
Abstract
Data are lacking on factors that may impact conception-related decision-making among individuals living with HIV. This study’s aim was to shed light on these considerations. Participants were invited to complete a survey on preconception considerations. A rank-ordered logit model was fit to estimate the relative importance of listed consideration factors; the interaction of HIV status and the factors was assessed. Fifty-nine participants living with HIV and 18 partners (11 HIV-negative participants and 7 living with HIV) were included. Risk of vertical and horizontal HIV transmission and the effect of antiretroviral therapy on the fetus were the top considerations. However, individuals living with HIV prioritized vertical transmission, whereas HIV-negative participants prioritized horizontal transmission. Other factors of importance were probability of conception, stress of trying to conceive, cost associated with fertility clinics, and stigma associated with certain conception methods. This study builds our understanding of the preconception considerations for people living with HIV.
Introduction
Many people living with HIV, who at one time might not have considered pregnancy for fear of transmission, lack of medical support, or reprimanding from the medical community and general public, are now planning to start or expand their families. A growing body of literature has demonstrated the need for greater attention to the preconception and pregnancy planning needs of people living with HIV. 1 -5 But questions remain about how reproductive decisions are made by people living with HIV and their partners and how considerations related to their HIV statuses might factor into this decision-making process, particularly when making choices about how to attempt pregnancy. This may be highly relevant in the context of serodiscordant couples and is imperative to explore more fully to better inform clinical support. To allay their fears, and to ensure the appropriate management steps are taken, adequate preconception counseling is needed to support decision-making. 1,2
Prior to landmark studies, such as the HPTN 052 Study, 6 clinicians had insufficient information related to the risk of horizontal HIV transmission in discordant couples and how this could impact conception attempts in the context of HIV. Practitioners were often uncomfortable counseling about potentially risky or harm reduction approaches to conception. 2,7 However, recent studies have provided strong scientific evidence supporting the concept that the risk of horizontal and vertical HIV transmission can almost be eliminated with appropriate antiretroviral measures in the infected partner and have also introduced the potential use of preexposure prophylaxis in the uninfected partner. 6,8 -13
The HIV-positive individuals and couples planning pregnancy have a series of personal considerations. 7,14 One may be the willingness to accept the risk of horizontal HIV transmission in serodiscordant relationships, in order to conceive. 14 Other factors that must be considered include the acceptability and/or financial feasibility of accessing fertility or surrogacy services to reduce the risk of horizontal transmission, as a result of suboptimal fertility, or if a same-sex couple is planning pregnancy. Yet another may relate to personal, familial, and cultural desires for a child 14,15 and apprehensions related to HIV stigma and discrimination experienced by prospective parents living with HIV that has been well documented in the literature for upward of 20 years but persists today. 15 -17 Understanding the preconception needs and desires of people and couples living with HIV is becoming increasingly complex and requires expert clinical counseling informed by solid evidence. 7,18
The purpose of this study was to explore the preconception considerations of individuals and couples living with HIV in Ontario, Canada, especially as it pertains to the choice of potential method of conception. We achieved this through the use of a survey that was developed by the research team to review several decision-making considerations of individuals and couples living with HIV, during the preconception period, which require participants to rank the factors to specifically identify the relative importance of each factor for the participants.
Methods
Study Setting and Participants
Ontario has an estimated 27 000 people living with HIV, 19 among which greater than 80% are of reproductive age. 3,20 Given these numbers and our previous work demonstrating the high pregnancy intention among women with HIV in Ontario, 3 this province was deemed an appropriate site for the current study.
We required preliminary steps to engage community, to explore what was missing in the literature, and to better understand the complexity of the issue of preconception considerations that have been alluded to in previous research.3,7 A community advisory board (CAB), composed primarily of people living with HIV and other stakeholders, was established to assist in the development of the process for the pilot study and the development of the survey instrument. The composition of the CAB reflected the diversity of people living with HIV across Ontario including geography, age, sexual orientation, race/ethnicity, and pregnancy intention. During CAB meetings, potential locations across the province that would enable recruitment of a representative sample of individuals and couples living with HIV who were considering pregnancy were identified. Eighteen final sites were initiated. These included hospitals, community-based and pediatric HIV clinics, gynecology and fertility clinics, and community-based organizations. People living with HIV, with or without their partners, who were considering pregnancy were recruited by local research coordinators or site personnel.
