
Abstract
Objectives:
Evidence-based guidelines have long recommended that HIV care providers deliver HIV transmission risk-reduction (RR) services, but recent data are needed to assess their adoption.
Methods:
The authors surveyed a probability sample of 1234 US HIV care providers on delivery of 9 sexual behavior– and 7 substance use–related HIV transmission RR services and created an indicator of “adequate” delivery of services in each area, defined as performing approximately 70% or more of applicable services.
Results:
Providers were most likely to encourage patients to disclose HIV status to all partners since HIV diagnosis (81%) and least likely to ask about disclosure to new sex and drug injection partners at follow-up visits (both 41%). Adequate delivery of sexual behavior– and substance use–related RR services was low (37% and 43%, respectively).
Conclusion:
The majority of US HIV care providers may need additional support to improve delivery of comprehensive HIV transmission RR services.
Introduction
Improvements in treatment and a relatively stable number of new infections have resulted in a growing population of persons living with HIV in the United States and an increasing public health need to support HIV-infected persons in reducing behaviors that may transmit HIV to others. Although biomedical approaches to prevention have grown in importance, behavioral prevention services are still recognized as necessary and effective components of a combination approach to HIV prevention. Evidence-based federal guidelines for HIV prevention, including the newly published Recommendations for HIV Prevention with Adults and Adolescents with HIV in the United States, have long recommended that HIV care providers deliver an array of behavioral prevention services to HIV-infected patients to prevent transmission of HIV, 1,2 and delivery of these services is also recommended as an essential element of quality HIV clinical care. 3,4 Recommended services include risk screening for sexual risk behaviors, substance use, symptoms of sexually transmitted diseases (STDs), and current sex and drug injection partners, in addition to the provision of risk-reduction (RR) intervention services, which include provider-delivered RR counseling and provision of or referral to intensive RR interventions for those who continue risky behaviors. Moreover, providers are recommended to encourage patients to disclose their HIV status to all sex and drug injection partners since the time of diagnosis and on an ongoing basis, in addition to assisting the patient with partner notification through referral to partner services.
Despite these long-standing recommendations and the efficacy of RR services, 2,5,6 the available evidence suggests that delivery of prevention services by health care providers is suboptimal. Among a national probability sample of HIV care providers participating in the Medical Monitoring Project (MMP) provider survey in 2009, 66% reported always discussing HIV transmission RR and 35% reported always discussing partner counseling services with patients who were new to HIV medical care. 7 Because studies find that providers are more likely to provide RR services at initial as opposed to follow-up visits, 8,9 delivery of these services to all HIV-infected patients was likely lower. An analysis of MMP patient interview data collected in 2009-2010 found that only 44% of US HIV patients reported having a discussion with a health care provider about HIV/STD prevention. 10 Observational studies of patient encounters have also documented low levels of RR screening and counseling, even when indicators of risk behavior were present. 11,12
Recent surveys of health care providers have identified provider characteristics (profession, age, race/ethnicity, attitudes toward prevention counseling) and practice characteristics (time allotted to patient visits, number of HIV-infected patients) associated with nonadherence to recommendations regarding delivery of prevention services. 7,9,13 In most surveys, RR services are measured either by a global question (eg, how often do you discuss transmission RR) 7,13 or by a limited number of questions. 9,14 These shortcomings in measurement limit the ability of these studies to identify which RR services are least often provided—information needed to inform efforts to improve delivery of RR services. Also, most provider surveys have not examined delivery of HIV transmission RR services related to alcohol and drug use or disclosure of HIV status to the partners of persons who inject drugs (PWID), which are key parts of a comprehensive approach to RR. Although one study found that 77% of providers in 7 hospital-based HIV care centers reported asking most or all patients seen in the past month about alcohol use, 15 to our knowledge an assessment of provision of more comprehensive substance use–related HIV transmission RR services by clinicians in a wide range of care settings has not been published.
