
Abstract
We evaluated the efficacy of a brief motivational intervention (MI) counseling in reducing alcohol consumption among persons living with HIV/AIDS in Kampala, Uganda. Persons living with HIV/AIDS with Alcohol Use Disorders Identification Tool (AUDIT) score ≥3 points were randomized to either standardized positive prevention counseling alone or in combination with alcohol brief MI counseling. The mean change in AUDIT-C scores over 6 months was compared by treatment arm. The mean (standard deviation [SD]) AUDIT-C scores were 6.3 (2.3) and 6.8 (2.3) for control and MI arms (P = .1) at baseline, respectively, and change in mean AUDIT-C score was not statistically different between arms over the 6 months (P = .8). However, there was a statistically significant decrease in mean AUDIT-C score (−1.10; 95% confidence interval: −2.19 to −0.02, P = .046) among women in the MI arm. There was a nondifferential reduction in alcohol consumption overall, but MI appeared effective among women only. Studies with more than 1 counseling session and evaluation of gender differences in treatment response are needed.
Introduction
By the end of 2014, nearly 37 million people were living with HIV/AIDS globally, of which 25.8 million were in the sub-Saharan Africa (SSA) region. 1 The SSA countries have per capita alcohol consumption levels that are well above the global average of 6.2 L of pure alcohol per year. 2 With the high prevalence of both HIV/AIDS and excessive alcohol consumption in SSA, it is not surprising that there is a high prevalence of alcohol use among persons living with HIV/AIDS (PLWHAs). 3 -5
Alcohol use increases the risk for acquisition and transmission of HIV, 6,7 while specifically in PLWHAs, alcohol use is associated with delayed entry and poor retention in care, 8,9 reduced adherence to antiretroviral therapy (ART), 10 increased risky sexual behaviors, 11 and impaired immunological and virological response to ART. 12,13 Therefore, interventions to reduce alcohol use among PLWHAs could lead to improvement in HIV treatment outcomes and potential reduction in further HIV transmission risk. 14
Brief interventions are recommended for the treatment of hazardous alcohol use, a pattern of drinking that increases the risk of harmful consequences, 15 in primary healthcare settings. These interventions, usually last than 30 minutes a session over 1 to 6 sessions, aim to prevent development of harmful alcohol problems including alcohol dependence. 16
Several brief alcohol reduction interventions have been tested in PLWHAs; however, most were done in high-income settings mainly in North America. 17,18 Findings from some trials show effective reduction in alcohol consumption, whereas others show no effect. 19 These findings may not be generalizable to SSA where fewer studies have been done. A study conducted in Kenya among HIV-infected men and women with hazardous or binge drinking showed that 6 sessions of cognitive behavioral therapy (CBT) resulted in significant reduction in percentage of alcohol drinking days among participants in the CBT arm compared to controls who received the standard usual care. 20 Another trial done among patients with tuberculosis in South Africa, of whom 54% where HIV infected, showed that the information–motivation–behavioral skills intervention counseling was not more effective that an education leaflet given to participants. 21 With these few studies conducted, the effectiveness of brief alcohol reduction interventions among PLWHAs in SSA is not yet clearly known, hence the need for additional studies among HIV-infected alcohol drinkers. 22 –24
Among the different brief alcohol reduction interventions, motivation intervention (MI) is one of the most efficacious interventions for hazardous alcohol use. 25 Motivation intervention is a form of directive client-centered counseling approach that enhances the motivation to reduce alcohol use by helping the participants clarify and resolve their ambivalence about reducing alcohol use. 26 Motivation intervention may be provided as a single session with a view that once participants get motivated, they proceed to mobilize within themselves their own change resources without additional training in behavior change skills. The ability to deliver MI in a single session makes it particularly attractive in SSA, which has a heavy workload in a setting of limited healthcare workers. 27 We evaluated the efficacy of a single brief MI counseling session on reduction in hazardous alcohol consumption among PLWHAs not seeking alcohol use care in Kampala, Uganda.
Methods
Study Design, Setting, and Population
This was a randomized trial (clinical%20trials.gov trial identifier NCT01802736) among HIV-infected participants not seeking treatment for alcohol use. The study was conducted at the Adult Infectious Diseases Institute Clinic (AIDC) located within the Mulago National Referral and Teaching Hospital complex in Kampala, Uganda. Details of the clinic population and services have been published previously. 5 This clinic has not had any prior alcohol intervention trials.
