
Abstract
Combination antiretroviral therapy has been shown to reduce HIV transmission and incident infections. In recent years, Malawi has significantly increased the number of individuals on combination antiretroviral drugs through more inclusive treatment policies. Using a retrospective observational cohort design, records with HIV test results were reviewed for pregnant women attending a referral hospital in Malawi over a 5-year period, with viral load measurements recorded. HIV prevalence over time was determined, and results correlated with population viral load. A total of 11 052 women were included in this analysis, with 440 (4.1%) HIV infections identified. HIV prevalence rates in pregnant women in Malawi halved from 6.4% to 3.0% over 5 years. Mean viral loads of adult patients decreased from 120 000 copies/mL to less than 20 000 copies/mL. Results suggest that community viral load has an effect on HIV incidence rates in the population, which in turn correlates with reduced HIV prevalence rates in pregnant women.
Introduction
HIV prevalence rates in Malawi remain at a medium to high level, that is, at approximately 11%, 1,2 despite commendable efforts of the national response to HIV and AIDS coordinated by the National AIDS Commission in the country. As of September 2012, Malawi had almost 400 000 people living with HIV on highly active antiretroviral therapy (HAART). 2 This is a common favorable trend in several sub-Saharan African countries, following joint efforts of governments, the Global Fund, the US President’s Emergency Plan for AIDS Relief (PEPFAR), and local and international nongovernmental organizations (NGOs) to expand antiretroviral access to affected populations. 3
The role of HAART in lowering HIV incidence is being progressively documented. Different studies have shown significant reduction in sexual transmission of HIV at the community level through the use of HAART. 4,5 Recently, the HIV Prevention Trials Network (HPTN) 052 study has shown a 96% reduction in HIV transmission among serodiscordant couples in several countries when the HIV-positive partner receives HAART. 6 The sustained suppression of HIV in genital secretions with the use of HAART is the most likely mechanism for the prevention of HIV transmission. 7 At a population level, this can be expressed as a reduction in the “community viral load,” the viral load averaged over the whole population. 4 Similarly, administration of HAART during pregnancy and breast-feeding was proven extremely effective in preventing mother-to-child transmission of HIV. 8 –10
Several models, either based on theoretical assumptions 11 or based on data originating from large sub-Saharan patient cohorts, 12 suggest that a yearly test-and-treat strategy could rapidly lower the HIV incidence to very low rates in the population and would achieve a prevalence rate of 1% in the adult population within the long term (3-5 decades). In the short term, initiating treatment earlier in generalized epidemics saves lives and money. 13 Apart from reduction in HIV transmission, it has also been clear that there is (in most cases) individual benefit from early initiation of treatment. The use of HAART has dramatically reduced disease progression and death in patients with HIV infection. 14 -16 The purpose of the present study is to describe the impact of a treatment/prevention of mother-to-child transmission (PMTCT) approach on HIV prevalence in pregnant women living in a rural area of Malawi, based on large numbers of individuals registered in our program database.
Methods
Study Design and Population
A retrospective cohort design was used in this analysis. The study population was composed of individuals living in the catchment area of the Francisco Palau Hospital (FPH), Dowa district, in the central region of Malawi. This institution is the main provider of health services for the region. The main characteristics of the population living in the catchment area of the hospital are listed in Table 1. The Drug Resource Enhancement Against AIDS and Malnutrition (DREAM) Program (an NGO of the Community of Sant’Egidio) has been running an antiretroviral treatment (ART) clinic and a PMTCT program at FPH since 2004 and 2005, respectively. Guidelines of the DREAM ART program for treatment initiation in adults include a CD4 count lower than 350 cells/mm3 or a CD4 count between 350 and 500 cells/mm3 if the viral load is higher than 100 000 copies/mL and/or a World Health Organization (WHO) clinical stage 3 or 4. The PMTCT guidelines include provision of HAART to all HIV-positive pregnant women from the 14th week of gestation until 12 months after delivery. 8,9 All pregnant women accessing antenatal care (ANC) for the first time at FPH during the study period underwent an HIV rapid test. They were given the option to retrieve results if they wanted to, per Malawi’s health policy. HIV-positive pregnant women who opted to receive HIV rapid test results were offered HAART per the DREAM and Malawi program guidelines. Laboratory monitoring (including viral load and CD4 counts, basic biochemistry, and complete blood counts) was done on a routine basis for all patients, as well as monthly food supplementation to all pregnant women and to severely malnourished adult patients (body mass index less than 18.5). The DREAM program operates in Malawi under the operational research protocol n.386 approved by the Malawian National Science and Health Research Committee. The DREAM program activity coexisted at FPH in parallel with another ART clinic run by the hospital personnel. This clinic provided treatment to all adults with CD4 counts less than 250 or patients with a WHO clinical stage 3 or 4, according to national guidelines in place at the time.

