
Abstract
The study was conducted to evaluate the prevalence of nasal colonization of Staphylococcus aureus in individuals with HIV infection attending the Integrated Counselling and Testing Centre in a teaching hospital and compare the prevalence with HIV-uninfected individuals. A case–control study was conducted among newly diagnosed HIV-infected individuals and an equal number of age-group and sex-matched HIV-uninfected individuals, and nasal swabs were collected from both the samples. Sociodemographic and clinical data were collected through individual interviews. Ethical aspects were respected. A total of 100 individuals participated in the study, and 22 (44%) of the 50 HIV-infected cases were colonized by S aureus, including 19 (86.4%) methicillin-sensitive S aureus (MSSA) and 3 (13.6%) methicillin-resistant S aureus (MRSA). Only 12 (24%) strains were isolated from 50 HIV-uninfected individuals, with 11 being MSSA and 1 being MRSA. This difference in the isolation rate was statistically significant (P = .035). The 2 most commonly encountered risk factors in both the groups appeared to be history of tuberculosis and history of surgical procedures but none being statistically significant (P = .093 and P = .996). All the strains of S aureus were sensitive to mupirocin. The study concluded that HIV-infected individuals are at a higher risk of carriage as compared to HIV-uninfected individuals. By eliminating carriage in immunocompromised individuals, infections due to S aureus can also be minimized.
Introduction
The relationship between colonization with Staphylococcus aureus and HIV infection is of particular interest due to the morbidity and mortality associated with staphylococcal infections in HIV-infected patients. 1 Despite multiple reports on the severity and recurrent nature of S aureus infection, 2 the factors predisposing HIV-infected patients to S aureus infection do not appear to have been well studied.
The growing number of patients infected with HIV warrants more studies to establish the importance of nasal carriage for the development of infection. Furthermore, the underlying mechanism of increased carriage in this group of patients remains to be elucidated. It has been pointed out that defining the risk factors for S aureus infection in patients with HIV infection is needed so that high-risk patients who may benefit from preventive strategies can be identified. 3
Staphylococcus aureus is one of the most versatile human pathogens and is notoriously virulent. It has the ability to acquire antimicrobial resistance easily, making treatment difficult. It is in this context that we now view methicillin-resistant S aureus (MRSA) as a worldwide phenomenon. 4 Methicillin-resistant S aureus was first reported in 1960s, and it started to establish itself as a nosocomial pathogen with increasing prevalence rates among hospitals nationally and worldwide. 5,6 Originally associated with health care acquired infections, MRSA began to be recognized as an important cause of community acquired infections in late 1990s. 7 Methicillin-resistant S aureus has thus established itself as a heterogenous group of organisms with different epidemic potentials resulting in its constantly evolving epidemiology. HIV-infected patients are now recognized as one of these higher risk groups due to the increased rates of both MRSA colonization and infections over the past decade. The organism’s interactions and disease manifestations in the immunocompromised host are expected to be complex and diverse as the epidemiology of MRSA and HIV continues to change over time.
We report the incidence of nasal carriage of S aureus and MRSA among the HIV-infected and HIV-uninfected individuals in the community and elicit various risk factors that would lead to increased carriage in these high-risk patients. Also by eliminating the carriage in these groups, we can decrease the incidence of staphylococcal infections anywhere in the body.
Study Design
The present study is a case–control study enrolling 50 newly diagnosed HIV-infected individuals and an equal number of age-group and sex-matched HIV-uninfected individuals attending the Integrated Counselling and Testing Centre of a tertiary hospital during the period of January to December 2010. This research project was considered and approved by the research ethics committee of the hospital.
The inclusion criteria established included individuals between 20 to 50 years of age and those with laboratory confirmed HIV positivity. Those excluded from the study were younger than 20 years and older than 50 years of age, patients clinically suspected to have active tuberculosis, those on antiretroviral therapy, and who had a history of application of topical mupirocin in the anterior nares in the last 2 weeks.
Study Procedures
Those who participated in the study received information referring to the study objectives and the research’s ethical aspects; and once the individual had understood and accepted to participate, he or she signed the informed consent. Sociodemographic, clinical, and behavioral data were collected through individual interviews in a structured proforma. The nasal secretion was obtained using self-made cotton swabs, these being rubbed lightly in the left and right anterior nares of every study participant. All aseptic precautions were observed while collecting the specimens and were immediately transported to the department of microbiology and processed.