The aim of this study was to recruit 60 individuals living with HIV, with or without their partners, from across Ontario. A sample size of 60 was chosen based on the literature and some specific considerations for this project. 21 -23 As it was hypothesized that one-third of the participants would enroll with a partner, we also wanted to ensure a sufficient sample size of partners.
Inclusion criteria included individuals ≥18 years of age, living with HIV, and who were residing in Ontario and considering pregnancy in the next 6 months. When couples were recruited, at least 1 partner needed to be living with HIV. Exclusion criteria focused on those individuals with advanced medical issues, who could not read and write English or French, or who could not provide informed consent. Participants were enrolled from February 1, 2012, to June 30, 2013, from 11 of the study sites.
Ethical Considerations and Study Visits
Research ethics approval was obtained from Women’s College Hospital Research Ethics Board (reference number: 2010-0014-B), and institutional approval was obtained from all additional study sites that required it. Individuals who consented to participate were invited to attend 2 study visits. While the data collection was intended to be administered by the interviewer, participants were also given the option of completing any part of the data collection on their own due to the sensitive nature of the questions. The average length of the first study visit was 90 minutes. At the end of the first visit, participants were provided with educational materials on pregnancy planning and HIV. The second visit was designed for the participants to provide feedback on the educational materials (these results are not reported in this article) and lasted approximately 30 minutes.
Survey Instrument Development
Data pertaining to preconception considerations were collected using the Pre-Conception Consideration Assessment (PreCCA) Survey (available upon request), which was developed in collaboration with the CAB as no existing survey could be located for adaptation. The PreCCA survey is a 43-primary-item instrument and uses questions from previously validated scales when possible, including the Ontario HIV Fertility Survey. 3 Survey completion ranged from 25 to 45 minutes on average. Six principle domains were identified via a yearlong, community-based consultation process and were included in the PreCCA survey. These domains were: (1) desire and intention for pregnancy, (2) stress related to conception and accessing fertility services, (3) stigma associated with conception, (4) awareness of available services, (5) service utilization, and (6) reproductive decision-making.
The questionnaire was developed in English and translated into French using backward translation methodology. Content validity was achieved by using previously validated questions when possible, conducting an extensive literature review, and consulting the CAB during development. Face validity was achieved by pilot testing the PreCCA survey (prior to enrolment) with 5 people living with HIV who were considering pregnancy. The pilot participants confirmed that the PreCCA survey appeared to be measuring the intended items related to the domains. Participants were also asked to comment on each item in terms of comprehension, clarity, and relevance. Initial piloting of the PreCCA survey resulted in minor changes, and the revised survey was retested with the same participants with no additional revisions. The objective of the PreCCA survey was to focus on the considerations during the preconception period and specifically the considerations that are most relevant to people with HIV and their partners, particularly as it related to the choice of method of conception. To achieve this, the PreCCA survey contains a series of questions that ask participants to rank considerations and preference. The ranking process was explained to all participants by the interviewer to ensure comprehension.
Data Analysis
Survey data were entered twice and verified prior to analysis. Statistical analyses were performed using statistical software Stata version 12 (StataCorp, College Station, Texas). Baseline characteristics of the study population were summarized using medians and interquartile ranges (IQRs) for continuous variables and frequencies and proportions for categorical variables.
The primary statistical analysis was intended to identify and rank the factors that were considered important by both people living with HIV and their partners in the preconception period and to subsequently determine the relative importance of each factor. This was measured by 1 question in the PreCAA survey that asked the participants to select and rank in order of importance, all factors that they were taking or had taken into consideration when planning for pregnancy. The factors included were those decided upon by the CAB and during piloting and included (1) risk of vertical HIV transmission, (2) risk of horizontal HIV transmission/superinfection, (3) effect of antiretroviral therapy (ART) on the fetus, (4) probability of conception, (5) travel time to access fertility services, (6) stress, and (7) cost associated with accessing fertility clinics, (8) stress of trying to conceive, and (9) stigma associated with certain conception methods.
