
Abstract
Background:
Intimate partner violence (IPV) is a severe form of abuse prevalent in urban and rural areas of India with its effects on mental and physical health of the person receiving it, leading to a poorer quality of life.
Methods:
A cross-sectional study was conducted among 99 women living with HIV, and information was collected using abuse assessment scale. The data were entered and analyzed using SPSS version 17.0.
Results:
The IPV was reported by 19.2% of the respondents, of which psychological (14.1%) was most common followed by physical (4.1%) and sexual abuse (1.0%). The experience of IPV was significantly associated with socioeconomic status, number of children, marital status, and CD4 counts of the participants.
Conclusion:
The prevalence of IPV in our study was found to be less compared to previous studies, however, there were significant association among factors such as socioeconomic status, CD4 counts, and marital status of the participants.
Introduction
Intimate partner violence (IPV) is a severe form of abuse prevalent in urban and rural areas of India. Women with retroviral diseases such as HIV/AIDS suffer abuse at the hands of their partners, which leads to poor quality of life (QOL). 1 This also makes them more prone to depression and nonadherence to their antiretroviral therapy (ART). 2 People living with HIV (PLWHA) who encounter IPV tend to show higher rates of HIV risk behaviors, sexually transmitted infections, drug and alcohol abuse, and increased incidence of cardiovascular diseases such as hypertension and stroke. 3 –8 Violence against females may lead to deleterious outcomes such as bodily injuries and psychological injury not only for the women but to their families and to society at large. 9 Also, there is a higher risk of IPV on pregnant women with HIV, which may lead to problems in getting the care needed for HIV-positive mothers and children. 10
HIV/AIDS and its sequelae by themselves are associated with poor QOL. 11,12 There is a complex relation between HIV and IPV, in which IPV escalates the risk of HIV infection and HIV-positive status perpetuates IPV due to victimization. 4,13,14 Studies have shown that IPV arises after the disclosure of seropositivity, and it is more prevalent among people with seropositive partners than seronegative/status unknown partners. 14 –17 People living with HIV experiencing IPV as adults are often seen with reduced CD4 counts, increased viral load, and lesser participation in their care. 3 Ezeanochie et al found that the prevalence of IPV in Nigerian women was 32.5%, the most common form of violence being psychological (27.5%) and least common was physical (5.9%). 9 The determinants of IPV included multiparity, participants with a seropositive child, prior exposure to violence before the diagnosis of HIV, and women with husbands without postsecondary education. 18 In all, IPV and HIV are a deadly combination that warrants sincere attention from doctors and counselors all over and should be given the appropriate modicum of care to prevent a further deterioration of the current situation.
Studies have shown that the prevalence of HIV infection was more among Indian women exposed to IPV from their spouses than in those not experiencing IPV. 19 –21 This is similar to studies done elsewhere. 22,23 However, IPV is underestimated, undisclosed, and, to a certain extent, a social taboo. Hence, not much data are available especially in the regions of coastal South India. This study has tried to fill the void in this context.
The objective of the present research was to assess the occurrence of IPV among HIV-positive women visiting the ART centers of a tertiary care center in Mangaluru and the factors affecting it such as their socioeconomic status, addiction status of their partner, and the severity and form of abuse (including psychological, physical, and sexual abuse) that they are exposed to.
Methodology
A cross-sectional study was conducted at ART Centers of KMC Attavar Hospital and Government Wenlock Hospital, Mangaluru, Karnataka, where all HIV-positive women attending the center were explained about the research by a counselor and HIV physician, and an informed consent was obtained from the study participants. Ninety-nine participants were recruited using the nonrandom sampling technique, and the study was undertaken over a duration of 60 days, from May to June 2014. Women younger than 18 years; uncooperative women; and those having AIDS-related dementia, chronic diseases such as hypertension and diabetes mellitus, and admitted for HIV-related opportunistic infection were excluded from our study.
The research was approved by the institutional ethics committee of Kasturba Medical College, Mangaluru. A sample size of 99 was calculated on the basis of prevalence of 32.5% IPV against HIV-seropositive women, 9 an absolute precision of 10%, a confidence interval of 95%, and a nonresponse rate of 10%.
Information was collected using a pro forma containing 2 segments and a semistructured questionnaire containing 4 different segments. The first segment dealt with the sociodemographic data of the patients, which included their age, religion, marital status, and number of children. The second segment dealt with the HIV-related aspects such as the CD4 count, time since seropositivity, mode of infection, total number of visits to the ART center in a year, and the addiction status of their partner. Abuse assessment scale 24 was used to assess the IPV faced by the participants, which contained questions concerned with the type of abuse they have gone through including mental, physical, or sexual and also how long have they been a victim to IPV and the frequency of the same. The World Health Organization Quality of Life Instrument for HIV clients (WHOQOL-HIV BREF) 25 was used to assess the QOL, and Beck Depression Inventory 26 was used to assess depression.