Laboratory Identification and Antimicrobial Susceptibility
One of the swabs collected from the nares was inoculated in a selective mannitol salt broth, and the other was inoculated onto 5% sheep blood agar and MacConkey’s agar as well. The plates and the broth were incubated aerobically at 37°C. After overnight incubation, the plates were read. Subcultures were made from the mannitol salt broth onto 5% sheep blood agar and MacConkey’s medium and incubated again at 37°C and read the following day. Hemolytic 1-mm colony on blood agar was confirmed as S aureus by tube coagulase and anaerobic mannitol test. All the isolated strains of S aureus were also tested for methicillin resistance by the cefoxitin disc method as recommended by Clinical Laboratory Standards Institute. 8 Cefoxitin-resistant S aureus were confirmed as MRSA by VITEK 2 system (BioMerieux Inc, France). Further antimicrobial susceptibility pattern of all the strains of S aureus including MRSA was determined using the disc diffusion method by employing the modified Stokes technique 10 as follows: penicillin (10 IU), cephalexin, cefazolin, clindamycin (2 µg), erythromycin (15 µg), ofloxacin (5 µg), ciprofloxacin (5 µg), amikacin (30 µg), gentamicin (10 µg), netilmicin (30 µg), tobramycin (10 µg), framycetin (100 µg), isepamycin (30 µg), fusidic acid (10 µg), chloramphenicol (5 µg), rifampicin (5 µg), cotrimoxazole (1.25/23.75 µg), tetracycline (30 µg), vancomycin (30 µg), teicoplanin (30 µg), and linezolid (30 µg).
The minimum inhibitory concentrations (MICs) of mupirocin, for all isolates of S aureus, were determined by the E-test (AB-Biodisk Solna, Sweden). Standard control strains of S aureus NCTC 6571 was used as the reference strain.
Phage Typing
All the strains of S aureus were phage typed by using the conventional set of phages as described by Blair and Williams. 9 Phage typing was done at the National Phage Typing Centre, Maulana Azad Medical College, New Delhi, India. The propagating strain was first subcultured onto a blood agar plate. A single colony was picked up, and the phage pattern was checked using the 23 phages of the basic set at 1 and 100 routine test dilution (RTD). Strains that were nontypable at 1 RTD were typed at 100 RTD.
Phage typing using supplementary MRSA phages
All MRSA strains were additionally phage typed using 9 supplementary phages. The 9 phages used were M3, M5, M12, M8, MR25, 622, C30, C33, and C38.
Statistical Analysis
The data were organized in Microsoft Office and Mac Excel 2011 spreadsheets and then exported to the Statistical Package for the Social Science program, version 17.0. All the qualitative data were compared using the chi-square test or the Fisher exact test. On the other hand, all quantitative data were compared using t test or nonparametric Mann-Whitney test.
Result
A total of 100 individuals (50 HIV infected and 50 HIV uninfected) participated in the study. The mean age of the HIV-unfected group was 33.96 ± 8.471 (50, 18) and of the HIV-uninfected group was 33.78 ± 7.965. (48, 20) In both the groups, 18 (36%) participants were female, 31 (62%) were male, and a single (2%) transgender. In relation to education, 20% of the interviewers were illiterate, 26% had completed primary school, 38% had completed high school, 12% completed twelfth standard, and 4% were graduate. In all, 90% of the study participants were married, of which 80% were living with their spouses.
Of the 50 HIV-infected cases, 47 (94%) acquired HIV infection by sexual route, 7 (14%) gave a history of blood transfusion, and only 1 (2%) was intravenous drug (IVD) abuser. None of the cases were acquired by vertical transmission. Of the 50 HIV-infected individuals enrolled in the study, 11 (22%) reported hospitalization in the past, 18 (36%) gave a history of surgical procedure, 16 (32%) had a history of tuberculosis, 12 (24%) were alcoholic, 6 (12%) were smokers, and 7 (14%) had taken antibiotics in the last 3 months. Also, few (9) were taking antibiotics at the time of sampling, 1 was diabetic, 3 had dermatitis, and 3 had a history of sexually transmitted disease (Table 1). Of the study participants, 4 (8%) were men having sex with men (MSM). The mean CD4 count of the HIV-infected cases was 231 ± 192.126 (926, 12). Seventy-six percent of the patients had a CD4 count of less than cells/mm3.
