the heterosexual focus of public health strategies for HIV prevention, which ultimately isolate MSM from services 13,22 as well as the stigmatizing views of some providers regarding MSM, which is compounded by limited training regarding sexual health of MSM. 11,13,20 –22 Men who have sex with men face high levels of social stigma and homophobic violence which may be associated with traditional attitudes toward sexuality. 23,24 A 2013 study found that less than a third of South Africans reported that homosexuality should be accepted by society. 25 Simultaneously, the progress and momentum in South Africa are encouraging; it is the only country in sub-Saharan Africa where gay rights are formally recognized, and national policies emphasized reducing discrimination based on sexual orientation. 26 Men who have sex with men were included for the first time in the 2007 to 2011 National Strategic Plan for HIV, and the South African government has developed specific efforts and resources to combat HIV among MSM, 15,19 including promotion of PrEP and routine HIV testing. 15
One promising approach to HIV prevention is the creation of combination prevention packages that conglomerate individually efficacious HIV-prevention measures into 1 package, which is targeted specifically to the unique needs and risks of a given population. Provision of a combination prevention package has shown significantly greater impacts on HIV incidence than the provision of single prevention option. 27 –29 In order to maximize the impact of combined prevention packages, it is important to work with both the specific population and the community of services providers expected to deliver the interventions, in order to understand their knowledge, willingness to utilize or provide, and acceptance of the prevention package components. 28,30
An important first step in the development of a combined package of HIV-prevention tools for MSM in South Africa is to determine which prevention tools MSM know, are willing to use, and understand as necessary to protect against HIV. 31 This article presents qualitative data obtained from focus groups of MSM and health service providers recruited in Cape Town and Port Elizabeth, to examine perceptions of the HIV-prevention needs of MSM. The focus is on comparing the perceptions of MSM (the clients) and service providers in order to inform the development of a combined package of HIV prevention tools tailored to the specific needs of MSM and to highlight the public health messaging and training strategies that are needed to successfully implement the package.
Methods
Focus group data were collected as part of a larger qualitative study assessing HIV-prevention services among MSM, in South Africa. 32 –34 The qualitative data collection efforts is the first step of a 3-stage process of developing and testing a combined package of HIV-prevention tools for MSM, in South Africa. Although participants were asked to indicate preferences, and those preferences were quantified to guide focus group discussions and analysis, the results presented should be considered qualitative in nature. Details of the project are previously described in McNaghten et al,. 34 This article presents the results of 11 focus group discussions: 5 with MSM and 6 with health care providers convened in Cape Town and Port Elizabeth.
Ethical clearance for the study was provided by boards at Emory University, Desmond Tutu HIV Foundation, and Human Sciences Research Council. Eligible MSM were of age ≥18 years, assigned male sex at birth, reported sex with a man in the last 6 months, and lived in Cape Town or Port Elizabeth, South Africa. Approximately one-third of participants were recruited using preexisting contact lists of MSM, gathered by local collaborating entities, Desmond Tutu HIV Foundation in Cape Town and the Human Sciences Research Council in Port Elizabeth. The remaining two-thirds were recruited by snowball sampling from these initial lists of men. 35 Participants were contacted by telephone and screened for eligibility. All participants provided informed consent and were remunerated with 80 Rand ($10 USD) for their time and for travel expenses.
Health care providers were recruited from clinics and organizations that provided HIV-prevention services to the communities in which MSM participants were living. Eligibility criteria for providers included presently serving as clinic or organizational staff that provided HIV testing, counseling, or treatment in either of the cities where MSM were recruited. Six health care provider focus groups were conducted: 3 in Cape Town and 3 in Port Elizabeth. Both MSM and providers were asked about their current clinics and experiences with HIV-prevention services. A series of prevention tools with visual representations was explained to participants who were then asked about their experiences and preferences with each. Prevention tools included HIV voluntary counselling and testing (VCT), condoms, lubricant to be used with condoms, PrEP/PEP, couples’ HIV counseling and testing (CHTC), over-the-counter and self-administered home HIV testing, HIV education, text message (SMS) health advice, and referral services. Participants were also shown a list of clinic characteristics and were also asked to discuss their experiences and preferences for each of these. Clinic characteristics included confidentiality of visit, friendly staff, short waiting time, having the same provider at each visit, clean environment, lesbian, gay, bisexual, and transgender (LGBT) sensitization, one-stop shop, MSM-specific space, the provider’s ability to ask MSM-specific questions, and incorporation of MSM services into a general testing space. Focus groups were conducted primarily in English, with local Xhosa translation available when needed.