Enrollment Procedures
To achieve a representative sample, every 15th patient returning for a clinic appointment was initially assessed for eligibility to participate in the screening for alcohol consumption. Participants were eligible for alcohol screening if they were (1) aged ≥18 years, (2) planning to continue receiving care or be followed up at the AIDC for the next 6 months, and (3) willing to provide written informed consent. Participants were excluded if they were very sick with Karnofsky clinical performance score <50 or if they were pregnant.
All participants fulfilling the initial screening were evaluated for alcohol consumption using the 10-item Alcohol Use Disorders Identification Tool (AUDIT) by a trained nurse counselor, not involved in provision of routine care, in a private nontreatment/consultation room. The sum of the first 3 questions of the AUDIT questionnaire that capture alcohol consumption frequency, quantity, and binge drinking, referred to as AUDIT-C, was used to screen for hazardous alcohol use. 28,29 The AUDIT-C tool has a minimum score of 0 and maximum score of 12 points. Participants with an AUDIT-C score of 3 and above were enrolled into the study.
In addition to the AUDIT interview, additional alcohol consumption evaluations were conducted on enrolled participants using alcohol Timeline Followback (TLFB) method to record days on which alcohol consumption occurred or did not occur within 30 days preceding the interview. The types and brand of alcohol consumed on a typical drinking day were also collected. Information on sociodemographics, HIV treatment history, and alcohol consumption was also collected. Specifically, data on participant age, sex, marital status, religion, highest educational level, employment status, and income in the last month were collected. Participants were evaluated for depression using the 10-item Center for Epidemiology Studies on Depression tool. HIV clinical data including HIV/AIDS clinical stage, ART receipt status, and CD4 count were abstracted from clinic records. Self-reported adherence to medication in the last 1 month was assessed in both ART- and non-ART-receiving patients using a visual analog scale ranging from 0 to 100, with 0 representing all prescribed treatment (ART or co-trimoxazole for those not yet on ART) not taken whereas 100% representing no missed medication.
Randomization and Treatment Allocation
Participants with an AUDIT-C score ≥3 were randomized to 1 of the 2 study arms (standardized positive prevention counseling alone or standardized positive prevention counseling plus MI counseling). The randomization was based on a computer-generated random numbers using permuted blocks of 6, 8, and 10 for an overall total of 15 blocks and assigned to the 2 arms randomly in a 1:1 ratio. Participants were randomized using previously prepared, consecutively numbered, opaque, sealed envelopes. Inside the envelopes was a written paper marked with the treatment arm assignment. Treatment allocation was done by the study nurse who provided assessment interview by opening the next sequentially numbered sealed opaque envelope to reveal the participant’s study arm. The participant was then taken to the respective counselor to receive their assigned counseling.
Study Interventions
Both the control and the intervention were designed with consultation of a psychologist and a social scientist and were administered on the same day after the enrollment interview to participants who had scored ≥3 points on the AUDIT-C. The goal of the treatments was to reduce alcohol use to as low as possible and to abstinence for participants who wished to subsequently abstain from it. The treatments were administered by different study personnel, with 2 counselors dedicated exclusively to each treatment arm.
The intervention arm received the standardized “positive prevention” information (see details below) and advice and, in addition, received a single brief alcohol counseling session lasting between 20 and 30 minutes based on MI style. During the counseling sessions, the counselor reflectively listened to the participant elaborate their alcohol use, reaffirmed the issues surrounding the alcohol use, and inquired about the participants’ plans to reduce alcohol use. The counselor strived to elicit, from the participant, the possible benefits and harms of not cutting down on their alcohol, what they have done along the way to try and cut down if any, what made them fail, and what they are willing to do about those previous attempts to cut down. The counselor summarized the issues as presented by the participant, recognized, and commended their efforts in trying to reduce their alcohol use as well as corrected any misinformation that may have arisen. The participant then set a personal goal of what they do plan for the next 6 months in reducing their alcohol use.
The active control arm received only a one-on-one set of standardized positive prevention information and advice lasting between 10 and 30 minutes delivered by a trained counselor. The positive prevention messages covered the following: how to prevent opportunistic infections, nutritional advice, supporting adherence to medications, encouraging HIV disclosure to sexual partners, safer sex practices including condom and contraceptive use, preventing sexually transmitted infections, as well as avoiding alcohol and substance use. The counselor informed the participant the risks of alcohol use and encouraged them to reduce alcohol intake. After the counseling, participants were provided information on when they will be seen again, and they proceeded to attend the other routine clinic procedures.
