
Abstract
The benign lymphoepithelial lesion is a rare and diagnostically challenging entity. Classically, these lesions present as early manifestation of HIV infection and are rarely seen in those on highly active antiretroviral therapy. We describe 2 rare cases of HIV-associated lympho-epithelial lesions of parotid gland in a 37-year-old female and a 47-year-old male receiving antiretroviral therapy. The lesions were characterized with respect to clinical features, as well as histopathology and radiology findings. Fine-needle aspiration cytology revealed benign squamous epithelium and lymphocytes. Sonographic evaluation of the parotid gland demonstrated intraparotid solid hypoechoic nodule. Computed tomography showed cystic and solid masses. These lesions were diagnosed as benign lymphoepithelial lesions in both cases. To our knowledge, this is the first report in the published literature describing newly occurring benign lymphoepithelial lesions in patients on antiretroviral therapy.
Keywords
Introduction
The benign lymphoepithelial lesions (BLLs) of major salivary glands, particularly of parotid glands, are rare disorders affecting HIV-infected patients and are also associated with Sjögren syndrome. 1,2 These lesions usually develop as an early manifestation of HIV infection, 3 with an incidence of 3%. 4 Sometimes BLL represents initial manifestation of the HIV infection. Benign lymphoepithelial lesions occur in salivary glands and their lymph nodes, but have also been described in the oral cavity, tonsil, thyroid gland, and pancreas. 5 Histologically, HIV-associated BLLs are typified by lymphoid hyperplasia in combination with an epithelial component, as well as cystic and proliferative changes, together with the formation of lymphoepithelial islands. 6 Clinically, patients with parotid BLL typically present with painless bilateral parotid swelling. 7 Parotid BLL rarely involves the facial nerve and can cause gross facial deformities. 8 These lesions occur in both adults and children, equally affecting males and females. 8 The association of BLL with HIV was first reported in 1985. Since that time, the incidence of BLL has been significantly reduced with the increased use of highly active antiretroviral therapy (HAART). Thus, it is unusual to see these lesions in those patients on HAART. 7 This article describes 2 cases of BLL, which were confirmed using histopatholology and radiology findings. Both cases of BLL were diagnosed in HIV-positive patients receiving HAART.
Case Reports
Case 1
A 37-year-old female with a history of HIV and Hodgkin lymphoma presented with right sided facial swelling of 4 days. She complained of pain with swallowing but denied any fevers, chills, or shortness of breath. Her past medical history was significant for right sided cervical lymph node resection with radiation secondary to her Hodgkin lymphoma. Upon examination there was nonerythematous but tender edema inferior to her right maxillary sinus extending to her submandibular region with sublingual lymphadenopathy. The right facial nerve was intact. She reported adherence to antiretroviral therapy. At the time of presentation her CD4 lymphocytes count was 361 cells/mm3. An immunoglobulin M mumps titer was negative.
Case 2
A 47-year-old male with a history of HIV/AIDS with a mycobacterium avium complex (MAC) infection presented with right sided jaw mass for 2 months. He reported the mass fluctuated in size and had become larger compared to when he first noticed it. He reported nonradiating pain when chewing that resolved with rest. Upon examination, he was febrile at 38.5°C. A 2- to 3-cm mass over his right parotid gland region was noted along with right tender submandibular and anterior cervical lymphadenopathy. Right facial nerve was intact. At the time of presentation, he was being treated for MAC infection. The CD4 count was 25 cells/mm3. Both patients were initially thought to have an infectious process but failed to respond to multiple antibiotics.
Histopathology Findings
Case 1
The patient underwent an ultrasound-guided fine-needle aspiration of hypoechoic intraparotid mass. The cytologic samples yielded a small amount of fluid accompanied by a dense lymphoid infiltrate (Figure 1) and benign squamous cells suggesting a cystic lesion lined by squamous epithelium. Malignant cells were not identified. The fine-needle aspiration cytology (FNAC) features that have been reported for HIV-associated BLL include squamous cells, lymphocytes, and foamy macrophages. 6 Histology findings of our case were consistent with those in the published literature.

Radiology Findings
Case 1
Ultrasonographic (US) evaluation of the right parotid gland demonstrated 1.3 × 1 × 0.9 cm intraparotid solid hypoechoic nodule. Reports in the literature suggest that these lesions typically appear as prominent round hypoechoic areas, ranging from 0.5 to 5 cm in diameter, with well circumscribed margins, internal septations, and posterior acoustic enhancement. 8,9
Multiple computed tomography (CT) images of the neck from the thoracic inlet to the skull base were obtained for further investigation to include surveillance for reoccurrence of her Hodgkin lymphoma. Computed tomography demonstrated peripherally enhancing cystic structure within the right parotid gland measuring 1.2 cm in diameter (Figure 2A). There was no lymphadenopathy or focal soft tissue mass. The submandibular glands were preserved.