Data Analysis
Audio recordings from each of the focus groups were translated (when necessary) and transcribed. Data were analyzed using a constant comparative method by comparing similarities and differences between emerging categories. 36,37 Independent coding took place across 3 coders, followed by consensus revisions and development of an inductive codebook. During the focus groups, participant votes were taken to indicate their experiences and desires for each of the clinic characteristics and HIV-prevention tools; votes were counted and tallied at each focus group. These client-expressed preferences were utilized by interviewers to guide and shape subsequent discussion. Codes were applied to the text to examine the reasons for the desired clinic characteristics and combined prevention package items. Analysis was conducted using MAXQDA version 10 (Verbi Software, Berlin, Germany). Key quotes are presented using pseudonyms to protect the privacy of participants. Quotes are presented by participant type, client or provider, and city of focus group attendance for confidentiality.
Results
The median age was 30 years (range: 19-67 years) for MSM focus group participants. Approximately two-thirds (60%) identified as black, 18% as colored (South African term indicating mixed ancestry), and 19% as white. Almost all participants identified as gay (95%), with 4 identifying as bisexual (5%). Nineteen (26%) participants reported living with HIV; self-reported HIV status was not confirmed by testing. Three focus groups with MSM were conducted in Cape Town and 2 with MSM in Port Elizabeth.
Tables 1–4 display the preferences indicated by participants. Clients based in Cape Town most frequently indicated that their currently attended clinic displayed the characteristics of confidentiality of visit, friendly staff, and general testing space (Table 1). Clients in Port Elizabeth expressed that their current clinic exhibited confidentiality of visit, friendly staff, short wait time, and same doctor at each visit. None of those from Port Elizabeth indicated that their current clinic had general testing space. The most commonly occurring characteristics at client’s current clinics in both cities were confidentiality of visit, friendly staff, and same doctor at each visit. Across both locales, clients most commonly selected confidentiality of visit, same doctor at each visit, and friendly staff as ideal clinic characteristics for MSM.
Client Experiences and Preferences for Clinic Characteristics.

Abbreviations: LGBT, lesbian, gay, bisexual, and transgender; MSM, men who have sex with men.
aThose characteristics that are present at a participant’s current clinic.
bThose characteristics that a participant ranked among the top 3 ideal characteristics to be included in a hypothetical clinic.
Provider Experiences and Preferences for Clinic Characteristics.

Abbreviations: LGBT, lesbian, gay, bisexual, and transgender; MSM, men who have sex with men.
aThose characteristics that are present at a participant’s current clinic.
bThose characteristics that a participant ranked among top 3 ideal characteristics to be included in a hypothetical clinic.
Client Experiences and Preferences for HIV Prevention Services.