Follow-up Study Assessments
At the follow-up visits, at 3 and 6 months postenrollment, participants’ alcohol use that occurred since they were last seen was collected using the same methods as at baseline with modification of AUDIT to reflect a shorter intervisit period of 3 months.
Implementation, Training, and Support
The treatments were provided by minimum of bachelor’s degree–trained counselors, and all had >5 years of clinical experience in HIV clinical counseling strategies but not in alcohol counseling experience. Counselors received induction training and individual ongoing support. A training workshop specifically on treatment administration as well as receiving a treatment manual for the contents and mode of administration of counseling messages was done. There was role-playing for potential participant presentations, specifically for the MI arm and guidance how the counselor would proceed. During study implementation, there was one refresher training to emphasize adherence to treatment protocols. We carried out no formal assessment of treatment adherence and fidelity.
Statistical Analysis
We aimed to test the hypothesis that the brief motivational intervention will result in greater reductions in AUDIT-C scores compared to the control arm. Results from a prior cross-sectional study showed the AUDIT-C standard deviation is 2.6. 5 In order to detect the minimum difference in mean AUDIT-C score of at least 1 point or more between the study arms over 6 months and setting the power at 90%, using a 2-sided test and an α level = .05, and allowing for a 10% loss to follow-up, 160 participants were needed per study arm.
Data were collected on paper forms and double entered in a customized Microsoft Access database (Microsoft Corp). Statistical analyses were carried out using SAS V.9.1.3 (SAS institute) based on intention-to-treat principle, and a P value <.05 was considered statistically significant.
Descriptive characteristics of the study population were summarized as means (SD) and medians (interquartile range [IQR]) for continuous variables and as percentages for categorical variables. Baseline characteristics were compared by treatment arm using χ2 test for categorical outcomes and t tests or Wilcoxon test for continuous outcomes.
To assess study participation and attrition, the proportion of participants seen and those not seen at follow-up is calculated and reasons for missing are summarized. Because not all participants returned for both follow-up visits, we tested for baseline factors associated with the probability of not having both follow-up visits (versus having 2 follow-up visits) using logistic regression methods.
Using known alcohol concentrations of both commercial and locally brewed alcoholic drinks taken on a typical drinking day, 30 we calculated quantity of alcohol in grams (except for the communally served and shared drinks because an individual’s approximate volume consumed couldn’t be ascertained) consumed on a typical day and converted them to US equivalent standard drinks of ethanol by dividing by 14 grams.
The primary outcome, mean AUDIT-C score, was compared using the independent samples t test by treatment arm at each study visit. Furthermore, the mean AUDIT-C score at 3 and 6 months within each treatment arm was compared with the mean baseline AUDIT-C using the dependent samples t test. The difference in the AUDIT-C score between 6 months and the baseline was calculated for each participant and categorized as a reduction in alcohol use frequency and volume if the difference was less than 0 or no reduction if the AUDIT-C difference was ≥0 points.
To assess the intervention effect over time, we used linear mixed-effects model with the AUDIT-C score as the outcome, treatment arm by follow-up time interaction, fixed effect of baseline AUDIT-C and follow-up time while the random component consisted of a random intercept for each participant, and a random slope that allows the correlations between the repeated AUDIT-C measurements to vary over the follow-up time.
To examine gender differences in the intervention effects, we constructed a separate linear mixed-effects model in the strata created by gender.
A set of secondary outcomes, namely, proportion of participants with full AUDIT score ≥8 points, median number of drinking days in the last 1 month, average number of US equivalent standard drinks of alcohol consumed on a typical drinking day, were compared between the treatment arms at the 3- and 6-month visit using χ2, Wilcoxon rank sum, and Student t independent samples tests.
To examine the robustness of our primary findings to missing data or categorical outcome variable, a set of 2 sensitivity analyses were conducted. The primary linear mixed model was rerun after multiple imputation of missing data. Because we had nonmonotone missingness, we used the Markov chain Monte Carlo method to create 20 imputed data sets that were further analyzed as the primary outcome analysis and their results combined using the PROC MIanalyze function in SAS.