Abbreviations: ANC, antenatal care; DREAM, Drug Resource Enhancement Against AIDS and Malnutrition; FPH, Francisco Palau Hospital; HAART, highly active antiretroviral therapy.
Study Procedures
In the present analysis, the HIV infection rate among pregnant women accessing ANC services at FPH was used in the determination of HIV prevalence rates in the general population. The ANC service access rate is very high throughout Malawi: about 90% of women access the service at least 1 time during pregnancy. 1 Since September 2005, the opt-out approach for HIV testing and counseling was implemented in the FPH ANC service as well as in the rest of the country. All women accessing ANC services were offered group counseling sessions on HIV testing followed by HIV screening (determine 1/2 Rapid HIV test; Alere, Bedfordview, South Africa, and Uni-Gold Rapid Test; Trinity Biotech, Bray, Ireland, for confirmation of any positive result). In the Opt-Out HIV testing approach, clients chose whether to get test results or not. Pregnant women who chose to receive test results underwent a face-to-face counseling session before receiving results by a qualified counselor. HIV test results were recorded in the Malawi national register as per country guidelines and coded and recorded into the DREAM database for treatment management and surveillance purposes. All activities were authorized by the institutional review boards in Malawi and Italy. Following September 2010, 2 additional centers initiated the provision of PMTCT services within the previous catchment area of FPH and, therefore, the present analysis did not include any patients presenting to care after September 2010, in order to ensure a homogeneous patient population and avoid potential selection bias.
Statistical Analysis
The comparison of HIV prevalence over time was performed through χ2 tests, and determination of the odds ratio (OR) with 95% confidence intervals (95% CIs) was computed by the SPSS statistical package 19.0. The population’s viral load was calculated based on viral load values of individual patient accessing the DREAM program clinics at FPH. At least 1 quantitative viral load assay (b-DNA technique) was performed every year on every patient followed in the DREAM clinics at FPH, irrespective of whether they were on HAART. HIV prevalence was evaluated in relation to the population viral load.
Results
The population within the catchment area of FPH at baseline consisted of 56 800 individuals, with an estimated HIV prevalence of 6.0%. 1,17,18 The estimated number of HIV-positive adults within this catchment area, however, was 1700. Estimates for the number of HIV-positive patients in this area were derived from applicable incidence and mortality rates according to national estimates. 1 On the basis of these estimates, for the purposes of this analysis, an additional 300 individuals were added to the estimated number of adults living with HIV within the catchment area for a total number of approximately 2000 individuals. In addition, as of 2005, a total of 4232 HIV-positive adults initiated HAART at the institution. This higher figure is explained by the fact that the hospital attracts patients who also live outside the catchment area. The number of patients receiving ART increasingly outnumbered the number of patients in prior years who accessed HIV treatment at FPH from 2005 to 2010. Hence, we estimate that a high percentage of HIV-positive patients within the catchment area accessed both ART services available at FPH.
The general fertility rate in Malawi is 154 to 213/1000. 2 Therefore, the estimated cumulative number of pregnancies in the region from 2005 to 2010 ranged between 13 000 and 18 500. In total, 14 197 pregnant women were tested for HIV at FPH during the years 2005 to 2010, with 11 052 (80%) included in this analysis. Clients who were tested before September 2005 or after August 2010 in the HIV clinic at FPH were excluded from this data set either because the opt-out approach was not applicable before September 2005 or because of the change in the flow of pregnant women due to the opening of new ANC services in the catchment area after 2010. The mean age of pregnant patients was 28 years (SD ±5.4), and the estimated cumulative number of pregnancies among HIV-positive women from the catchment area between 2005 and 2010 ranged from 800 to 1100. The cumulative number of HIV-positive pregnant women who started HAART from 2005 to 2010 during ANC at FPH was 856 (DREAM program database). The numbers demonstrate that ANC services at FPH were accessed by at least 80% of the highest estimate of HIV-pregnant women in the catchment area during the study period.