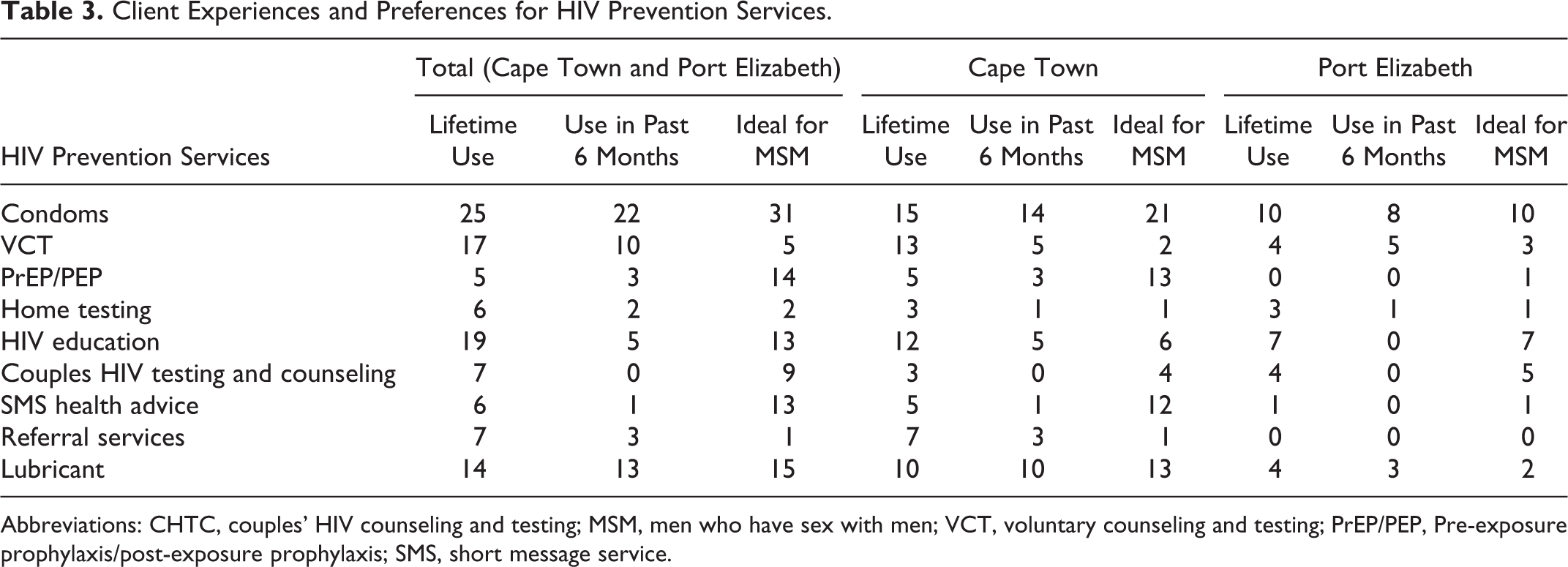
Abbreviations: CHTC, couples’ HIV counseling and testing; MSM, men who have sex with men; VCT, voluntary counseling and testing; PrEP/PEP, Pre-exposure prophylaxis/post-exposure prophylaxis; SMS, short message service.
Provider Experiences and Preferences for HIV Prevention Services.
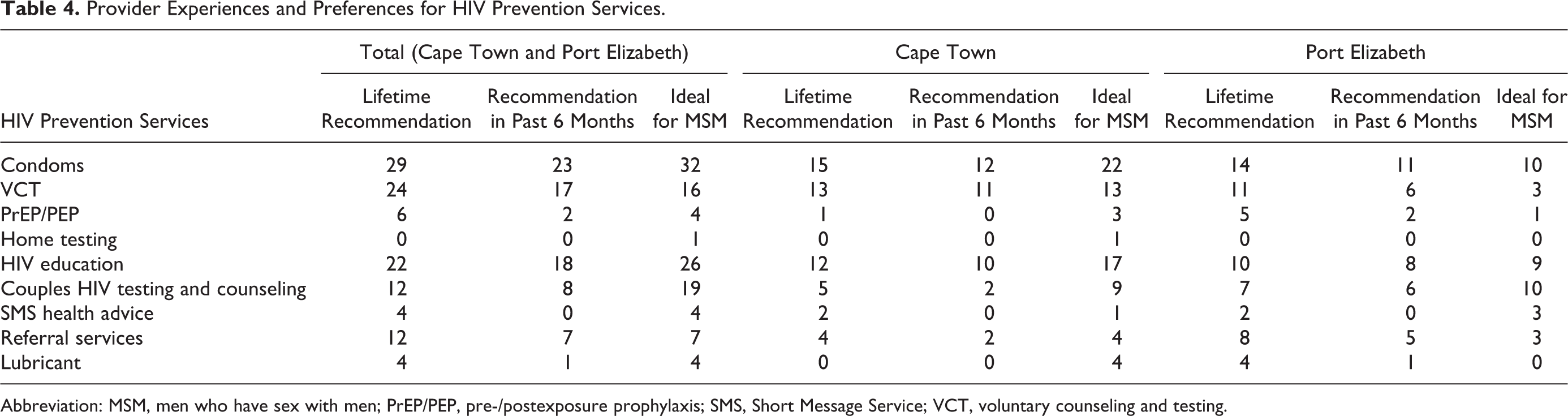
Abbreviation: MSM, men who have sex with men; PrEP/PEP, pre-/postexposure prophylaxis; SMS, Short Message Service; VCT, voluntary counseling and testing.