The present study extends the earlier work discussed above 7 –9,11 –14 by presenting analyses of more recent data from providers in a variety of clinical settings across the United States and by examining delivery of a broader range of HIV RR services, including those related to alcohol and drug use, which may help to identify specific areas needing improvement. Further, to guide efforts to increase delivery of RR services, we identify provider and practice characteristics independently associated with the provision of adequate HIV RR services in 2 areas: sexual behavior and substance use.
Methods
We analyzed data collected from the 2013 MMP Provider Survey, which was conducted in the geographic areas and HIV care facilities sampled for MMP in 2011. 16,17 The Provider Survey used a complex 2-stage sample design, first by selecting 16 states and 1 territory using probability proportionate to size (PPS) sampling, with size based on estimates of the number of AIDS cases. All sampled geographic areas agreed to participate in MMP, including California, Delaware, Florida, Georgia, Illinois, Indiana, Michigan, Mississippi, New Jersey, New York, North Carolina, Oregon, Pennsylvania, Puerto Rico, Texas, Virginia, and Washington. Second, 622 facilities within these areas were sampled using PPS based on the number of persons receiving care for HIV infection, and 505 of these facilities participated in the Provider Survey (81% crude participation rate). Participating facilities provided a list of 2208 providers, all of whom were invited to participate in the MMP provider survey. Providers were eligible to participate in the survey if they were physicians, physician assistants, or nurse practitioners (NPs) who had completed their training and provided HIV care (defined as ordering CD4 count or HIV viral load tests and/or prescribing antiretroviral medications) between January and April 2012. Providers were recruited with a modified version of Dillman’s Tailored Design Method, 18 which included mailing individualized recruitment packets to all of the providers in participating facilities, with follow-up letters and e-mails sent at set intervals between June 2013 and January 2014. The recruitment packets included a letter from the Centers for Disease Control and Prevention (CDC), explaining the purpose of the survey, instructions for completing the self-administered survey via paper or a web-based response system, and a US$20 cash incentive. The recruitment materials explained the voluntary nature of the survey, and written informed consent was not obtained. In all, 2023 of 2208 providers were determined to be eligible, and 1234 of the eligible providers returned surveys (American Association for Public Opinion Research RR3 = 64% 19 ) from 391 HIV care facilities. The data were then weighted based on probability of selection, and response propensity adjustments of the design weights were performed to correct for possible nonresponse bias. Nonresponse adjustments were made to the sampling weights based on provider and facility factors associated with nonresponse: provider profession, number of HIV care providers practicing at the facility, facility university affiliation, whether the facility was a private practice or a community health center, and whether the facility had a computerized system for medications or lab results.
The 2013 MMP provider survey instrument consisted of 61 questions and required approximately 30 minutes to complete. For this analysis, we focused on provider-delivered services intended to reduce HIV transmission risk in 2 areas: sexual behaviors and alcohol and drug use (“substance use”). Each provider was asked whether they provided each of 9 sexual behavior–related and 7 substance use–related HIV transmission RR services to most or all of their patients (Table 1). We constructed 2 composite variables indicating “adequate” sexual behavior–related and substance use–related HIV transmission RR service delivery, using a standard of approximately 70% of services delivered. 20 Adequate sexual behavior–related RR was defined as providing at least 7 of 9 sexual RR services for most or all of the provider’s patients (or 6 of 8 in the case of providers who did not see patients at initial visits). Adequate substance use–related RR was defined as providing at least 5 of 7 substance use RR services for most or all of the provider’s patients (or 4 of 6 in the case of providers who did not see patients at initial visits) among providers seeing PWID. Independent variables were chosen based on prior studies of provider-delivered HIV transmission RR 7,9,13 and included age, gender, sexual orientation, race/ethnicity, provider type, years caring for HIV patients, primary care provision, language, number of patients, satisfaction with support services, having sufficient time to see patients, and patient characteristics. Also examined was HIV specialist designation, which was based on meeting criteria established by the HIV Medicine Association 21 or the American Academy of HIV Medicine, 22 and utilization of an integrated team, which was defined as multiple clinicians working together to augment the provider visit by providing pre-visit, post-visit, or between-visit contact with HIV-infected patients.