The HIV prevalence dropped from 6.40% in 2005 to 2.84% in 2010 (OR: 0.474; 95% CI: 0.330-0.683; Table 2) in the population of women who went for testing for the first time or women who had tested negative before the current pregnancy. As shown in the comparison between the expected number of cases in 2006 and the observed number of cases, a decline in absolute numbers was observed over the years, with 185 less cases in 2006 than originally estimated (30% reduction). From 2006 to 2010, the decline in HIV prevalence among pregnant women in this area was close to 50% (Figure 1). It is unlikely that the decrease in HIV prevalence among pregnant women in Malawi was due to more women opting out of testing under the opt-out approach as HIV acceptance rates became reportedly very high in Malawi after this guideline was adopted, that is, in the range of 99%. 19 In our clinics in Malawi, we noted a significant increase in testing over time, and opt-out rates were negligible among pregnant women (<1%-2%) overall.
Yearly HIV Prevalence in Pregnant Women Accessing ANC at Francisco Palau Hospital.

Abbreviation: ANC, antenatal care. aExpected number of cases based on the 2006 prevalence rate.
b2005: 4 months were included in the analysis as HIV testing was only offered routinely as of September 2005.
c2008: November 2008 was excluded from the analysis due to error in register compilation.
d2010: the first 8 months were included in the analysis (refer to Methods section).

HIV prevalence among pregnant women tested at Francisco Palau Hospital antenatal care (ANC) services by year (value and 95% confidence interval [CI]).
The calculation of mean population viral loads per year for both adult nonpregnant patients and pregnant women shows a decline in background prevalence rates. The mean viral load of adult patients at FPH dropped from about 120 000 copies/mL in 2005 to less than 20 000 in 2010 (P < .001; Figure 2). The decline in community viral load paralleled the decline in HIV prevalence among pregnant women.
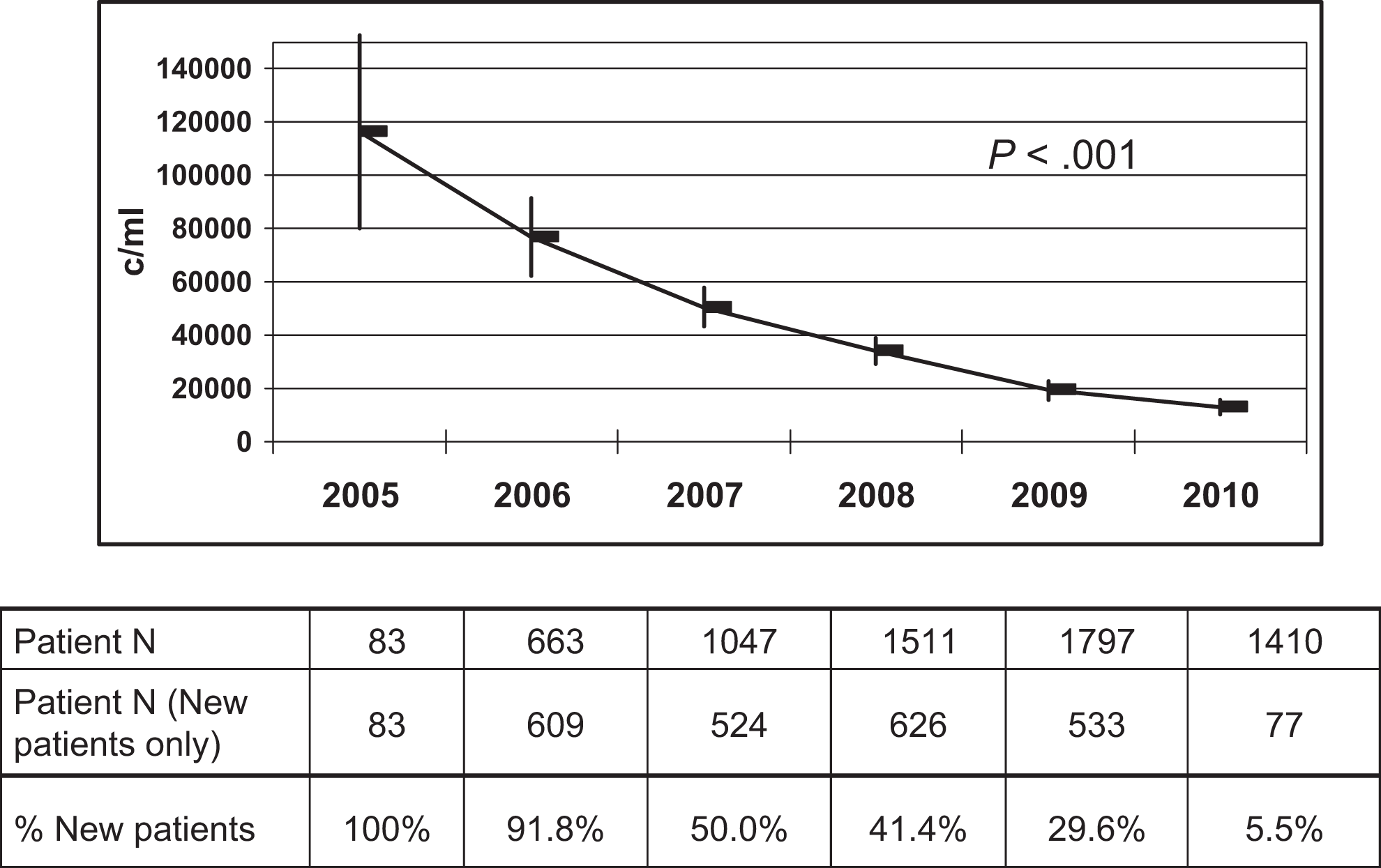
Mean viral load (and 95% confidence interval [CI]) of Drug Resource Enhancement Against AIDS and Malnutrition (DREAM) program patients at Francisco Palau Hospital by year.
Discussion
In the context of generalized epidemics, HIV testing of pregnant women is considered a good proxy estimate for the prevalence of infection in the general population. 20 Most sentinel surveillance sites in sub-Saharan Africa are in fact ANC clinics that assess HIV prevalence during pregnancy. Our results demonstrate that the HIV prevalence among pregnant women in the FPH cohort decreased by almost 50% between 2006 and 2010. In contrast, the HIV prevalence reported for the nearest facility to FPH (Mponela Health Center, which is primarily outside the FPH catchment area but within the same administrative district of Dowa) was reportedly 6% in 2010. 1 This is the same prevalence reported in prior years for the Dowa district rural area where the Francisco Palau hospital is located. 18 Therefore, our findings indicate that the HIV prevalence trend for the FPH catchment area is different from the ones observed in adjacent rural areas. Our results highlight the favorable impact of ART on the population accessing hospital ANC services, especially those who live mainly within the hospital catchment area. The decrease in HIV prevalence was associated with a decline in mean HIV viral load values among individuals accessing treatment at the same institution. It is likely that the decrease in mean HIV viral load reflects a reduction in circulating virus, which would be the main reason for the observed decrease in HIV prevalence over time.