Health care providers from Cape Town perceived that their clinic of employment most commonly displayed friendly staff, confidentiality of visit, and clean environment (Table 2). Providers in Port Elizabeth most frequently believed their places of employment to exhibit confidentiality of visit, same doctor at each visit, short wait time, and clean environment. Despite its commonality in Port Elizabeth, only 1 provider from Cape Town expressed that the provider’s workplace featured same doctor at each visit. Health care providers in Cape Town believed that confidentiality of visit, one-stop shop, and MSM-specific testing space were the most ideal characteristics of MSM clients. Those in Port Elizabeth most commonly listed confidentiality of visit, friendly staff, and LGBT sensitization training as most important for MSM. This culminated in overall provider preference for confidentiality of visit and friendly staff, congruent with the top 2 selection of clients. The third most common ideal clinic characteristic selected by providers, however, was MSM-specific testing space, which ranked seventh among MSM.
At least 3 MSM in Cape Town expressed having ever used each HIV-prevention service, while none of the clients from Port Elizabeth had ever utilized PrEP/PEP or referral services (Table 3). Condoms, VCT, and HIV education were the services most commonly ever used by Cape Town clients, while those in Port Elizabeth had most common lifetime use of condoms, HIV education, VCT, CHTC, and lubricant. In the past 6 months, clients in Cape Town had commonly used condoms, lubricant, and VCT, and no members of this group had used CHTC during that period. Men from Port Elizabeth reported using only condoms, VCT, lubricant, and home testing during the previous 6 months. Men from Cape Town preferred condoms, PrEP/PEP, and lubricant as ideal prevention services for MSM; those from Port Elizabeth preferred condoms, HIV education, and CHTC. In total, clients’ top preferences were consistent with the views of men from Cape Town, favoring condoms, PrEP/PEP, and lubricant.
A minimum of 1 health care provider in each city had ever recommended each service to MSM except home testing, and providers from Cape Town never recommended lubricant (Table 4). For lifetime recommendation and recommendation in the past 6 months, providers in Cape Town and Port Elizabeth most often indicated condoms, VCT, and HIV education. In Port Elizabeth, providers also commonly recommended CHCT over the past 6 months. Providers in the Cape Town focus groups most often selected condoms, VCT, and HIV education as ideal prevention services for MSM; providers in Port Elizabeth selected condoms, CHTC, and HIV education. Overall provider preference was for condoms, HIV education, and CHTC.
Analysis of transcripts revealed 6 themes underlying the selection of clinic characteristics and HIV-prevention services that would be ideal for MSM. These categories are community stigma, health care stigma, patient adherence, personal/partner preference, availability of care, and perceived effectiveness.
Community Stigma
Both MSM and health care providers reported community stigma related to seeking HIV-prevention services among MSM, which influenced the selection of clinic characteristics and prevention services. Clients expressed a sense of marginalization within their local communities and “…especially from the straight people because the way they look at us is like we’re not a human being, or we’re not okay.…They care less about us, as men who sleep with other men” (Client, Cape Town). Clients indicated that clinic practices that indicated to other clients that they are either MSM or seeking HIV services and were regarded negatively. Clients indicated that some clinics separate those receiving HIV-related services, so that “…people they all [know] if you go for HIV test. They know that that side is for HIV people, do you understand? They all look at your face when you come back from that room” (Client, Cape Town). A small number of MSM also stated difficulty with sharing a waiting room with the general patient population because “…when you’re a gay person you have to sit on the bench while everyone look at you, especially for a drag queen like me. You really come out in a dress” (Client, Cape Town). These practices were frequently linked to a desire for confidentiality of visit, the most commonly selected ideal clinic characteristic by clients. A small number of MSM also linked negative views of these practices to the selection of the characteristics of one-stop shop, short wait time, and MSM-specific testing space. Complicating selection of an optimal location for testing, the majority of MSM expressed discomfort in attending the clinic nearest to their place of residence, electing to travel to a further site that was perceived to exhibit greater degrees of confidentiality of visit and friendly staff, 2 of the 3 most commonly selected ideal clinic characteristics: “I like to come to [specific clinic]; the nurses are more attentive and mostly is people I don’t know unlike the clinic that’s close to my house that everyone goes there” (Client, Port Elizabeth).