A rank-ordered logit regression model was then used to estimate the importance of each factor, including any statistical differences between factors’ importance. The rank of each factor, 1 (highest) to 9 (lowest), was determined based on the estimated weight from the rank-ordered logit model. Exploring differences between each factor’s importance and HIV status was achieved using interaction terms of each factor with being HIV negative (ie, factor × HIV negative). This method was used due to the small sample size of HIV-negative partners.
Results
Description of Study Participants
Fifty-nine individuals living with HIV from Ontario who were planning pregnancies were enrolled. An additional 18 partners of the primary participants were enrolled. Of these partner dyads, 11 were serodiscordant and 7 were seroconcordant. Table 1 summarizes the demographic characteristics of the cohort. The final study population (total N = 77) had a median age of 35 years (IQR: 33-40), 68% were female, 87% identified as heterosexual, and 58% were of African ethnicity. Forty-seven percent were married, with an additional 35% stating they were in a committed relationship. Sixty-five percent were living in a large urban area. Sixty-four percent of the study population expected to have 2 or more additional children, and an additional 31% expected to have 1 more child.
Sociodemographic Characteristics of Study Participants.a
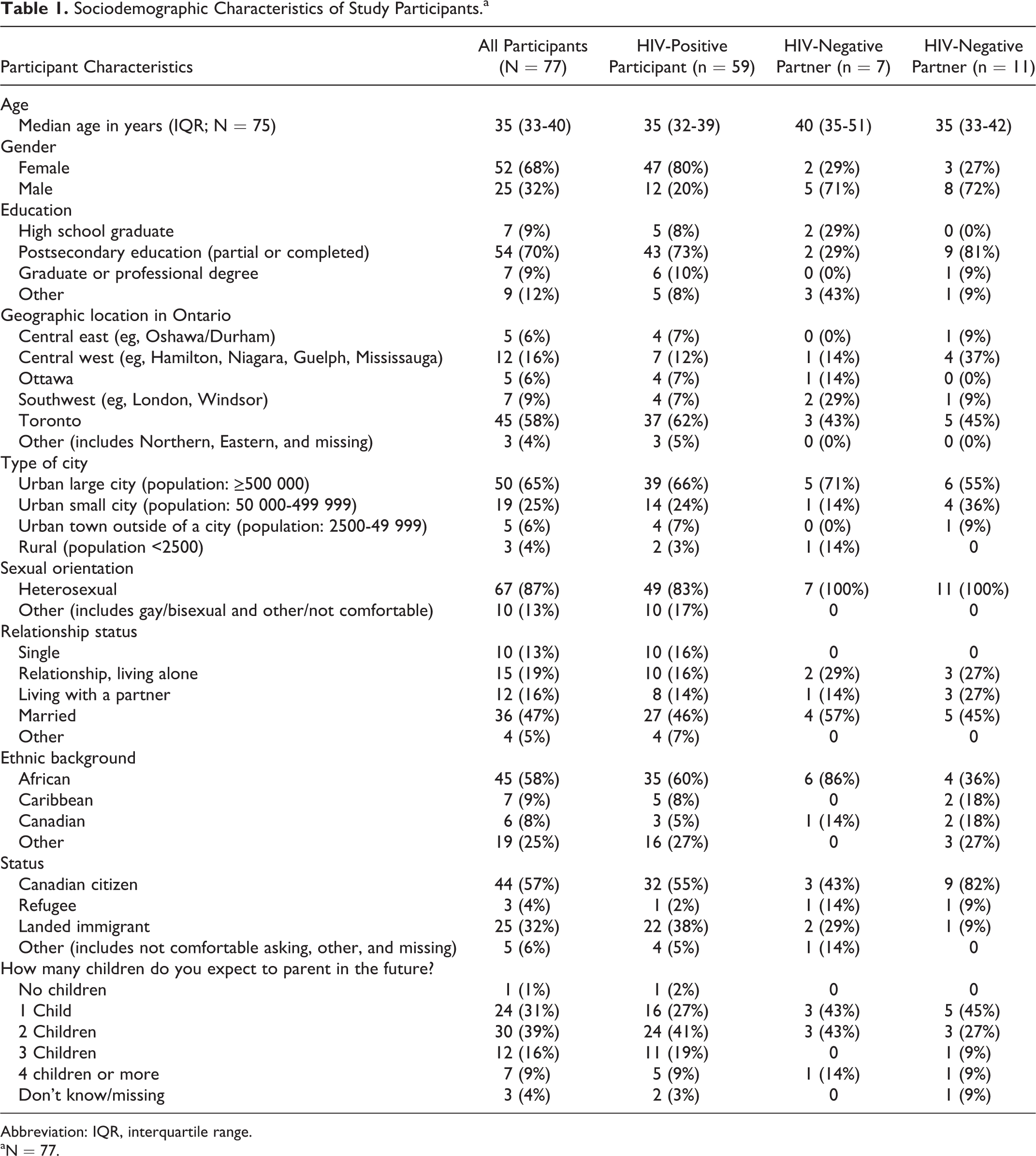
Abbreviation: IQR, interquartile range.