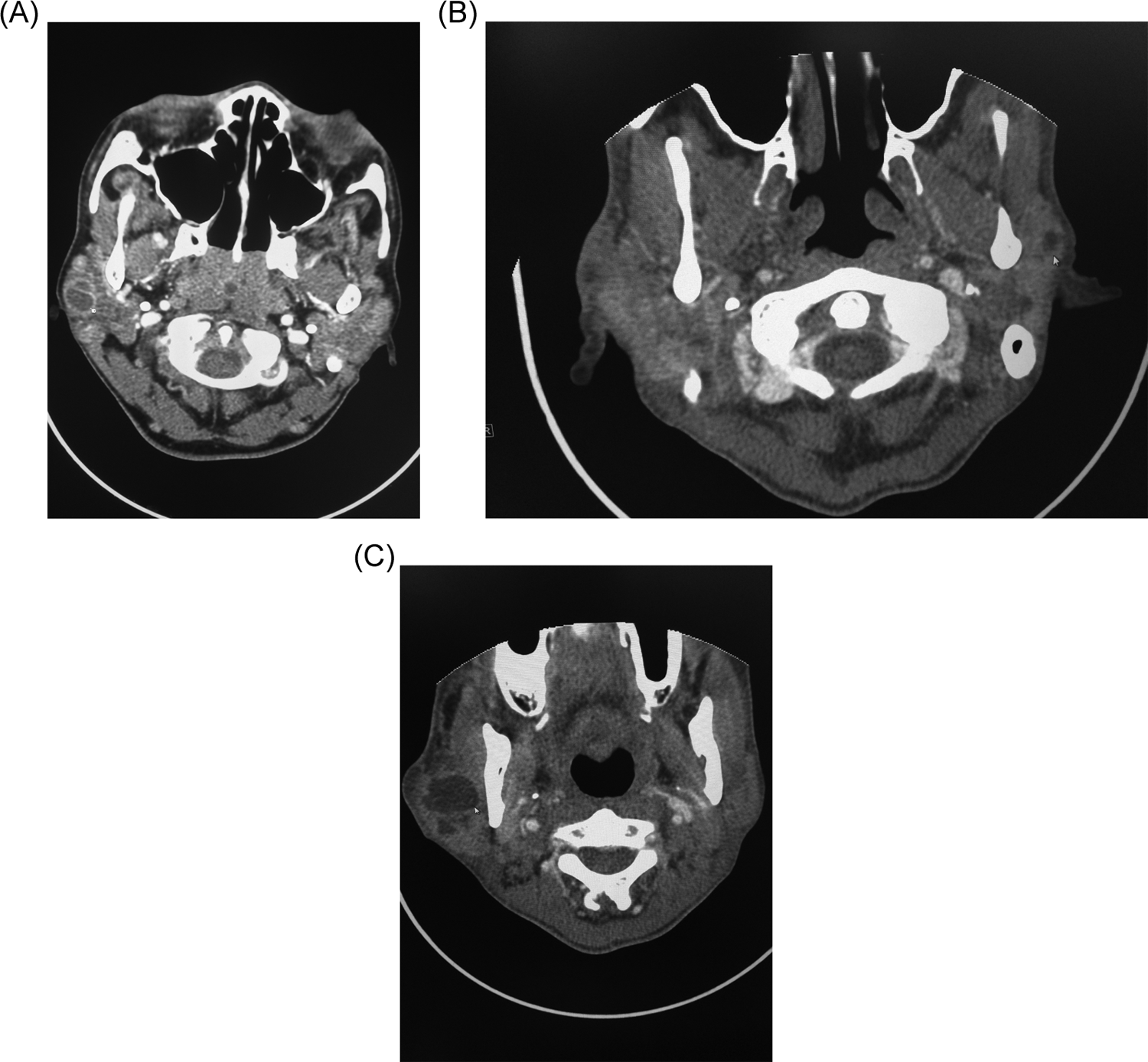
Contrast-enhanced computed tomography (CT) images of the neck show a well-defined cystic lesion in the right parotid gland of patient 1 (
Case 2
A CT scan with contrast revealed multiple, well circumscribed bilateral cystic and possible solid masses, with the largest masses measuring 2.4 and 1.1 cm in diameter within the right and left parotid glands, respectively (Figure 2B and C). The thin-rim enhancement of the cystic lesions was appreciated. There was good flow within the regional vasculature with no evidence of venous thrombosis. Anterior and posterior lymphadenopathy was noted. The largest lymph node, measuring 2.6 cm in diameter, was identified adjacent to the left jugular vein at the level of the larynx. Computed tomography findings reported in the published literature usually reveal multiple small cysts with enlarged parotid glands. Computed tomography can demonstrate cervical lymphadenopathy in 100% of cases. 8,10,11 The imaging findings for both cases are in agreement with those described in the published literature.