Providers also recognized the potential for encountering stigma for MSM and those seeking HIV-related care. Although no specific clinical practices were discussed as potential catalysts for community stigma, there was a clear belief among health care providers that “The moment people see people that they know, they stay away, especially when, if it’s a health provider or a, um, or a patients that a neighbor, people stay away if they feel they’ve been exposed to people that know they coming for a certain service” (Provider, Cape Town). This potential for community stigma was connected with a desire for confidentiality of visit and a one-stop shop, where it was perceived that a patient could be receiving any of a number of offered services. None of the providers involved connected community stigma to a desire for short wait time, as a number of clients did. Multiple providers echoed awareness of client travel to avoid community stigma. Those clients traveling long distances were perceived as wanting to enhance confidentiality of visit, as it was understood by providers that “…people, so many times, cross borders where they go to from one area to another just not to be seen and to be known” (Provider, Cape Town).
Health Care Stigma
Stigma experienced by MSM and those seeking HIV-related care extended beyond the community and into health care settings. Men who have sex with men shared patterns of health care worker behavior that discourage MSM from visiting specific clinics or disclosing that they are MSM. Included were instances of intentional and unintentional breaches of confidentiality and general poor treatment by health care providers. It was generally stated by clients irrespective of explicit discrimination, “…the minute they heard, you know, or they see your file and they ask you, and you say you are gay, there is this immediate shift in attitude” (Client, Cape Town). Clients connected this and similar interactions with a desire for confidentiality of visit, friendly staff, same doctor at each visit, and MSM-specific questions from provider, the top 4 clinic-characteristic selections by clients.
Clients also shared that the potential for encountering stigma can cause an aversion toward visiting a new clinic. In selecting a provider, it was important to many MSM to have “…someone who’s going to understand the types of symptoms or I’m going through, these things that are related to gay men” (Client, Port Elizabeth). This desire was linked to the selection of same doctor at each visit and MSM-specific questions from provider, which were both discussed as manners of assuring that a provider would be sympathetic to issues of health for MSM and would understand the sexual behaviors of MSM. This potential for stigma was further linked with the selection of SMS health advice as an ideal prevention service. One client felt that “…there’s no way I’m going to go to a clinic, just for certain things. I have my cell phone. So, it would be nice to know I can ask for any information about anything. I can just SMS and you know, [ask] what do I do or how do I…with lube and stuff” (Client, Cape Town).
Providers acknowledged that stigma exists within some clinical settings. Although none of the providers participating explicitly stated that their own practice would be affected by personally held stigmatizing views of MSM or those seeking HIV-prevention services, multiple providers gave responses that suggested some level of underlying stigma of same-sex practices. One provider stated “I wouldn’t encourage uh uh promoting men and men sexual projects but that doesn’t mean that I wouldn’t provide the services…But it’s not a thing that I would enjoy doing it honestly speaking” (Provider, Cape Town). Another indicated that the volume of patients at the clinic, rather than an agreement of confidentiality, was what prevented the provider from sharing clients’ HIV statuses with their partners: I get somebody who’s HIV positive…someone who has a partner, and sometimes you have to talk about it with your partner, but people are not going to tell that person. They’ve got a problem, because I know that girl is HIV positive, but I didn’t know that she’s staying with him, and I never knew that she carried HIV. So the big problem is when the clinic is bigger and opening. Before, I could tell someone, you know, she is HIV positive, but now, the clinic is bigger, and I can’t say anything. (Provider, Port Elizabeth)
Patient Adherence
Patient adherence to HIV-prevention service recommendations was discussed by both clients and providers. Clients identified a potential lack of adherence to certain HIV-prevention services. Potential inconsistent adherence to PrEP/PEP appeared to slightly mediate its popularity among MSM, although it still ranked third among ideal prevention services. It was further stated that “To prevent HIV [lubricant] would be much easier for me [than] for me to wake up and take the PREP-PEP and use a, carry condoms with me, everything” (Client, Cape Town). This belief that lubricant was the most likely service for MSM to adhere to was common throughout the client sample. Multiple providers indicated that, in their experience, MSM “…didn’t adhere to any of [their] treatment whether it was wellness or ARTs” (Provider, Cape Town), but this was not directly connected with any ideal clinic characteristics or prevention services. Numerous comments by clients and providers established a belief that “…couples testing encourages bonding between the couple, [even] besides knowing the status of your partner” (Provider, Port Elizabeth). It was further expressed that “…if couples do [CHTC] together it’s either they are going to develop a trust between them. If both of you know your status then I think you can be faithful to one another and all of that” (Client, Port Elizabeth). Adherence to agreements of sexual monogamy was linked to the intimacy that CHTC created, which both clients and providers cited as reason to select this as an ideal HIV-prevention service.