Total Cases with Various Risk Factors in HIV-Infected and HIV-Uninfected Individuals.
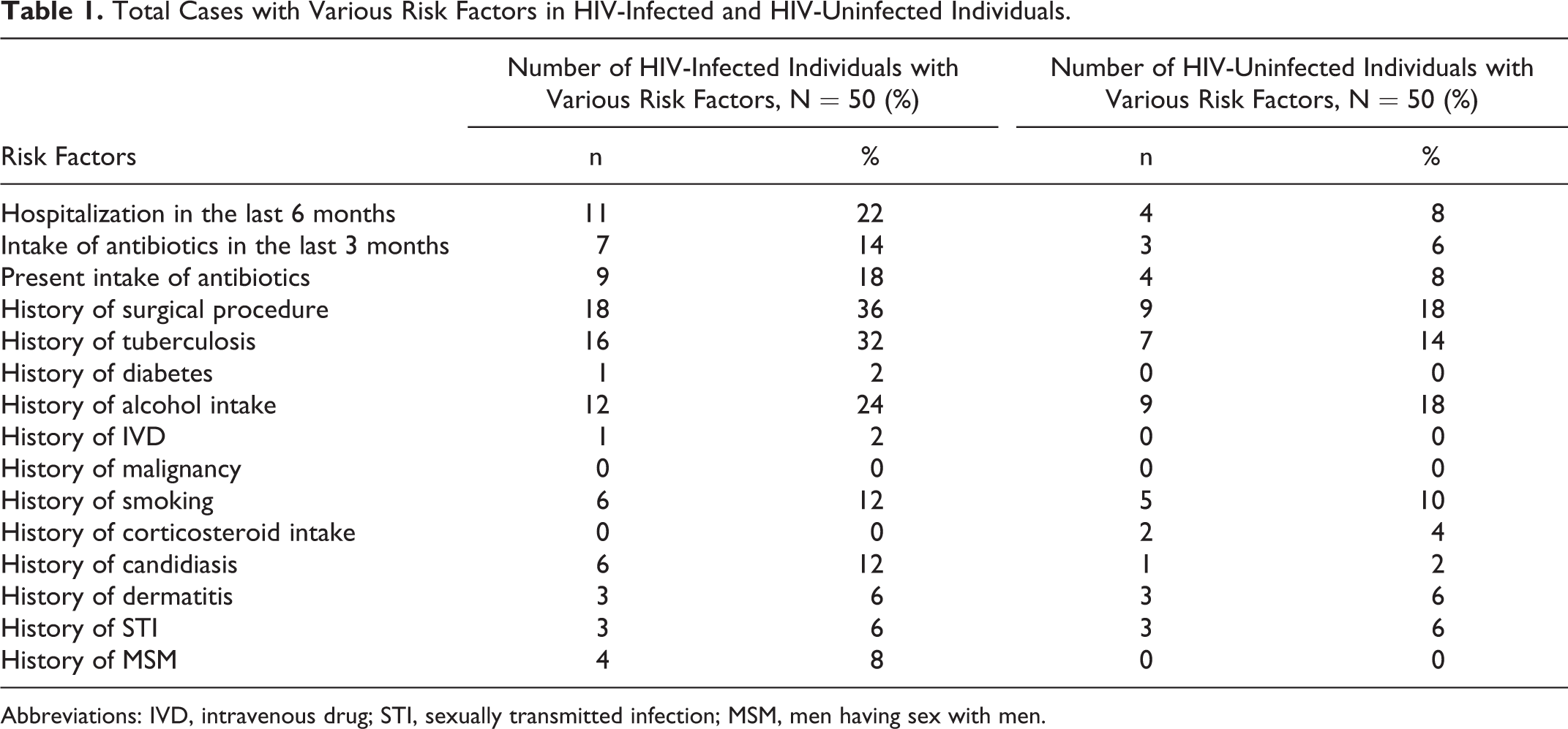
Abbreviations: IVD, intravenous drug; STI, sexually transmitted infection; MSM, men having sex with men.
The microbial analysis of the material resulted in 44% (22 cases) of HIV-infected individuals colonized with S aureus as compared to 24% (12 cases) of the HIV-uninfected individuals. This difference in the isolation rate of S aureus in both the groups was statistically significant (P = .035). Among those who were colonized in the HIV-infected group, 86.4% (19 cases) were sensitive to cefoxitin and are known as methicillin-sensitive S aureus (MSSA) and 3 (13.6%) were resistant to cefoxitin, known as MRSA. In the HIV-noninfected group, only 1 (8.7%) was cefoxitin resistant, that is, MRSA (Table 2).