Prevalence of HIV Transmission Risk-Reduction Services—2013 MMP Provider Survey, United States.
Abbreviations: CI, 95% confidence interval; HSV-2, Herpes simplex virus 2; MMP, Medical Monitoring Project; STD, sexually transmitted diseases.
aAdequate sexual behavior–related RR was defined as performing at least 7 of 9 sexual behavior–related RR activities for most or all patients who met certain characteristics (6 of 8 services for providers who did not see patients for initial visits).
bCoefficient of variation is greater than 0.30, estimate may be unreliable.
cAdequate substance use–related RR was defined as performing 5 of 7 substance use–related RR activities for most or all patients who met certain characteristics (4 of 6 services for providers who did not see patients for initial visits; providers with no intravenous drug using patients were excluded).
We computed weighted estimates of percentages and associated 95% confidence intervals (CIs) to describe the target population of providers. Rao-Scott χ2 tests were used to test bivariate associations between selected independent variables and the 2 adequate RR services variables. All independent variables having associations of P < .05 were included in logistic regression models predicting the 2 dependent variables. Based on the examination of frequencies, number of HIV patients was also included in the models to assess whether there was a significant curvilinear association between this variable and the 2 dependent variables. Prevalence ratios for the independent variables were computed using methods described by Bieler et al. 23 All estimates incorporated the survey weights, and variance estimates were computed using Taylor Series Linearization to reflect the complex features of the MMP provider sample. We used SAS/STAT (version 9.3; SAS Institute Inc, Cary, North Carolina, USA) and SUDAAN (version 11; RTI International, Research Triangle Park, North Carolina, USA) procedures for the analysis of complex sample survey data, and considered estimates with a coefficient of variation greater than 0.3 unreliable.
Results
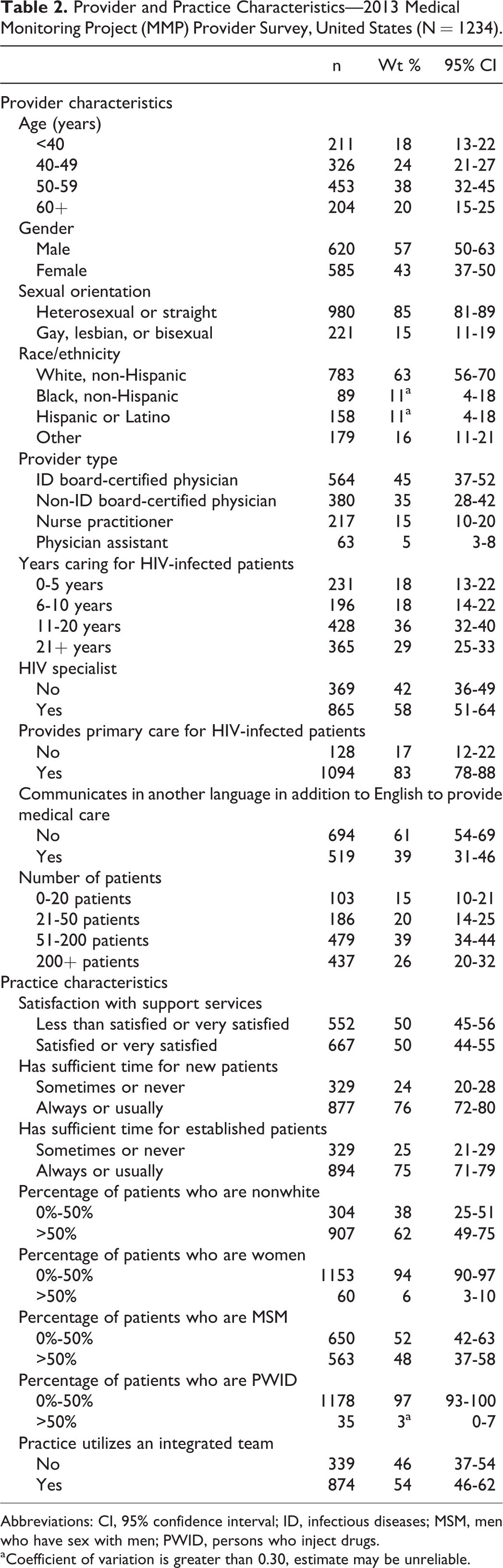
We estimate that the majority of HIV care providers in the United States in 2013 were over age 49 (58%), male (57%), heterosexual (85%), non-Hispanic white (63%), and physicians (medical doctors or osteopaths) (79%; Table 2). Over half were HIV specialists (58%) and most provided primary care to their HIV-infected patients (83%). About half (50%) were satisfied with the level of support services available in their practice and 54% utilized an integrated team in their practice.