Personal/Partner Preference
In discussing HIV-prevention services, participants often described the importance of partnership dynamics, including personal and partner preferences, to provide background for the preferences of the community. Men who have sex with men had varying preferences surrounding condoms. When responding to the interviewer’s inquiry into possible barriers to condom use, clients said “If your partner doesn’t want to use condom” (Client, Cape Town), “Maybe you don’t like it yourself” (Client, Cape Town), and that “…there are still MSM, men sleeping with other men, that still don’t use condoms because they’re trying to save for love or they’re trying to protect their relationship” (Client, Cape Town). As condoms were nonetheless an ideal HIV-prevention service selected by every client, this recognition that it may not be utilized in every situation did not detract from its desirability. Recognition of the potential for varying personal preferences, however, motivated the selection of services that can be utilized even when a condom is not, including PrEP/PEP and lubricant, which were characterized as assurance that “At least there’s something to back you up, even though you have to go test” (Client, Cape Town). This is further motivated by clients sharing preference for the personal comfort of lubricant and preference for PrEP/PEP and VCT when one does not like the sensation of condom use. Providers did not mention the notion of personal or partner preference when making selections.
Availability of Care
Availability and accessibility of specific services were put forward as contributing factors to the choices of clinic characteristics and HIV-prevention services by both clients and providers. Physical accessibility played a large role in the selection of PrEP/PEP as a prevention service by clients. As PrEP/PEP was largely unavailable in each of these regions at the time, most involved were largely unfamiliar with the PrEP/PEP programs, but frequently selected it as an ideal service after the interviewer’s brief explanation, desiring greater availability of the service for MSM. One client stated that “[PrEP], I think they must give everyone so that the drugs must be in their blood when the HIV goes into their body” (Client, Cape Town). Temporal accessibility was discussed among clients. “Short waiting time [was selected as ideal because] sometimes you have to be somewhere else and you don’t want to wait in a queue all day” (Client, Cape Town). In addition to short wait time, temporal accessibility was connected to a desire for same doctor at each visit. A number of clients felt that, at public clinics, “When you come they make you wait long. So you know what it’s much easier to go to a private doctor…as soon as you can” (Client, Cape Town). The financial dynamics of care were also conferred by clients. Although other factors often complimented the decision, some clients “…prefer [a specific doctor] because [they] use medical aid, so [clients] don’t have to pay” (Client, Port Elizabeth). Whenever mentioned, this sentiment supported the selection of the same doctor at each visit. Unlike clients, none of the providers mentioned financial impact as a reason for selecting any particular ideal clinic characteristic. Providers’ interpretations of accessibility shaped their selection of ideal characteristics and services as well. Similar to clients, providers were largely unfamiliar with PrEP/PEP, and it was shared that only PEP was available in at least 1 of the regions. This lack of practical knowledge and current availability likely contributed to providers’ decreased selection of this prevention service. Providers also recognized the significance of long wait times at clinics, saying that “staying in a clinic from let’s say 7 o’clock to 4 o’clock, it’s not a friendly approach to patient care” (Provider, Cape Town). As with clients, providers linked the impact of long waits to selection of short wait time among clinic characteristics.