The general situation of HIV prevalence in Malawi appears to parallel the trend observed in our FPH cohort. The HIV prevalence rate in rural settings (similarly to the FPH catchment area) reported in the national Malawi database decreased from 12.5% in 2004 to 10.5% in 2010. 1,16 Nevertheless, during the same period, the rural sentinel surveillance site closest to FPH reported an overall HIV prevalence of 5.6% and 6.2% in 2001 and 2006, respectively, which is distinctly different. 17,18,21 We attribute these findings to the fact that the total number of people living with HIV/AIDS (PLWHA) has increased since mortality decreased due to the widespread ART coverage in the country. Nevertheless, the widespread availability of treatment has also reduced the number of new infections significantly, with reports suggesting a 50% decline in incident infections. 1 The balance of these 2 situations could first appear as a stabilization in HIV prevalence over time followed by a subsequent decline in prevalence, as new infections decrease. We believe there is a declining trend in HIV prevalence in rural areas in Malawi, however, this finding is distinctly more pronounced in the FPH catchment area, where policies for treatment of a large number of PLWHA tend to be more disseminated and heavily implemented. Our hypothesis is that the reduction in population viral load in the FPH catchment area substantially contributes to the reduction in HIV prevalence in our observed population of pregnant women. The reduction was significant and occurred as the population viral load dropped from 120 000 copies/mL in 2005 to 20 000 copies/mL in 2010. This is probably due to the large number of PLWHA treated in the 2 ART clinics operating at FPH in addition to the DREAM PMTCT program on site, which implemented triple therapy to all HIV-infected pregnant women attending our clinic. Certainly, the reduction in prevalence observed in 2010 is also related to the decrease in incident infections, as incident infections are usually accompanied by higher viral loads. There is emerging evidence that reduced infectiousness at a population level, which is attributable to wider ART coverage in some communities, contributes to decline in HIV incidence. 4,22,23
Limitations of our study include the fact that we cannot demonstrate a causal association between ART and decline in HIV prevalence as our analysis did not include a control population. One additional limitation was that the actual residence of pregnant women attending FPH was not recorded in our database. Nevertheless, there is no reason to believe that patients would be coming from other districts. There are significant limitations in transportation, and most likely women initiated ANC care in health service facilities close to their home, which would be easily reached in case of need. Since the standard of care is very similar across the country, there would be no incentive for patients to procure ANC further away from home. We did note an increase in other patients seeking ART care as of 2005 at FPH, a higher estimate than anticipated, likely reflecting the fact that individuals from outside the catchment area were coming to FPH for the provision of ART. Although the unavailability of residence data is a study limitation, we do not believe that patients seeking care at FPH from outside the catchment area would affect population viral load results. We assumed that the decline in population viral load was attributable to the availability of ART at FPH. If the decline in population viral load was due to the inclusion of patients living outside the hospital catchment area, one would need to consider extraneous factors associated with population viral load decline other than the availability of ART. One could speculate, for example, a difference in antiretroviral adherence related to