aN = 77.
Preconception Considerations
Among the 66 participants living with HIV, the primary preconception consideration was the probability of vertical HIV transmission, followed by the effect of ART on the fetus during pregnancy (Table 2). Horizontal HIV transmission was the third most important preconception consideration. All subsequent factors were ranked as follows: (4) probability of conception, (5) stress associated with conception, (6) cost of conception, (7 and 8) stigma associated with, and stress of, finding a fertility clinic, and (9) travel time to access fertility services (Table 2).
Summary of Rankings of A Priori Preconception Considerations.
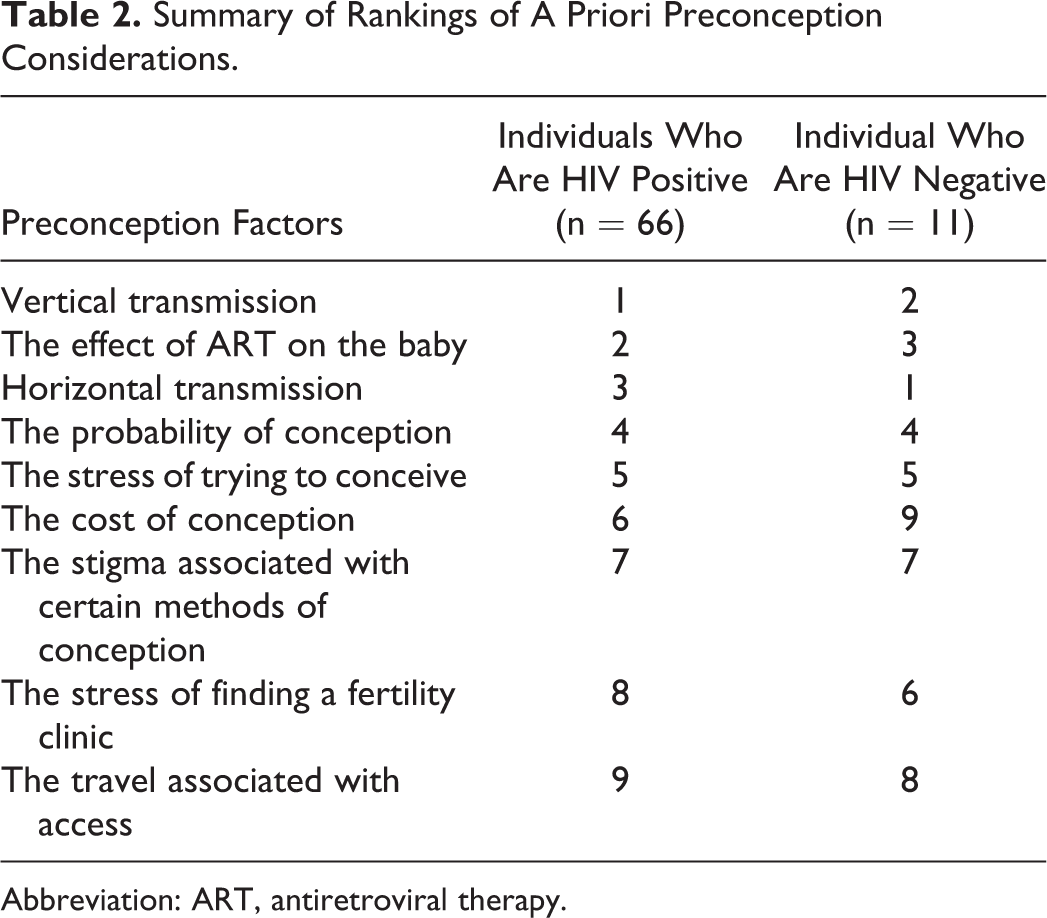
Abbreviation: ART, antiretroviral therapy.