Ethics Statement
The study was approved by the scientific review committee of the Infectious Diseases Institute, the Makerere University School of Public Health Research and Ethics Committee, and the Uganda National Council of Science and Technology. The trial was registered on the US clinical trials registry trial identifier NCT01802736. All participants provided individual written informed consent and received no monetary compensation for participation.
Results
Descriptive Characteristics
Between August 2013 and April 2014, 1253 participants were approached, of whom 982 (78.4%) fulfilled the initial eligibility criteria and were screened for alcohol use. Of these, 342 (34.8%) participants scored 3 or more points on the AUDIT-C test, of which 337 accepted and were randomized to the 2 study arms (Figure 1).

Trial profile of persons living with HIV/AIDS (PLWHAs) enrolled in the alcohol intervention trial at the Infectious Diseases Institute, Kampala, Uganda.
The median (IQR) age of the enrolled participants was 39 (32-46) years, 221 (65.6%) were males, 303 (89.9%) were employed, and 258 (76.6%) were receiving ART. Baseline characteristics were similar in the 2 arms (Table 1), except the median CD4 count, which was higher in the intervention arm, 424 (288-567) cells/µL, compared to the control arm, 363 (264-480) cells/µL, P < .001. The mean AUDIT-C score at baseline was comparable in the treatment arms (6.4 [SD 2.2] in the control and 6.8 [SD 2.3] in the intervention arms, respectively, P = .099).
Baseline Characteristics of PLWHAs by Treatment Allocation Group Enrolled in the Alcohol Intervention Trial, Kampala, Uganda.
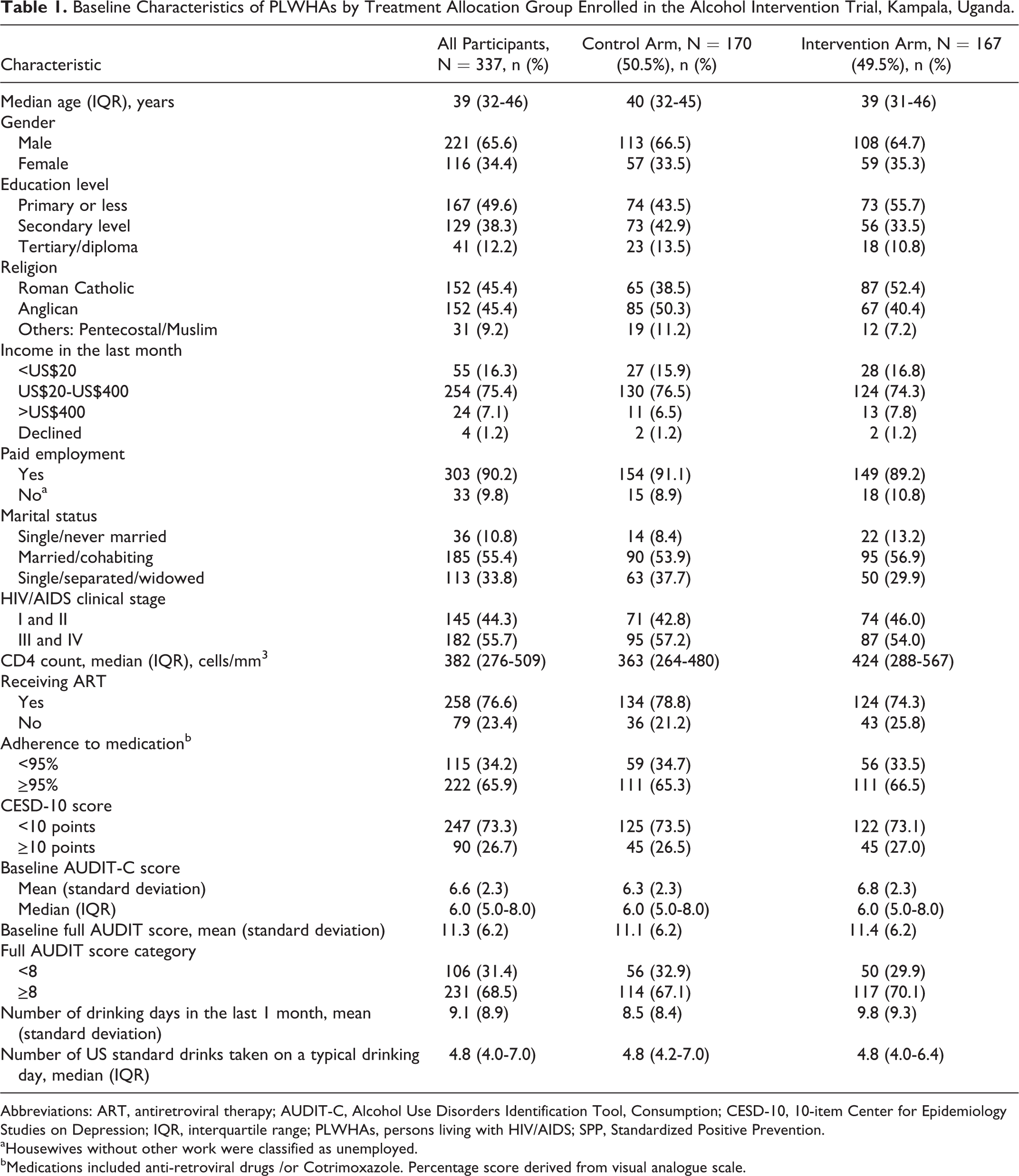
Abbreviations: ART, antiretroviral therapy; AUDIT-C, Alcohol Use Disorders Identification Tool, Consumption; CESD-10, 10-item Center for Epidemiology Studies on Depression; IQR, interquartile range; PLWHAs, persons living with HIV/AIDS; SPP, Standardized Positive Prevention.
aHousewives without other work were classified as unemployed.
bMedications included anti-retroviral drugs /or Cotrimoxazole. Percentage score derived from visual analogue scale.