Discussion
HIV-associated BLL are very uncommon, often resulting in diagnostic difficulties. For cases presented, the differential diagnosis initially favored infectious process or malignancy due to both rarity of this condition and immunodeficient status of the patients. Until early 1980s, BLLs were considered a rare manifestation of Sjögren syndrome, while later studies showed a strict predilection of these parotid lesions for HIV-positive patients. 12 It has also been reported that sometimes BLL represents initial manifestation of the HIV infection, 13 thus encouraging physicians to administer an HIV test to a patient who presents with parotid swelling and whose HIV status is unknown. Although association of BLL with HIV was first reported by Ryan in 1985, histopathogenesis of parotid BLL still remains unclear. One suggested mechanism of BLL formation states that HIV-related reactive lymphoproliferation occurs in the lymph nodes of the parotid gland, resulting in the entrapment of the parotid glandular epithelium in normal intraparotid lymph nodes, and ultimately leading to cystic enlargement. Advocates of alternative, obstructive theory of BLL formation suggest that ductal obstruction by lymphoid proliferation might lead to ductal dilation that mimics a true cyst. 8
The diagnosis in the first case was reached by employing a combination of clinical findings, FNAC, US and CT with contrast. Case 2 diagnosis was established based on clinical and CT findings. Several studies demonstrated that CT findings of single and/or multiple parotid cysts and cervical adenopathy were sufficient for BLL diagnosis. 8
Parotid BLLs need to be distinguished clinically and pathologically from the lymphoepithelial sialadenitis of Sjögren syndrome, Warthin tumor, and Hodgkin lymphoma. This was particularly important for the first case given the patient’s prior history of Hodgkin lymphoma. Benign lymphoepithelial lesions can readily be distinguished by the characteristic triad of squamous cells, lymphocytes, and foamy macrophages while Hodgkin lymphoma is confirmed by typical Reed-Sternberg cells or atypical mononuclear Hodgkin cells with lymphocytes, eosinophils, plasma cells, and histiocytes. 14,15 Although Warthin tumor clinical presentation—unilateral, painless, firm, circumscribed cystic masses—is similar to that of BLL, histopathologically it is characterized by bilayered cuboidal, columnar, or oncocytic ductal epithelium. Furthermore, Warthin tumor is not associated with cervical lymphadenopathy, which is a prevalent finding in BLL. 14,15 Lymphoepithelial sialadenitis is a component of autoimmune Sjögren syndrome. It is characterized by lymphocytic infiltrate of salivary gland with parenchymal atrophy and foci of ductal hyperplasia with lymphocytic epitheliotropism. Also, features of Sjögren syndrome include xerostomia and serum autoantibodies like anti-Sjögren’s-syndrome-related antigen A (anti-SSA) and anti-Sjögren’s-syndrome-related antigen B (anti-SSB). 15
As mentioned above, BLLs are rare. Furthermore, it is exceedingly uncommon to find BLL in patients receiving HAART. Remarkably, the cases discussed were patients receiving HAART at the time of presentation with the lymphoepithelial lesions. To our knowledge, this is the first report in the published literature describing newly occurring BLLs in patients on HAART. In fact, HAART is one of the treatment options available for patients with BLL, along with repeated fine-needle aspiration and drainage, surgery, radiotherapy, and sclerotherapy. 16,17 Observation is an accepted alternative if the patient is asymptomatic or chooses to not undergo treatment. Multiple studies have reported that parotid gland swelling was completely reduced to a fraction of their initial size upon administration of HAART in children and adults. 18 -20 Although it has been widely accepted that HAART targets the origin of BLL, the HIV infection, the mechanism of HAART’s action on BLL seems to be multifactorial. It is recognized that HAART increases the CD4 count and decreases the blood viral load. 21 Also, it has been shown that HAART decreases the diffuse infiltrative lymphocytosis syndrome (DILS), 22 which might correlate with obstructive theory of BLL formation, whereas the diminution of DILS owing to HAART might subsequently lead to the reopening of previously obstructed salivary gland ducts and resolution of the BLL. 18 Given the findings of BLL in the setting of HAART, the obstructive theory mechanism is not the case for these 2 patients. Thus, it seems plausible that HIV-related lymphoproliferation mechanism is responsible for the BLL in the presented cases or the 2 mechanisms occur concurrently.
In summary, the cases presented illustrate rare examples of HIV-associated BLL in the setting of HAART. Given the rarity of this condition, it is important to keep this entity in the differential diagnosis when working up parotid swelling in HIV-positive patients receiving HAART.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.