The HIV-negative partners had different ranking results (Table 2). Horizontal HIV transmission was their primary consideration followed by chance of vertical HIV transmission. The effect of ART on the developing fetus was reported as the third most important preconception consideration. The probability of conception and the stress of trying to conceive were ranked fourth and fifth, respectively. The remaining factors were ranked sixth through ninth as follows: stress of finding a fertility clinic, stigma associated with certain methods of conception, travel time associated with, and cost of, accessing fertility services. Table 2 shows the comparative results for the relative ranking of all preestablished considerations.
Rank-Ordered Logit Model
The results from the rank-ordered logit regression analysis can be found in Table 3. The mean weight of each factor is relative to the reference category of travel time to clinic, as travel time to clinic was consistently ranked low (by implication, travel time to clinic has a “0” weight). The factors of vertical transmission (2.13; 95% confidence interval [CI]: 1.56-2.69), the effect of ART on the baby (1.81; 95% CI: 1.25-2.37), horizontal transmission (1.54; 95% CI: 0.97-2.11), probability of conception (1.35; 95% CI: 0.79-1.91), stress of trying to conceive (1.07; 95% CI: 0.51-1.62), and cost of the procedures (1.03; 95% CI: 0.45-1.55) were determined to be statistically significantly different from zero for the entire cohort of 77 participants. This finding suggests that of the factors included in the PreCCA survey, these factors were of greatest importance to study participants. The remaining factors (stress of trying to conceive, stress of finding a fertility clinic, and stigma associated with certain methods of conception) were not significantly different from zero.
Regression Analysis of Preconception Considerations.
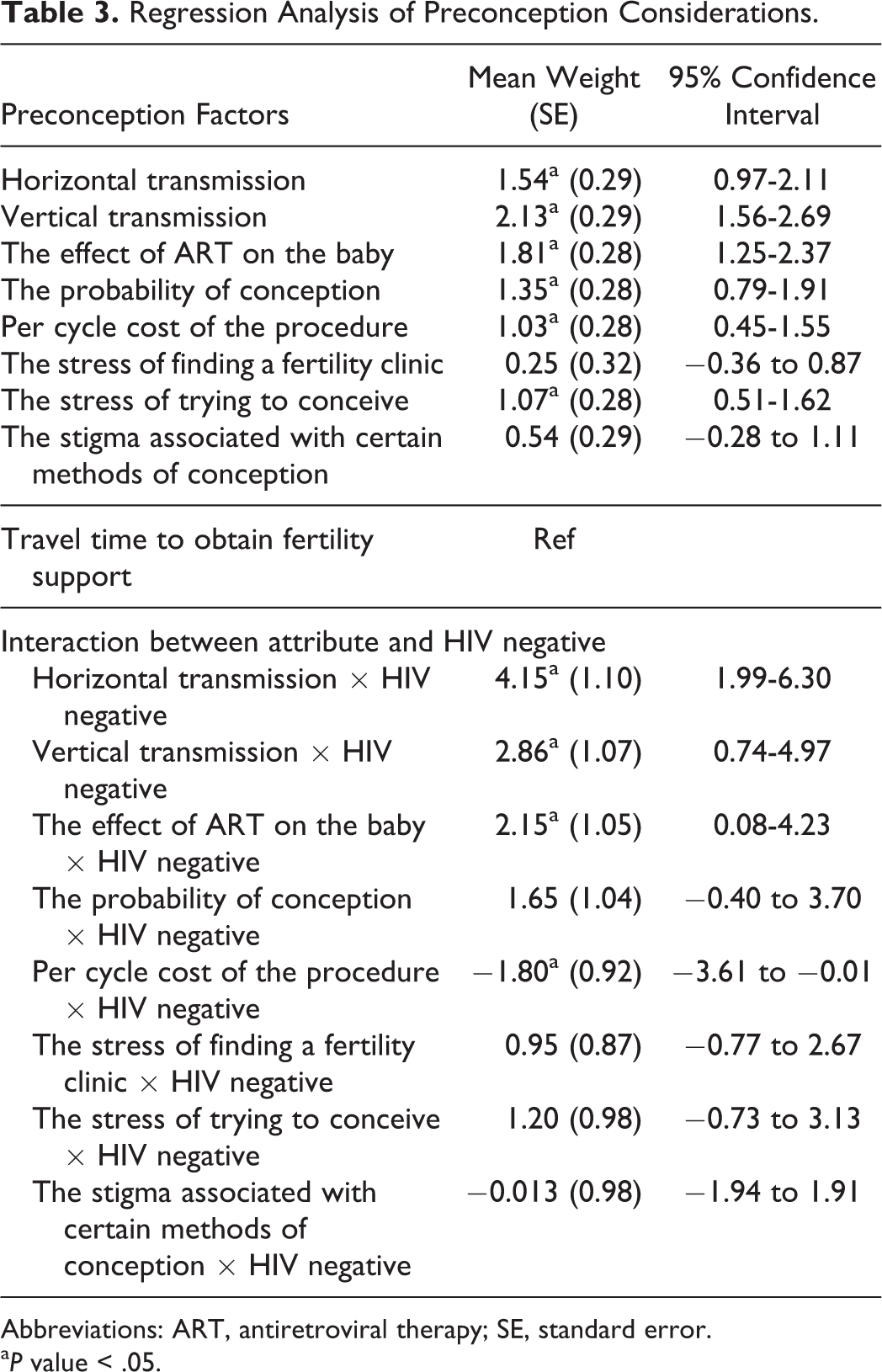
Abbreviations: ART, antiretroviral therapy; SE, standard error.
a P value < .05.
An interaction term was used with HIV-negative status to determine whether any difference could be detected based on serostatus. The interaction item yielded statistically significant results for the following preconception considerations—horizontal transmission (4.15; 95% CI: 1.99-6.30), vertical transmission (2.86; 95% CI: 0.74-4.97), the effect of ART on the baby (2.15; 95% CI; 0.08-4.23), and cost of the procedures (−1.80; 95% CI: −3.61 to −0.01). This indicates that HIV-negative participants had different importance weights for these variables when compared to the individuals who were living with HIV. Differences in other factors did not reach statistical significance.