Isolation Rates of MRSA and MSSA Obtained from Nasal Swabs in HIV-Infected and HIV-uninfected Individuals.

Abbreviations: MRSA, methicillin-resistant Staphylococcus aureus; MSSA, methicillin-sensitive S aureus.
History of tuberculosis (45.45%), history of surgical procedures (40.90%), and history of hospitalization (27.27%) were the most common risk factors associated with nasal colonization in both the groups, but none of the risk factors studied was statistically significant. Other risk factors associated with carriage were intake of antibiotics in the last 3 months (18.18%), history of alcohol intake (13.63%), smoking (9.09%), history of dermatitis (9.09%), and MSM (9.09%). History of mucocutaneous candidiasis (4.54%), sexually transmitted disease (4.54%), and intravenous drug abuse (4.54%) are also associated with carriage (Table 3).
Comparison of Risk Factors for Nasal Carriage of Staphylococcus aureus in HIV-Infected and HIV-Unoninfected Individuals.

Abbreviations: IVD, intravenous drug; STI, sexually transmitted infection; MSM, men having sex with men.
With regard to the type of sexual behavior in the HIV-infected cases from whom nasal swabs grew S aureus, it was found that 18 (90%) individuals were practicing heterosexual activity, and 1 isolate each were reported from individuals practicing homosexual and bisexual activity (Table 4 and B).
Risk Factors for HIV Transmission Seen in HIV-Infected Cases in Whom Staphylococcus aureus Was Isolated from Nasal Swab.a

Abbreviation: IVD, intravenous drug.
an = 22.
Type of sexual behavior in the HIV infected cases whose nasal swabs grew Staphylococcus aureus.

In relation to the HIV viral load, S aureus was isolated from 50% of the cases with a CD4 count <200 cells/mm3, while 22.7% of the cases had a CD4 count >350 cells/mm3. Methicillin-resistant S aureus was identified in 3 (6%) individuals with a CD4 count < 200 cells/mm3 (Table 5).
CD4 Count of the Study Participants with MSSA and MRSA from Nasal Swabs.
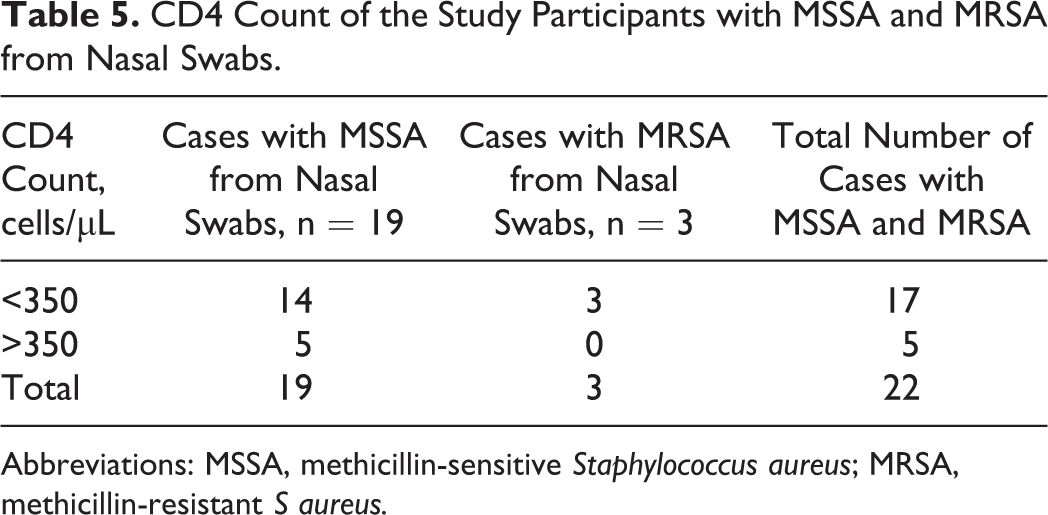
Abbreviations: MSSA, methicillin-sensitive Staphylococcus aureus; MRSA, methicillin-resistant S aureus.