Provider and Practice Characteristics—2013 Medical Monitoring Project (MMP) Provider Survey, United States (N = 1234).

Abbreviations: CI, 95% confidence interval; ID, infectious diseases; MSM, men who have sex with men; PWID, persons who inject drugs.
aCoefficient of variation is greater than 0.30, estimate may be unreliable.
The sexual behavior–related HIV transmission RR services most frequently provided to most or all patients were encouraging patient disclosure of HIV status to all sex partners (81%), asking patients newly diagnosed with an STD about disclosure of HIV status to sex partners (69%), and asking about HIV disclosure to all sex partners at a patient’s initial visit (62%; Table 1). Asking about HIV disclosure to new sex partners at follow-up visits (41%), offering condoms to sexually active patients (42%), and referring patients to partner services for assistance with notifying sex partners who had not been informed of their exposure to HIV (53%) were the services least likely to be provided to most or all patients. We estimate that 38% of providers offered condoms to few or none of their sexually active patients and 16% referred few or no patients to the health department for assistance with notifying sex partners who had not been informed of their HIV exposure. Screening for sexual risk behaviors and for symptoms of STDs in sexually active patients was only done for most or all patients by a little more than half of providers, and between 20% and 24% of providers did this for half or fewer of their patients. Examination of our composite variable indicates that adequate delivery of recommended sexual behavior–related RR services to most or all patients was low (37%).
The substance use–related HIV transmission RR services most frequently provided to most or all patients were assessing substance use every 6 months (64%) and encouraging patient disclosure of HIV status to all drug-injecting partners (61%; Table 3). Asking about HIV disclosure to new drug-injecting partners at follow-up visits (41%), informing PWID about sterile syringe sources (43%), and referral to partner services for drug-injecting partners that have not been informed of their possible exposure to HIV (45%) were the least likely to be provided to most or all patients. We estimate that 24% of providers discussed sources of sterile syringes with few or no patients who shared drug injection equipment and 20% referred few or no patients to the health department to discuss drug-injecting partners that had not been informed of their HIV exposure. Overall, adequate delivery of recommended substance use–related RR services to most or all patients was also suboptimal (43%).
Associations between Provider and Practice Characteristics and the Provision of Adequate Sexual Behavior–Related HIV Transmission Risk-Reduction Services—2013 MMP Provider Survey, United States (N = 1214).

Abbreviations: Wt, weighted; CI, 95% confidence interval; PR, prevalence ratio; CI, 95% confidence interval; aPR, adjusted prevalence ratio; Ref, referent; ID, infectious diseases; MSM, men who have sex with men; PWID, persons who inject drugs.
a P < .05; significance levels for PRs and aPRs were obtained from pairwise comparisons, based on the average marginal predictions.
b P < .01, significance levels for PRs and aPRs were obtained from pairwise comparisons, based on the average marginal predictions.
cCoefficient of variation is greater than 0.30, estimate may be unreliable.