Discussion
We have found that individuals and couples living with HIV who are planning pregnancies take many factors into account when making their decisions. With research suggesting that counseling in this area is lacking, 7,18,24,25 we assert that understanding these factors is important for optimal clinical counseling and ultimately optimal pregnancy planning outcomes. The risk of HIV transmission (vertical and horizontal) and effect of ART on the fetus were the top 3 considerations among all participants, although the order differed between individuals living with HIV and HIV-negative participants. In the simplest sense, one can postulate that the differences based on serostatus are predictable: one’s identity as a person living with HIV becomes so defining that any decision-making process will be influenced by the knowledge and experience that goes along with this identity. It follows then, that even the partner of a person living with HIV may look at factors and considerations differently than a person himself or herself living with HIV.
Some of the differences may require deeper consideration for how clinical care is provided. One explanation for the difference in the top 3 rankings between the 2 subgroups may be that the participants living with HIV are better informed of the low risk of horizontal HIV transmission during conception attempts, even condomless sex when the partner living with HIV is fully suppressed on combination ART. 6,10,25 It is conceivable that the HIV-negative partners have been inadequately counseled on issues related to HIV. Alternatively, the persistent stigmatization and ongoing medical challenges associated with HIV may continue to fuel fear of transmission among HIV-negative people. Simply put, it is likely that HIV-negative partners are worried about HIV acquisition, and thus their ranking of this factor is higher.
The finding that vertical HIV transmission is the primary consideration for people living with HIV is well supported by previous literature. 26 -30 However, with the near zero risk of vertical transmission afforded by modern HIV treatment, as clinicians, our awareness of these persistent fears may be lacking, leading to possible limitations in how we counsel and support in the current area of ART. This finding alone warrants further investigation using different research methodologies, such as a qualitative design, to better understand how clinicians can continue to support families regarding these fears and how best we can design interventions to address them.