Risk Factors for Nasal Carriage of MRSA in HIV-Infected Individuals
All the 3 cases with MRSA carriage in nares were males. History of surgical procedure (33.33%, P = 1.000), tuberculosis in the past (66.66%, P = .571), alcohol intake (66.66%, P = .038), IVD (33.33%, P = .136), smoking (33.33%, P = .260), and history of mucocutaneous candidiasis (33.33%, P = .136) comprised the various risk factors. All 3 individuals whose nasal swabs yielded MRSA had a CD4 count <200 cell/mm3 (P = 1.000).
Risk Factors for Nasal Carriage of MSSA in HIV-Infected Individuals
MSSA colonization was reported in 36.36% males. Four had a history of hospitalization in the last 6 months and 2 had a history of intake of antibiotics. History of surgical procedures, tuberculosis in the past, diabetes mellitus, alcohol intake, smoking, and dermatitis were the various risk factors for MSSA colonization.
Antibiotic Susceptibility Pattern
The antibiotic resistance pattern of S aureus isolated from the nasal swabs of HIV-infected cases was different from those of HIV-uninfected cases. All the isolates of S aureus from both the groups were resistant to penicillin. A high percentage of strains from the HIV-infected cases showed resistance to erythromycin (27.3%), ofloxacin (45.5%), ciprofloxacin (59.1%), and cotrimoxazole (77.3%). Strains from HIV-uninfected cases were also resistant to the above-mentioned antibiotics, but the percentage resistance found among these groups was much lower—erythromycin (25.0%), ofloxacin (33.3%), ciprofloxacin (33.3%), and cotrimoxazole (50.0%; Figure 1).

Comparison of resistance of Staphylococcus aureus isolates from the nasal swabs of HIV-infected and HIV-uninfected cases.
Since the number of MRSA isolates was so few, it would be futile to attempt to draw any conclusion by comparing the percentages of resistance seen in the MRSA strains isolated from the HIV-infected versus those from the HIV-uninfected cases.
The MIC for mupirocin for all the 34 isolates of S aureus was determined by using the E-test. The MIC ranges, MIC50 and MIC90 values, of the isolates of S aureus (MSSA and MRSA) for mupirocin were <0.064 µg/mL and <0.064 µg/mL, respectively. Of the 34 strains tested from the nasal swab, 33 showed an MIC of <0.064 µg/mL, while a single MSSA strain isolated from the nasal swab of an HIV-infected case had an MIC of 4.0 µg/mL. All the 4 MRSA isolates from nares showed an MIC of <0.064 µg/mL. All the nasal isolates of S aureus were sensitive to mupirocin, hence facilitating nasal carriage of this organism by its topical application. However, all the strains irrespective of their methicillin status were found to be sensitive to the 2 glycopeptides, namely, vancomycin, teicoplanin, and linezolid.
Phage typing
While 90.9% of the isolates from HIV-infected cases were typable, only 33.3% of isolates from HIV-uninfected cases were typable. A high percentage (94.7%) of the MSSA isolates from the nasal swabs of the HIV-infected cases were typable, whereas only 36.4% of the MSSA isolated from nasal swabs of HIV-uninfected cases were typable. Also, the sole MRSA isolate from the uninfected cases was nontypable.
All 4 MRSA when additionally typed using 9 supplementary phages for MRSA were found to be typable (100% typability). The 4 strains that were typable showed 2 different typing patterns, either 622 or 622/C22 phage type.
Discussion
As demonstrated in our study, nasal colonization of S aureus in the HIV-infected group is more than that in the HIV-uninfected group, wherein nasal swabs from HIV-infected cases yielded a higher carriage rate of 44% as compared to HIV-uninfected group (24%). Many published studies among HIV-infected patients showed slightly lower carriage rate than that reported in our study (ie, Nguyen et al 3 [34%], Villacian et al 11 [23%], and McDonald et al 12 [33%]). A sole Indian study reported a much higher rate of isolation (76.67%). 1 In the control group (ie, HIV-uninfected individuals), all the studies 13,15 showed almost similar carriage rate as that of ours, but none of the studies have compared the carriage rate between both the groups.
During 2010, methicillin-resistant S aureus accounted for 13.6% of all our S aureus isolates, which is identical to that reported by McDonald et al. 12 Methicillin-resistant S aureus carriage rate among the HIV-infected group has been known to be increasing every year. A study conducted in 2008 13 found a carriage rate of 10.3%, as compared to a study in 2004 11 which reported an isolation rate as low as 3%. These data collectively demonstrate the increasing trend of MRSA colonization among these HIV-infected groups, without explaining the exact reason for this increasing trend.