socioeconomic factors. As the hospital in question is located in a very rural area, individuals coming from outside that area could potentially have more resources. As higher socioeconomic status can possibly be associated with better adherence to ART, one could hypothesize that the inclusion of outside patients might improve adherence in the overall population. Improved adherence in turn would influence the decline in population viral load. Although this hypothesis is plausible, we did not find any evidence to support it. We performed analyses using occupation as proxy for catchment area of residence as individuals within the catchment area were mainly farmers or unemployed, whereas merchants, clerks, students, or teachers were likely from outside the catchment area, and housewives were equally distributed between both groups. No statistical significant differences were seen in viral load levels by individual occupation either before or after HAART administration (data not shown). We are confident that the decline in viral load observed was due to the use of ART in this setting.
In an ideal setting, it would be optimal to evaluate 1 district with approximately 200 000 individuals in order to study the impact of universal HIV test-and-treat strategies for all pregnant women as well as all HIV-infected patients with CD4 counts less than 350 cells/mm3. These efforts should be coupled to an intense campaign aimed at behavioral change and massive male circumcision. This approach would provide crucial information about the potential reversal of the HIV epidemic in sub-Saharan Africa in the decades to come.
The significance of universal ART during pregnancy for reduction in HIV vertical transmission has been extensively demonstrated in multiple studies, 8 –10 as well as the importance of HAART to HIV-positive partners in serodiscordant relationships with a dramatic reduction in HIV sexual transmission. 6,7 The possibility of reversal of the HIV epidemic has already been shown through mathematical models based either on theoretical assumptions or on real-world data. 11–12 Both approaches were based on multiple interventions including the choice of treating all newly diagnosed HIV-infected patients through an annual program for universal HIV testing or the choice of providing triple ART to all HIV-positive pregnant women and treatment of PLWHA with CD4 counts below 350.
Our findings highlight the impact a specific intervention, that is, increased availability of ART, can have on HIV prevalence within a designated catchment area. This intervention was part of the approach considered in both cited modeling studies. However, even if our intervention included only a partial application of the approach suggested in the models, a significant impact on HIV prevalence was noted, demonstrating that the public health treatment approach currently in place in Malawi, after the implementation of 2010 guidelines, can significantly decrease the spread of HIV infection in the country.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The DREAM (Drug Resource Enhancement Against AIDS and Malnutrition) Program of the Sant’Egidio Community, a faith-based NGO in Rome, Italy, is sponsored by multiple organizations including the World Bank Treatment Acceleration Program, several Italian private banks, several governmental cooperations including the German Agency for Technical Cooperation, the Agence Francaise de Développement, the Catalan Agency for Development Cooperation, the Belgium Development Cooperation, and the United States President Emergency Plan for AIDS Relief among others. DREAM program–Project Malawi was funded in Malawi by Intesa Sanpaolo, Italy, and the CARIPLO Foundation, Italy. The present analysis was not funded by a specific award.