That both subgroups considered the effect of ART on the fetus suggests that individuals and couples living with HIV have inadequate knowledge of the safety of ART use in pregnancy, which in turn may reflect a lack of focus on this topic during preconception counseling. Informal information sharing may also be taking place at a community level that clinicians are unaware of. Alternatively, it may be that despite the growing safety and efficacy data on ART use in pregnancy, individuals and couples are leery of medication use in pregnancy in general and of possible side effects of ART that have yet to be scientifically identified and that remain classified as category B. 25 It is also essential that discussions of ART use in pregnancy are contextualized in the larger social discourses about medication use in pregnancy. Many pregnant women, and their partners, are hesitant to use any medication in pregnancy, 31,32 and discussions of the safety of food and caffeine are increasingly common as well. 33,34 So while the consideration of ART may be unique to HIV, this may also partially be a reflection of a more generalized concern experienced by a pregnant woman and her partner about her body.
Previously, the literature regarding pregnancy planning for people living with HIV in serodiscordant relationships did not focus on the primary concerns of the HIV-negative partner in-depth. In our simple ranking, the HIV-negative participants prioritized different considerations than their partners who were living with HIV, which is an important contribution to the literature. These differences in preconception considerations were quantified in our logit model, which offers a more nuanced understanding of how decision-making in the preconception period is moderated by HIV status. Our findings begin to elucidate the considerable anxiety regarding HIV status, both their own and a future child’s, among HIV-negative partners in serodiscordant relationships. It appears that the complications of transmission, medications, and cost are uniquely experienced depending on HIV status; however, further research is needed to support this conclusively.
In this study, HIV status did partially influence preconception considerations. This draws attention to the need for clinician’s and service providers to assess the need for preconception counseling for all patients and for patients to seek opportunities for counseling when making preconception decisions. It also points to the need to assess the best counseling approach in each situation. For example, while preconception counseling for couples is usually done with both members of the dyad, in serodiscordant couples, some element of individualized counseling might be warranted to create opportunities for open discussion. Counseling strategies to better support the decision-making process for all individuals in couples living with HIV need to be designed carefully with a focus on who should offer the counseling, how to assess the need for counseling, and approaches to counseling that address the unique circumstances and considerations surrounding pregnancy.
There are several important limitations in the study. The sample size was limited, with only 18 partners recruited of which 7 were HIV negative. Therefore, generalizability is limited. The generalizability of these findings are also limited by the sample being mainly heterosexual individuals or couples, and, therefore, there is limited applicability to same-gendered couples.
In this study, we hoped to yield some insight into the preconception considerations of people living with HIV and their partners. In this study, identifying the unique considerations of people living with HIV and HIV-negative partners of people living with HIV is a significant clinical contribution. Prior to this study, it was not clear that when counseling couples, the care provider must address and allay the individualized considerations and fears of people living with HIV and HIV-negative people. This can be achieved through opportunities for couple-based preconception counseling for couples living with HIV, in addition to individual sessions where personal concerns can be shared openly with a trusted and informed clinician or service provider. Preconception counseling for HIV-negative partners by a provider who is educated in the field of HIV and preconception health can be of high importance, given their concerns related to transmission. In addition, we found that basic knowledge, including transmission risk and the impact of ART on the fetus, appears to need extra counseling and knowledge translation. Comprehensive counseling is imperative to ensure informed reproductive decision-making. If counseling was ameliorated, shifts in the preconception considerations of individuals and couples living with HIV may also shift. The implication of these shifts is unknown but might include reduced stress during the preconception and perinatal period, improved reproductive health outcomes, and potentially higher fertility rates among people and couples living with HIV as some may remain deterred, given the complexity of their considerations.
Footnotes
Authors’ Note
This study was presented at Ontario HIV Treatment Network Conference (OHTN), Toronto, Ontario, Canada, November 17, 2013 to 19, 2013; Abstract 168. Mona Loutfy conceptualized this study. Dean A. Regier conducted the analysis and summarized the results in graphs and tables. V. Logan Kennedy and Mona Loutfy wrote the first draft of the manuscript. All authors contributed to the study design, implementation, data collection, and final revisions to the text and meet ICJME’s requirements as authors.
Acknowledgments
The authors of this article would like to thank all of the study participants and the members of the community advisory board. This study was made possible by the partnerships from all of the study sites.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: CIHR, Institute of Infection and Immunity Catalyst Grant # 103133.