Factors independently associated with providing adequate sexual behavior–related RR services were being an NP (adjusted prevalence ratio [aPR] 1.59), having 6-10 years of HIV care experience compared to over 20 (aPR:1.70), providing primary care (aPR:1.56), and having more than 50% of patients who were men who have sex with men (MSM; aPR:0.79; Table 3). Factors independently associated with providing adequate substance use–related HIV RR services were being an NP (aPR:1.59) and being an HIV specialist (aPR:1.27), and having more than 50% of patients who were PWID (aPR:1.56; Table 4).
Associations between Provider and Practice Characteristics and the Provision of Adequate Substance Use-Related HIV Transmission Risk-Reduction Services—2013 MMP Provider Survey, United States (N = 1207).
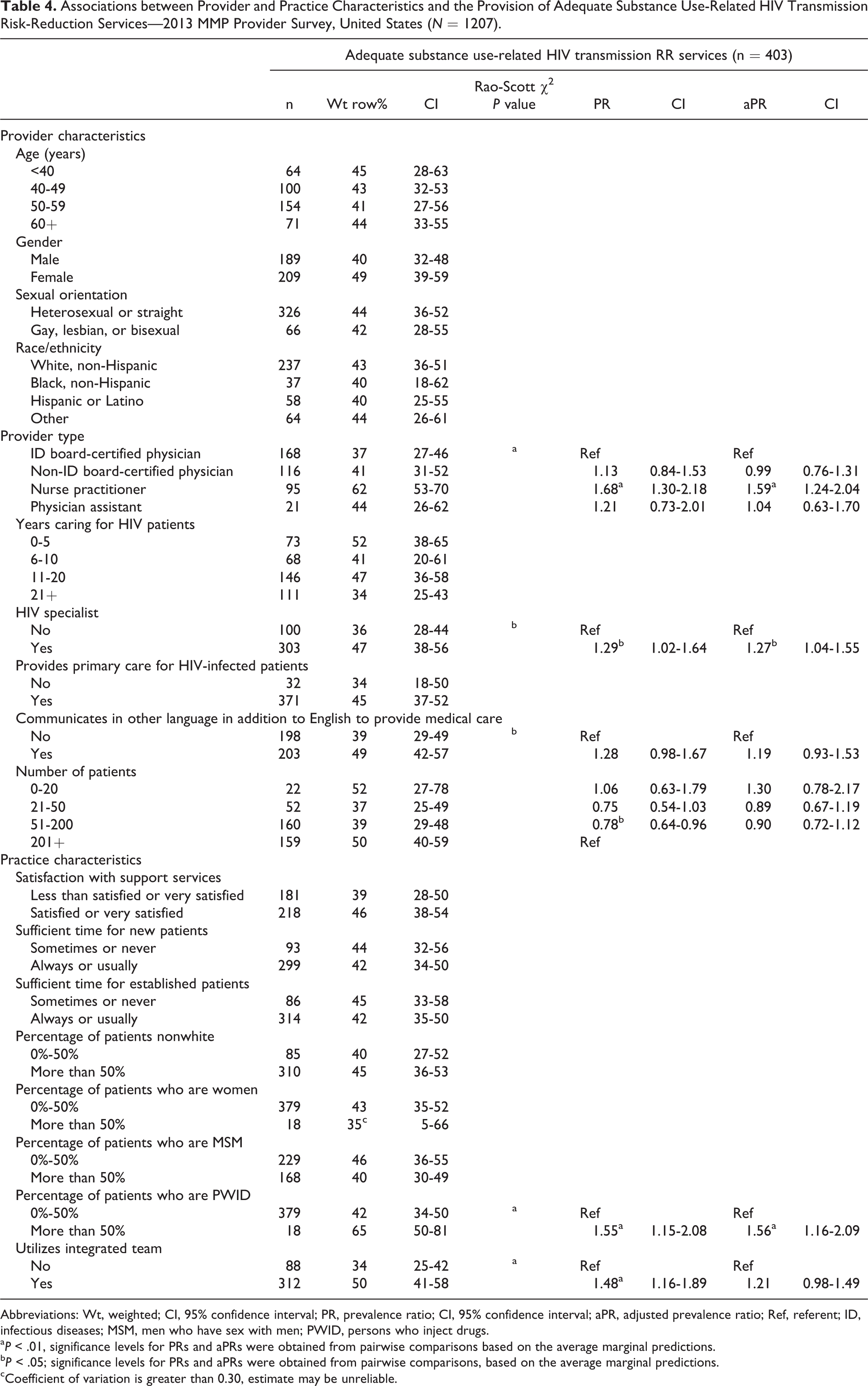
Abbreviations: Wt, weighted; CI, 95% confidence interval; PR, prevalence ratio; CI, 95% confidence interval; aPR, adjusted prevalence ratio; Ref, referent; ID, infectious diseases; MSM, men who have sex with men; PWID, persons who inject drugs.