Perceived Effectiveness
A final theme, which was salient throughout selection of HIV-prevention services and which was present among the selection of some clinic characteristics, was perceived effectiveness. Clients repeatedly shared concise and largely uncontested beliefs that “…condoms reduce the risk of HIV” (Client, Cape Town) and that “…there are less risks of getting HIV when you use lube” (Client, Port Elizabeth). The commonly held belief in the effectiveness of condoms and lubricant as primary methods of preventing HIV supported the selection of these as the top 2 ideal prevention services. Clients further established PrEP/PEP, VCT, CHTC, and HIV education as secondarily effective methods of prevention that can be utilized when the primary methods are not. Both VCT and CHTC were viewed as prevention options for those in committed partnerships who “decide that that’s been too long, [they] feel like [they] should not use a condom at all, [they] ask the partner ‘can you go and test?’” (Client, Cape Town). HIV education was explained as a catalyst for the use of other prevention methods. Clients across multiple focus groups attributed their personal decisions to engage in safer sex practices to specific HIV-education programs.
Several providers expressed concern that “[MSM] are very high risk of getting HIV because of the route they take” (Provider, Cape Town). Primary prevention methods were frequently described in that “…it is very important for [providers] to test them [and] Irrespective of what the results are, condoms are wise” (Provider, Cape Town). This notion of augmented risk was common among providers, and condoms, HIV education, and testing, including both VCT and CHTC, were recurrently portrayed as effective primary methods of mediating that risk. Providers additionally reasoned that HIV education, VCT, and CHTC were believed to be among the most effective of primary prevention measures because they encourage the use of other prevention services. It was shared that “…anybody that’s educated will, they will obviously go to the VCT to know their status, they will use condoms to protect themselves” (Provider, Cape Town). Unlike the more general popularity among clients, only 4 providers indicated that PrEP/PEP was an ideal method of preventing HIV transmission. Those that discussed PrEP/PEP recognized it as secondary to other prevention methods that they believed should also be employed. One provider shared belief that PrEP/PEP should be available so “If, by any chance [the condom] breaks…they can consult a doctor, and the doctor will give them the PEP” (Provider, Port Elizabeth). Unlike clients, providers rarely selected lubricant as effective primary or secondary HIV prevention.
Discussion
Collaboration between MSM clients and providers has been shown to improve engagement in HIV-preventive care including testing, 38 adherence to PrEP regimen, 39 and secondary prevention through treatment adherence. 40 Similarly, MSM clients’ perception of a lack of health care provider understanding has been associated with never having tested for HIV, 41 increased sexual risk taking, 42 and decreased utilization of all health care services. 13 Improving the relationship and establishing positive rapport between MSM clients and health care providers is crucial to improving awareness of prevention options and uptake of services, ultimately reducing HIV transmission. 12 The qualitative data presented here describe both consistencies and discrepancies between MSM and health-care providers’ understandings of the HIV-prevention needs of MSM. The identified discrepancies reveal the manner in which improvement can be made toward greater accessibility by specifying many of the boundaries experienced by MSM and the ways that providers already acknowledge or perpetuate those boundaries. The data also exposed differences within groups across cities, emphasizing the importance of tailoring HIV-prevention efforts to the locale as well as the population.
Determining the most effective method of service administration to sub-Saharan MSM has been raised as a research priority by previous studies. 12 As stigma and discrimination have been identified as prevalent barriers to care for South African MSM, 11,13,20 –22 determining operative methods of overcoming these barriers is essential to establishing optimally accessible services. Clients and providers in both cities highly ranked confidentiality of visit, and friendly staff among ideal clinic characteristics, indicating that there is already mutual understanding in this regard. Multiple client and provider comments, however, indicated breaches of confidentiality, and clients reported numerous instances of unfriendly interactions with providers. This apparent inconsistency regarding HIV-service administration between perception and behavior has been reported in previous study 43 and has been found to be more prevalent among health care workers with limited exposure to patients living with HIV. Similarly, many providers in our study expressed limited exposure to MSM clients, which may cause them to be less aware of the behaviors that MSM clients may perceive as discriminatory or stigmatizing, as has been reported in other sub-Saharan contexts. 44 Future efforts may benefit from accounting for this potential gap in provider knowledge and incorporating provider-focused educational interventions, such as those from The Global Forum on MSM and HIV, 45,46 the ANOVA Health Institute, 47,48 and the Desmond Tutu HIV Foundation 49 that seek to maximize access to care for MSM.