A total of 286 (84.9%) of the 337 participants returned for the 3-month visit and 321 (95.3%) returned for the 6-month visit (Figure 1). Overall, 304 (90.2%) returned for at least 1 follow-up visit, whereas 280 (83.1%) returned for both follow-up visits. There was a statistical trend for participants with baseline full AUDIT scores above 8 not completing both follow-up visits (odds ratio = 1.9, 95% confidence interval [CI]: 0.96-3.75, P = .06). The odds of not completing both follow-up visits were 14% higher for every 1 point increase in baseline AUDIT-C scores. The odds of not completing both follow-up visits did not differ by treatment arm, participant characteristics, CD4 level, or adherence level.
Change in Alcohol Consumption Over Time
There was an overall reduction in the mean AUDIT-C score in the 6 months of follow-up: 6.4 to 3.4 (P < .0001) in the control arm and 6.8 to 3.9 (P = .001) in the intervention arm.
The decline in both arms was greatest in the first 3 months after the counseling (Table 2). The mean AUDIT-C score at 3 months was significantly lower in the control arm compared to the interventional arm (3.5 [SD 3.0] in the control group versus 4.3 [SD 3.0] in the interventional group, P = .034; Table 3); however, the mean scores were not different between groups at 6 months (3.4 [SD 3.0] in the control group versus 3.9 [SD 3.0] in the interventional group, P = .141).
Results of Linear Mixed Model of AUDIT-C Scores by Arm and Over Time in Kampala, Uganda.

Abbreviations: AUDIT-C, Alcohol Use Disorders Identification Tool, Consumption; CI, confidence interval; MI, motivational intervention.
aAll models are linear mixed effects adjusting for follow-up visit and baseline AUDIT-C score, random intercept, and random slope for follow-up visit.
Baseline, 3-, and 6-Month Visits’ Alcohol Consumption Outcomes of PLWHAs Enrolled in the Alcohol Trial, Kampala, Uganda.

Abbreviations: AUDIT-C, Alcohol Use Disorders Identification Tool, Consumption; PLWHAs, persons living with HIV/AIDS; SD, standard deviation.
There was no significant difference in mean AUDIT-C change over the 6-month follow-up time between the intervention and the control arms, mean AUDIT-C difference of the differences = −0.07, 95% CI: −0.70 to 0.56, P = .8266 (Table 2).
The proportion of participants with mean AUDIT-C scores ≥3 was significantly lower in the control group compared to the interventional arm at 3 months (58.5% in the control group versus 71.5% in the interventional group, P = .019) and at 6 months (57.2% in the control group versus 70.2% in the interventional group, P = .024; Table 3).