a P < .01, significance levels for PRs and aPRs were obtained from pairwise comparisons based on the average marginal predictions.
b P < .05; significance levels for PRs and aPRs were obtained from pairwise comparisons, based on the average marginal predictions.
cCoefficient of variation is greater than 0.30, estimate may be unreliable.
Discussion
The majority of US HIV care providers may need additional support to improve delivery of comprehensive HIV transmission RR services to their patients. Services provided most consistently were those related to disclosure of HIV status to all sex and drug injection partners since HIV diagnosis and to sex partners at the time of an STD diagnosis, as well as assessment of alcohol and drug use every 6 months. Providers were least likely to ask patients at follow-up visits if any new sex or drug-injecting partners were notified of possible HIV exposure, to inform PWID about sources of sterile syringes, and to offer condoms to sexually active patients. The proportion of providers who refer patients to partner services for their sex and drug-injecting partners was also low.
Encouraging disclosure of HIV status to sex and drug-injecting partners at initial evaluations was more common than doing so at follow-up visits, as has been found by others. 9 Follow-up visits are generally allotted less time than initial visits, but we did not find an association between delivering adequate RR services and satisfaction with time spent with either new or established patients, as has sometimes been found by others. 13 Beyond the shorter time allotted to follow-up visits, providers may feel that discussing risk behaviors and HIV disclosure is not needed with patients who have not reported risk behaviors in prior encounters. However, because behaviors are dynamic and people with HIV are living longer, routine delivery of prevention services at follow-up visits is essential.
Delivery of services that require structural supports such as condom provision and information about sources of sterile syringes was also low. Delivery of these services may not entirely be at the discretion of the provider, as condoms and sterile syringes may not be available in all settings. For example, having condoms freely available to patients requires some coordination between the care facility and those who can provide the condoms, such as condom manufacturers or community-based prevention organizations. State and federal laws may affect the availability of syringe exchange and prescription options. However, the use of condoms and sterile syringes is effective behavioral interventions that reduce the risk of HIV transmission, and HIV care providers can be instrumental in promoting their use. Although free condoms may also be available from other sources (such as community-based organizations or social venues), health care settings are an important point of access. In 2011, approximately 64% of US HIV-infected patients who received free condoms obtained them from a general health clinic. 24
Consistent with prior work, referral to partner services for both sex and drug-injecting partners was also less frequently delivered. 7 Because health department–delivered partner services can be a cost-effective means of identifying new HIV infections and disrupting HIV transmission chains, 2 and early identification of HIV infection and subsequent ART improve the likelihood of treatment success and decreases the risk of onward HIV transmission, 25 enhanced efforts to increase provider referral of patients to partner services are warranted. The newly published Recommendations for HIV Prevention with Adults and Adolescents with HIV in the United States provides recommendations for clinical providers on strategies to establish infrastructure for HIV partner services. 2 Communicating with providers about partner services from a patient’s perspective may also help; evidence suggests that patient acceptability and safety are key factors in provider endorsement of partner services. 26