In the identification of the necessity of further research regarding implementation of HIV-prevention services for sub-Saharan MSM, specific attention has been given to determining whether services should be administered vertically, at clinics designated for MSM, or horizontally, with MSM-specific resources available at general clinics. 12 Although prior research has found high acceptability of MSM-tailored interventions among South African MSM, 13 there has been minimal investigation regarding whether this preference is for the integration of MSM-tailored services into a general clinic or for a separate MSM-specific clinic. Despite previous indication that stand-alone, MSM-specific testing spaces may be the client-preferred method of HIV-prevention service administration, 50 there was low ranking of MSM-specific testing space among our study’s MSM participants. Men who have sex with men studied indicated little preference for either stand-alone or MSM-specific clinic sites. It is possible that study participants who hold a preference, however, did not feel that this preference ranked among their top 3 concerns. Conversely, high rankings of MSM-specific testing space were present among providers and may be consistent with the findings from another sub-Saharan context, in which providers linked a lack of previous interaction with MSM and decreased willingness to administer HIV-prevention services to this population. 51 As detailed above, a number of providers in our study expressed little or no know experience with MSM clientele, underlying greater favorability of clinic characteristics that would not require increased personal interaction with MSM.
Regarding HIV-prevention services, there was an overall client preference for condoms, lubricant, and PrEP/PEP. There were some site-specific preferences, with clients involved in Port Elizabeth also expressing strong preference for HIV education and CHTC. Comparable similarities and differences have been found among the MSM from cities involved in a study by Lippman et al. 30 Men who have sex with men from all of the cities in the study expressed greatest preference for condoms, but the participants from only 1 city (Lima) did not prefer services that they had not yet utilized, specifically PrEP, and were most likely to prefer CHTC. 30 This variation was attributed to Lima’s lack of public LGBT support compared to the other cities involved. In our study, MSM in Port Elizabeth, which does not feature the same structural support for LGBT health equity as Cape Town, 52 favored services that they had already utilized, including CHTC, and were against new services, including PrEP/PEP. This linkage between social capital and HIV-prevention service utilization has begun to be studied in other African contexts, 53 and determining the mechanism and strength of this linkage among MSM in South African cities is a direction for further research.
Prior studies regarding the development of MSM-targeted HIV-prevention measures emphasize that maximum uptake requires that the intervention accommodates the needs and desires of MSM, 30,54 while minimally impeding on individual sexual satisfaction. 55 As indicated by MSM focus groups, ideal clinic characteristics for men in these locations include confidentiality of visit, same doctor at each visit, and friendly staff, whereas ideal HIV-prevention services are condoms, lubricant, and PrEP/PEP. Future interventions targeting South African MSM can be optimized by accommodating these identified preferences of MSM and educating providers regarding the needs of this population. 12,27,29 Further studies to determine the needs and preferences of MSM across other sub-Saharan locales can utilize the information revealed through this study as a basis of understanding and a model of MSM engagement.
There are several limitations to this study. The sampling method, which utilized existing contact lists from community-based organizations, may have overrepresented certain subgroups of MSM. This facilitated access to a somewhat hidden demographic in South Africa but may have limited the generalizability of the study. For example, young men and men who self-identified as gay were highly prevalent in this sample. Men who have sex with men who are not well-connected with community resources may have considerably different needs and preferences that would add value to the study. Recall bias and social desirability bias may have also influenced the results, as MSM were asked to share past clinical experiences and personal opinions in a group setting.
This study provides data comparing the clinical and HIV-prevention service preferences of MSM and health care providers in South Africa. The findings of this study provide groundwork for the development of a combination prevention package tailored to the needs and preferences of South African MSM. Information is also presented that provides a basis for the tailoring and integration of a parallel intervention targeting providers, working to bridge the divergence between them and MSM clients. Future HIV-prevention efforts may benefit by utilizing this knowledge to gauge the preferences of sub-Saharan MSM and implementing optimally accessible and relevant HIV-prevention interventions for South African MSM.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.