Overall, 354 (58%) of 610 of the person-visits had reduction in AUDIT-C scores, with no differential AUDIT-C reduction by arm, that is, 180 (59.2%) of 304 persons-visits in the intervention arm and 174 (56.9%) of 306 in the control arm (P = .56). The majority, 22 (62.7%) of the 354, of the reductions occurred in the first 3 months, with the remaining 132 (37.3%) of the 354 occurring between the 3- and 6-month visit. There was no statistically significant difference in the proportion of participants who had a reduction in AUDIT-C score between the baseline and month 6 visit in the intervention arm, 128 (81.5%) of 157, versus control, 121 (77.1%) of 157 arm (P = .3296).
Gender-stratified mixed-effects model showed that mean difference in AUDIT-C change over time was not different by treatment arm among males (0.38, 95% CI: −0.41 to 1.17, P = .3493), whereas among females, the MI arm had greater AUDIT-C reductions compared to the control arm (−1.10, 95% CI: −2.19 to −0.02, P = .0457; Table 2).
The median drinking days were not different between arms at baseline (6.0 in the control arm versus 7.0 in the intervention group), and similarly, they were not different at the 3- and 6-month follow-up visits. A similar trend was observed in the mean number of drinks consumed (Table 3).
Discussion
Identifying an efficacious single-session brief alcohol intervention would greatly reduce the consequences of hazardous alcohol consumption among PLWHAs in SSA. Brief alcohol interventions, especially those limited to a single session that can be integrated into routine care, are advantageous for resource-limited settings. 31 In this trial, we observed significant reductions in alcohol consumption after a single brief counseling session among HIV-infected men and women consuming alcohol at hazardous levels and not seeking treatment for alcohol use in Kampala, Uganda. The greatest reductions in alcohol use were in the first 3 months after the intervention. There were minimal reductions observed between the 3- and 6-month intervals. The proportion of participants with reduction in AUDIT-C scores was higher, but the difference was not statistically significant in the intervention arm compared to the active control arm. Similarly, there was no statistically significant difference in mean change in AUDIT-C scores 6 months following the intervention and control treatment counseling. The trial shows that MI counseling did not result in greater reductions in alcohol consumption over and above the standard-of-care positive prevention counseling among HIV-infected persons with hazardous alcohol use.
Our study is one of the few studies in SSA that has attempted to reduce alcohol consumption among PLWHAs not seeking care for their alcohol use and increases our understanding of alcohol use interventions in this setting. Moreover, our use of random allocation of treatment and a single MI session is in line with the Mesa Grande recommendations. 25
Despite evidence from systematic reviews demonstrating support for the use of brief alcohol interventions and motivational interviewing in primary care settings to reduce both alcohol use and related behaviors, 32,33 we did not observe similar results among PLWHAs in Uganda. The difference in the findings is that the studies included in the reviews used participants whose HIV status was either unknown or who were HIV uninfected and were from settings of low HIV prevalence, whereas this study was exclusively among HIV-positive participants enrolled in clinical care. In the few trials conducted among PLWHAs, similar findings of no effect of the intervention were observed by Samet et al in 151 PLWHAs in Boston, 34 and 2 other trials, one by Gilbert et al using the “video doctor” and the other by Parsons et al using cognitive behavioral and skills training, demonstrated no difference in alcohol consumption in the interventional group compared to standard of care after 6 months. 19,35
In fact, a synthesis of interventions among only PLWHAs by Brown and colleagues concludes that the reviewed studies provided mixed results on reduction in both alcohol frequency and quantity between the intervention and the comparison conditions, with 6 of the studies demonstrating significant reductions in alcohol frequency and quantity between the intervention and comparison conditions and the other 6 showing no significant interventions effects. 36 Among the studies with efficacious intervention effects is one study done in a typical SSA large outpatient HIV clinic in western Kenya that recruited HIV-infected hazardous/binge drinkers, using 6 sessions of CBT delivered by para-professionals, resulted in greater alcohol reductions in the intervention compared to a standard-of-care control. 20 In another trial by Velasquez et al among HIV-infected men who have sex with men, participants randomized to 4 session of motivational interview counseling significantly reduced their number of drinks as well as heavy drinking in the last 30 days compared to the controls who received educational material only. 37 The difference between this trial and our trial is that the intervention was provided in more than 1 session and effects were assessed after a short time interval of 30 days. Indeed, our trial shows that the reductions in alcohol consumption are realized within the first few months closest to the intervention(s). 37 A more recent trial among only HIV-infected women showed that 2 sessions of brief intervention resulted in a 58% reduction in the 90-day alcohol consumption frequency over 12 months in the intervention arm. 38
The marked but nondifferential reductions in alcohol consumption as measured by AUDIT-C suggest that both the intervention and the control had equally “partially effective components” 39 because our “active” control arm also received one-on-one counseling messages unlike other studies that use patient leaflets in the control arm.