We found suboptimal levels of screening for sexual risk behaviors and for STDs among sexually active patients. This concurs with the findings of low levels of STD screening among US HIV patients. 27 Some providers may not be comfortable discussing sex with their patients, 28 but tools exist that may help providers enhance their skills in these areas. For example, “Ask, Screen, Intervene” and “Partnership for Health” are 2 interventions that provide courses, continuing education opportunities, and other materials to facilitate their implementation by clinicians. 29,30 Increasing service delivery in this area is essential because provider-delivered risk counseling can be effective in reducing sexual risk behaviors among HIV-infected persons. 2,5,6
Nurse practitioners were independently more likely to provide adequate sex and substance use–related HIV transmission RR services to their patients. Although the role of NPs in the delivery of HIV care has not been studied extensively, studies suggest that NPs provide similar quality HIV care as physicians. 31 In addition, several studies have indicated that NPs have similar primary care outcomes as physicians, but outperform physicians in measures of consultation time, patient-follow-up, and patient satisfaction. 32 This analysis supports the key role of NPs in delivering comprehensive prevention services for HIV-infected persons and helps inform the debate regarding the future role of NPs in the delivery of HIV care. 33 As the number of HIV-infected persons needing care grows annually, NPs may play an essential role in delivering needed HIV transmission RR services.
Having more than 50% MSM patients was independently associated with lower delivery of sexual behavior–related RR. This finding concurs with patient-level data in which MSM report lower receipt of prevention counseling than other groups. 10 Enhanced efforts to improve this gap may be needed, as the risk of sexual transmission of HIV is substantially higher for MSM who engage in anal intercourse. 34 Although biomedical prevention strategies such as Treatment as Prevention and pre-exposure prophylaxis (PrEP) may hold great promise for populations disproportionately affected by HIV such as MSM, they will not supplant the need for continued delivery of RR services. An estimated 38% of HIV-infected persons receiving medical care in 2011 had at least 1 unsuppressed viral load test result over the prior year, 16 which indicates a continued need for behavioral strategies to decrease the risk of HIV transmission among sexually active persons and PWID in this group. Also, the success of PrEP as a prevention strategy may depend on expanding provider education and training programs so that all at-risk persons have access to PrEP. An analysis of 2013 MMP Provider Survey data found that only an estimated 26% of US providers who care for HIV-infected and non-HIV-infected patients reported ever prescribing PrEP. 35
That providers who also deliver primary care are more likely to deliver sexual behavior–related RR is encouraging and may indicate the complementary nature of HIV and primary care training. As the Institute of Medicine notes, as HIV-infected persons are living longer, there is an increased need for primary care skills among HIV care providers in order to meet their patients’ health needs. 36 As the Affordable Care Act provides funding to community health centers to enhance HIV care and treatment services, a growing number of HIV-infected persons may receive care from primary care providers and NPs, which may enhance delivery of RR services.
Having more than 50% PWID as patients was independently associated with delivery of substance use–related HIV transmission RR services, which may reflect the increased expertise and comfort with discussing substance use that comes with seeing larger numbers of patients for whom these services may be relevant. Also, providers who see many PWID may have more confidence in their ability to identify those in need of these services. Meeting HIV specialist criteria was also associated with being more likely to deliver substance use–related HIV transmission RR services. Although HIV specialist certification differs somewhat from credentialing through certification programs, given the recent debate about the value of maintaining certification programs and the difficulty in demonstrating their effect on quality of care, 37 this finding may warrant further exploration.