The socioeconomic status of the HIV-positive women was measured by the Kuppuswamy socioeconomic scale. 27 The collected data were entered and analyzed using SPSS version 17.0. For qualitative data, χ2 and Fisher exact tests were used. For continuous data, 1-way analysis of variance test was utilized, and statistical significance was considered at P < .05.
Observations and Results
Sociodemographic characteristics of the participants are shown in Table 1—mean age of the participants was 35.8 ± 6.6 years, with a maximum age of 58 years and minimum of 24 years. The mean CD4 count of the study participants was found to be 564 ± 174 cells/mm3 of blood. Maximum participants were Hindus (n = 90, 90.9%) followed by Christians (n = 7, 7.1%), and Muslims (n = 2, 2%). Most of the HIV-infected women were married (n = 86, 86.9%), 6 of the participants were widows (6.1%), 4 were unmarried (4%), and 3 were divorced (3%).
Sociodemographic Characteristics of the Study Population.a

aN = 99.
Regarding the route of transmission of infection, 31 (31.3%) of the participants refused to reply and 68 (68.7%) of them said unprotected sexual intercourse. At the time of research, 77 (79%) of the participants were on HIV medication. Most of the participants were HIV-positive since 5 years.
Of the 99 HIV-positive participants, 19 (19.2%) reported they had various kind of abuses from their partners, 6 (6.1%) of them refused to answer, and 74 (74.7%) didn’t report any such violence. Among those who reported to have been abused, mental abuse was the most common (n = 14, 73.7%) followed by physical abuse (n = 4, 21.1%), and the least common was sexual abuse (n = 1, 5.2%). Majority of our participants are being abused since 4 years, with some as long as 6 years and some for a period of 3 months.
Table 2 depicts the domain-wise QOL scores of the participants. On a scale of 0 to 20, the scores were uniformly distributed across all domains. Table 3 depicts the association between IPV and different domains of QOL among the study participants. A slight reduction in QOL was evident among those who experienced IPV among the domains of psychological, spiritual, and environmental health. However, there was no statistically significant association between the 2 across all domains.
Domain-Wise QOL Scores among the Study Participants.a

Abbreviations: SD, standard deviation; QOL, quality of life.
aN = 99.
Association between Intimate Partner Violence and Quality of Life.a
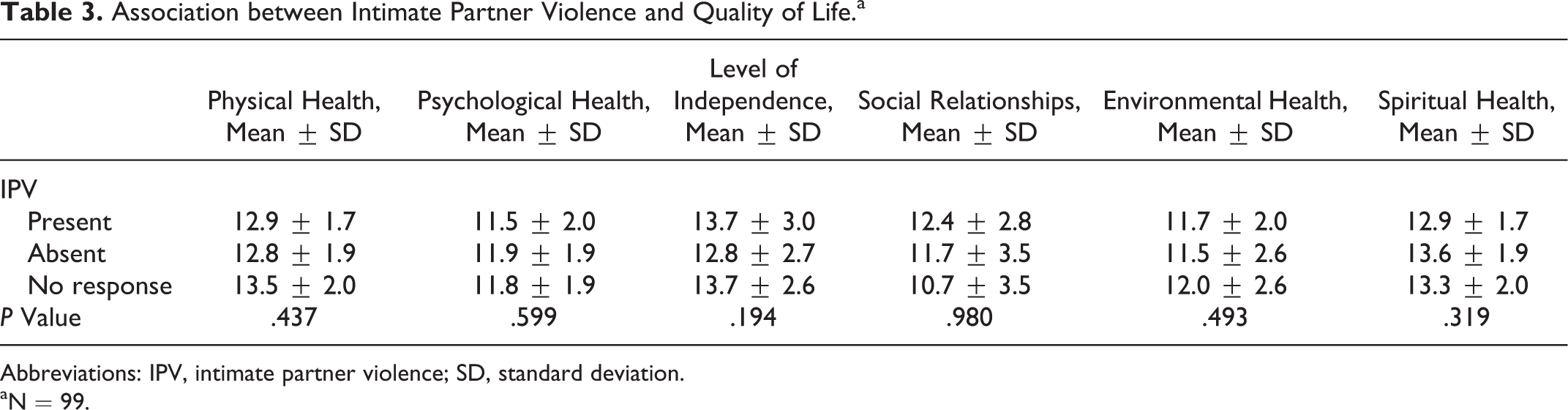
Abbreviations: IPV, intimate partner violence; SD, standard deviation.
aN = 99.
Table 4 describes the prevalence of depression among the participants. The prevalence of any form of depression was found to be 28 (28.2%). However, there was no statistically significant association between IPV and depression (P = .387).