Prior research has shown that participation and answering alcohol assessment questions may lead to reduced reporting of drinking behavior, mainly due to self-reflection and/or assessment reactivity to alcohol-related questions. 40 These effects therefore may have distorted the measured intervention effects and could account for the lack of effect noted in our study. However, it is not possible to determine whether these effects occurred and whether any such effects were differential by treatment arm.
We observed differential intervention effects by gender, with a statistically significant effect of MI only among female participants. This suggests a possible gender interaction effects, although our study was not powered to test the significance of this interaction. It is possible that the men were not satisfied with the one-on-one counseling style as has been previously proposed in a study conducted in South Africa. 41 This finding should be taken within the context that we did not hypothesize a priori that women would have a greater reduction in AUDIT-C scores relative to the control arm as observed in our study. It is possible that this observation was due to type 1 error or due to a differential bias in alcohol consumption reporting among women versus men. The observed reduction in AUDIT-C score in women could also represent a real effect of the intervention. Further, perhaps women were more likely than men to embrace the advice to reduce their alcohol consumption. Additional studies are required to confirm this apparent beneficial effect of MI among only women.
These results need to be interpreted in the context of the following limitations. We used self-reported measures of alcohol consumption that may be prone to recall and social desirability response biases. The best way to validate the self-report would be to use alcohol biomarkers; however, this was not feasible at the time the study commenced, and we believe that our use of the TLFB method aided in alcohol use recall. 42 Although we conducted baseline alcohol assessment interviews prior to randomization, we are not able to ascertain whether there was any differential bias in reporting alcohol use by study arm during the follow-up period. Biomarkers revealed differing drinking results when compared to self-report among PLWHAs in a rural clinic in Uganda, with self-reports showing declining unhealthy alcohol use in the first year of care, while using the biomarker revealed no trend overall. 43 Therefore, future studies in this setting should consider the use of biomarkers.
Although we did not provide an objective assessment to fidelity of the intervention, we provided preimplementation training, study treatment manuals, and continuous implementation support to ensure that the interventions were provided per the protocol. Despite all these efforts and the counselors in the 2 arms were of comparable expertise and duration of clinical counseling experience, it is possible that the counselors in the 2 arms differed in their ability to get participants to reduce their alcohol consumption; however, we are not able to ascertain whether this occurred and to what extent. The duration of follow-up may have been short to comprehensively ascertain the effects of the counseling programs, and therefore, we may have recorded only the short-term efficacy of the counseling programs. We did not expect a longer effect with a single counseling. We observed most of the reductions in the first 3 months, probably an indicator that a single counseling session effects may not be maintained over a longer duration. Therefore, future studies may need to consider the addition of booster counseling sessions.
Our findings are from a single HIV clinic, thus may not be generalizable; however, this clinic has a patient population that is similar to a typical patient population of PLWHAs in SSA. 44
Based on our findings and from the literature on interventions for alcohol use among PLWHAs, a single session of MI may not result in significantly greater reduction in alcohol use frequency and quantity over 6 months as compared to general positive prevention counseling in HIV clinics. Therefore, strengthening and standardizing the current positive prevention messages to always include alcohol consumption inquiry and alcohol reduction information is feasible and should be continued in current HIV clinical practice. These counseling messages can easily be administered by trained routine care providers (not necessarily a specialist counselor) and are brief allowing for incorporation into routine clinical care.
It is possible that more interventional effects may be demonstrated with repeated MI sessions in PLWHAs with hazardous alcohol use more so among female participants. Therefore, a larger trial designed to address the apparent gender interaction, providing additional counseling sessions and longer follow-up evaluations possibly supported with innovative interactive telephony and technology support, and objectively assess alcohol consumption using biomarkers is needed. In addition, identifying determinants and mediators of treatment response, the best measures of motivation to reduce alcohol, and how these measurements should be assessed in subsequent studies and practice among PLWHA in SSA should be undertaken.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported, in part, by the Wellcome Trust through Training of Health Researchers into Vocational Excellence in East Africa (THRiVE) consortium grant no. 087540 (B.W.) and NIH grant number K24AA022586 (J.H.).