Our analysis is subject to several limitations. First, we did not assess delivery of every possible sexual behavior– and substance use–related RR service, for example, delivery of more intensive behavioral RR interventions. However, we assessed a wide range of basic services that capture the minimum standard for provider-delivered RR. Second, our estimates of delivery of RR services are self-reported and may be subject to recall and social desirability bias. However, our findings concur with studies using direct observation methods, which have also found low rates of provision of these services. 11,12 Third, we did not measure the quality or quantity of services delivered, so we cannot determine whether the delivery of services by providers was adequate to meet the patients’ needs. For example, while Drainoni and colleagues 28 found that almost all providers they surveyed discussed risk behaviors and transmission with their HIV-infected patients, most did not routinely probe for the reasons for risk behaviors and thus missed opportunities to provide effective counseling to reduce these behaviors. Fourth, we were unable to fully assess delivery of RR services by provider race/ethnicity because the numbers of black and Hispanic providers were low, leading to unstable estimates with wide confidence intervals. Future surveys could oversample nonwhite providers to address this limitation. Fifth, the MMP Provider Survey is designed to produce national estimates, but participating states may be able to generate locally representative estimates. Such analyses may be useful for evaluating the adequacy of local RR services and determining what changes are needed to improve the delivery of these services. Sixth, in some care settings provision of selected prevention services may be performed by nonclinical staff, and thus providers may not provide the service so as not to be duplicative. However, provider-delivered RR has been found to be especially effective in reducing risk behavior, 5 and provider awareness of patient risk behavior is essential for providing quality medical care, for example, for determining the need for STD screening. 2 –4 Finally, while we chose to use a threshold of approximately 70% of services delivered for our composite measures, it is important to acknowledge that all services we examined are recommended by federal guidelines. 2 Despite this, we did not choose a threshold of 100% of services delivered because, as mentioned earlier, some services examined (eg, condom provision, referral to partner services) require structural supports that are not entirely within the control of the provider. Also, because 100% delivery (or “all-or-nothing”) measures are sensitive to the number of items included in the composite measure, a 70% threshold has been suggested as an alternative measure of clinical quality. 20 Because all services examined are recommended by federal guidelines, we decided to give all services equal weight in the construction of our composite measures.
Despite biomedical advances in prevention strategies, supporting behavior change through RR services remains an essential component of an effective combination approach to HIV prevention. The recent publication of the updated federal recommendations for HIV prevention with persons with HIV 2 provides an opportunity to refocus efforts on these important services. The HIV-infected population is growing as a result of a stable number of annual new infections and increasingly effective treatments that reduce mortality. Further, as our national efforts to move individuals along the continuum of care result in increases in numbers of HIV-infected persons engaged in medical care, it is crucial that we ensure that providers of HIV care are aware of recommended prevention services and that they are provided with adequate training and support to assess and address HIV transmission risks among their patients. This analysis presents evidence that comprehensive transmission RR services are not delivered by a majority of providers to most of their patients and identifies specific services that are in need of enhancement, such as RR at follow-up visits and referral to partner services. CDC has compiled a list of existing resources to support implementation of federal guidelines for HIV prevention (http://www.cdc.gov/hiv/prevention/programs/pwp/resources.html) and will continue to monitor the delivery of these services through provider surveys and other efforts to ensure that all persons with HIV are receiving needed services to prevent onward transmission and improve their health.
Footnotes
Authors’ Note
The findings and conclusions in this report are those of the authors and do not necessarily represent the views of the Centers for Disease Control and Prevention.
Acknowledgments
The authors thank the participating Medical Monitoring Project (MMP) providers, facilities, project areas, and Provider and Community Advisory Board members. The authors also acknowledge the contributions of the Clinical Outcomes Team, the Behavioral and Clinical Surveillance Branch, other members of the Division of HIV/AIDS Prevention at CDC, and the MMP 2013 Study Group Members: ![]() . Finally, the authors thank the Altarum Institute data collection team.
. Finally, the authors thank the Altarum Institute data collection team.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Sources of funding: The Medical Monitoring Project Provider Survey is funded by the Centers for Disease Control and Prevention.