Prevalence of Depression among the Study Participants.a
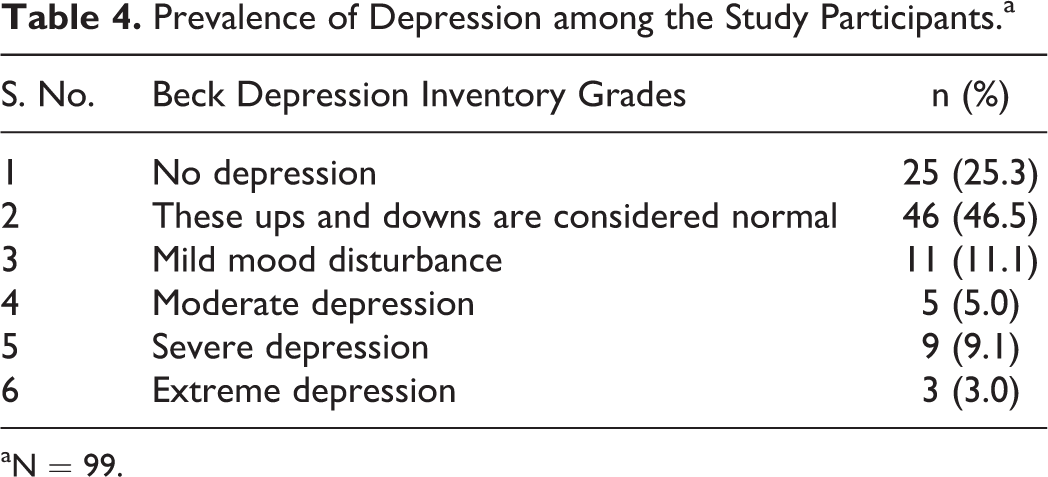
aN = 99.
Adherence was found to be 100% in all participants who were taking ART irrespective of their exposure to IPV. We observed that participants who experienced IPV had lower levels of mean CD4 counts (471.3 ± 153.2 cells/mm3 of blood) compared to those who didn’t (591.1 ± 172.4 cells/mm3 of blood), and the association was found to be statistically significant (Table 5).
Association between IPV and CD4 Counts.a

Abbreviations: IPV, intimate partner violence; SD, standard deviation.
aN = 99.
Table 6 depicts the association between IPV and the sociodemographic variables. It can be clearly seen that IPV was associated with lower socioeconomic status, those who were divorced, and those with 2 or more children. The associations were found to be statistically significant.
Association between IPV and Sociodemographic Factors.a

Abbreviation: IPV, intimate partner violence.
aN = 99.
Discussion
The present study was conducted to assess the burden of IPV among women living with HIV and its relation with important aspects like QOL, depression, and adherence. We found out a significant association between low CD4 count and IPV exposure, similar findings were observed in a study conducted by Schafer et al. 3 Another study conducted in Southern Alberta showed that IPV was more often reported by women with diagnosis of HIV earlier in the course of the disease, which is characterized by low CD4 levels, supporting our finding. 28
Regarding the type of abuse, mental abuse was the most common (73.7%) followed by 21.1% who reported being physically abused and 5.2% who said they were sexually abused by their partners, and the overall IPV prevalence was found to be 19.2%. Our findings are in agreement with the findings of a study done in Nigeria where they found that psychological (mental) violence was the most prevalent (27%) and composed of verbal abuse, threats, and humiliating comments. Although sexual violence was reported more often than physical violence and IPV prevalence was 32.5%, these can be attributed to larger sample size studied by them and underreporting by participants in our study due to social taboo. 9 Our results have also shown similarity to the study by Siemieniuk et al where they found that the most frequently reported forms of IPV were emotional and physical forms of IPV followed by sexual violence. 28 Another study by Ramachandran et al on the same aspects reported similar findings. 29
It was also observed that the vulnerability to IPV is also significantly associated with the socioeconomic status of the PLWHA (P = .007), which has been supported by another research by Silverman et al which says that IPV was more common in less educated and poorer women. 30
We couldn’t find any significant association between QOL, depression, and IPV exposure. This can be attributed to a smaller sample size in our study. Apart from a smaller sample size, our study also had another limitation, that is, since it is being a facility-based study, generalization to other settings may not be feasible. Nonetheless, our study did report on significant issues related to IPV among PLWHA, which can add to the available evidence in general.
Conclusion
Based on our observations, we can conclude that IPV has taken a toll on a significant number of participants, has its effect on the CD4 count, and is related to the socioeconomic status of the women. Although we couldn’t find much significant association between IPV exposure, QOL, depression, and adherence to ART, clear impact of IPV on QOL and mental health of the participants was evident. Thus, IPV is a major issue among PLWHA and hence should be taken as a major factor in the delivery of health services to PLWHA.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Indian Council of Medical Research (ICMR) as part of the ICMR Short Term Studentship (STS) exercise.