Various risk factors that predispose to the colonization included a history of hospitalization in the last 6 months, those with intake of antibiotics in last 3 months, those with history of surgical procedures, and those with a history of tuberculosis showed higher carriage rates of S aureus than their corresponding HIV noninfected counterparts with a similar history. Nevertheless, it may be mentioned that although these carriage rates were more in the HIV-infected group, the difference did not appear to be statistically significant. This comparison does not appear to have been reported by any other worker. However, others have correlated the association of the risk factors in those HIV-infected cases from whom S aureus (MSSA or MRSA) was isolated. Chacko et al 1 also made similar observations and reported that a higher carriage of S aureus was present in those HIV-infected cases with previous history of hospitalization and systemic infections like tuberculosis.
Of the 3 cases from whom MRSA was isolated, 2 had a history of hospitalization and intake of antibiotics in the last 3 months. These findings are similar to those of Villacian et al 11 who observed that previous use of antibiotics and admission to the hospital during the preceding year are the risk factors for nasal colonization of MRSA. Likewise, 1 case with MRSA colonization in the anterior nares gave a history of mucocutaneous candidiasis, which was similar to the finding of Chacko et al 1 and McDonald et al. 12
In our finding, 77.3% of our isolates had a CD4 count <350 cells/μL, and all MRSA isolated from those patients with CD4 count <200 cells/μL were consistent with previous studies. 1,13
McDonald et al 12 observed 12.2% resistance to ofloxacin and Chacko et al 1 observed 41.3% to yet another fluoroquinolone ciprofloxacin, but the present study recorded that the rates of resistance for these 2 agents were much higher at 45.5% and 59.1%, respectively. On the other hand, Chacko et al 1 have reported a resistance rate of 69.57% to cotrimoxazole, while our resistance rate was much higher at 77.3%. We attribute these increased rates of resistance to the wide spread and probably inappropriate use of fluroquinolones and cotrimoxazole in clinical practice as well as a general trend of increased resistance over the years. Surprisingly, only 13.6% of our isolates were resistant to gentamicin, and this finding is somewhat similar to the figure of 10.2% reported by McDonald et al. 12 It was demonstrated both in Chacko et al study 1 and in our study that all isolates are sensitive to vancomycin. Our isolates from HIV-noninfected cases also showed much less resistance as compared to their HIV-infected counterparts, hence much easily treatable compared to HIV-infected isolates.
Eradication of S aureus carriage served 2 purposes, that is, prevention of infection and prevention of transmission. 14 Many techniques have been used to eradicate S aureus from the nares, such as the use of systemic antimicrobials, normal bacterial flora augmentation, antiseptic washes, and topical antimicrobials. For a number of potential reasons, including efficacy and minimization of systemic antibiotic use, topical intranasal therapies have been recognized as a preferred method. 15
Mupirocin has emerged as the topical antibacterial agent of choice for elimination of S aureus nasal carriage. 16 Mupirocin produced by Pseudomonas fluorescens inhibits bacterial protein synthesis by reversibly binding to bacterial isoleucyl-tRNA synthetase. 17 Significant potential exists for mupirocin, as an agent to reduce nasal colonization and subsequent systemic S aureus infection. 18 So we determined the sensitivity of mupirocin so that nasal carriage can be eliminated from these groups of immunocompromised patients. We found that none of the strains of S aureus either from HIV-infected or from HIV-uninfected cases appeared resistant to mupirocin. Our results are significant, since in this study the isolates were all from the anterior nares where topical mupirocin is widely used.
To summarize, HIV-infected individuals are at an increase risk of carriage of S aureus in particular MRSA as compared to HIV-noninfected group. Risk factors for carriage included lower CD4 count, hospitalization in the past, surgical intervention in the past, and history of mucocutaneous candidiasis. All the S aureus strains were sensitive to mupirocin as determined by the MIC, so application of this drug topically can eliminate carriage and subsequently infection anywhere in the body can be eliminated.
Footnotes
Acknowledgments
We acknowledge with gratitude the technical assistance rendered by Shri Ram Prasad and Smt Vijay Arora and also Mrs Prem Lata from National Phage Typing Centre, Department of Microbiology, Maulana Azad Medical College, New Delhi, India.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.