
Abstract
A randomized controlled trial is being conducted in the United States to test the efficacy of a personalized interactive mobile health intervention (iSTEP) designed to increase physical activity (PA) and improve neurocognitive functioning among HIV-positive persons. This article describes an initial qualitative study performed to develop iSTEP for the HIV-positive population, including assessment of PA barriers and facilitators. Two focus groups, with 9 and 12 unique HIV-positive individuals, respectively, were administered to evaluate barriers limiting PA and potential iSTEP content created to encourage greater PA. Group discussions revealed prominent PA barriers, including HIV symptoms (neuropathy, lipoatrophy), antiretroviral medication effects, and fatigue; significant PA facilitators included self-monitoring and family support. Participants provided feedback on strategies to increase PA and expressed positive support for a mobile intervention adapted to personal priorities. These findings will assist the development of novel PA interventions focused on treating the epidemic of HIV-associated neurocognitive disorders.
Introduction
Although combination antiretroviral therapy (cART) has dramatically reduced AIDS-related morbidity, 1 HIV-associated neurocognitive disorders (HAND) remain prevalent. 2 HIV-associated neurocognitive disorders, which may involve deficits in executive function, attention, and memory, continue to represent a significant public health concern linked to impaired everyday functioning and poor quality of life among persons with HIV infection. 2 Despite the widespread incidence of neurocognitive deficits in the HIV-positive population, few studies have evaluated methods to compensate for this phenomenon, and there are no currently validated therapies to effectively treat HAND symptoms. 3
Physical activity (PA) has been utilized as an effective nonpharmacological method to improve cognitive performance among elderly individuals and patients with dementia. 4,5 Observational studies reveal a similar positive association between active lifestyle factors, including PA, and neurocognitive outcomes among HIV-positive persons. 6 –8 Although interventions to promote PA among HIV-positive persons have reported improvement in cardiopulmonary fitness, 9,10 the effects of PA interventions on HAND have not been characterized.
Recent short message service (SMS) interventions have successfully increased moderate PA associated with significant health benefits. 11 The aim of the parent project is to conduct a randomized controlled trial that utilizes a personalized interactive text messaging intervention to increase PA and subsequently improve neurocognitive functioning in HIV-positive participants with HAND. The purpose of this qualitative study was (1) to identify key PA barriers and facilitators for HIV-positive persons and (2) to obtain feedback for the development of a PA mHealth intervention (iSTEP) addressing the specific needs of the HIV-positive population. These findings will provide a foundation for the future refinement of mobile PA interventions dedicated to treating HAND.
Methods
Participants
Two focus groups, one with 9 and the other with 12 unique HIV-positive individuals, were conducted in fall 2013 for a total of 21 participants. Participants were recruited from ongoing studies of HIV infection at the HIV Neurobehavioral Research Program (HNRP) that receive referrals from HIV clinics. Participants had a confirmed HIV diagnosis, and half (10/21) met criteria for HAND based on comprehensive neuropsychological testing at the HNRP, following established guidelines 2 ; no other inclusion/exclusion criteria were applied. HIV-associated neurocognitive disorder is characterized by periods of remission as well as decline, and PA interventions may prevent or slow the development or reoccurrence of HAND in cognitively intact individuals. Therefore, the inclusion of participants with and without HAND allowed us to capture a broad range of perspectives to inform intervention development. Study approval was obtained from the local institutional review board. Each participant provided written informed consent for the study and received monetary compensation (US$35).
Intervention
The objective of the focus groups was to inform a 4-month SMS/multimedia message service (MMS) intervention (iSTEP) designed to increase moderate PA in HIV-positive persons with HAND. The iSTEP intervention, based on control theory principles of self-regulation, 12 uses SMS text prompts and MMS images to promote PA self-monitoring, facilitate personalized PA goal setting, and provide feedback on progress toward increasing PA.
Focus Group Procedure
We conducted 2 focus groups, each 1.5 hours, with semioverlapping content to increase the number of perspectives. Group moderators initiated discussion with a series of predetermined nonleading open-ended questions and asked follow-up questions to elicit additional opinions from the group. Group 1 acquired information about PA barriers and facilitators for people with HIV, and group 2 solicited feedback on potential intervention content (eg, text message topics, SMS frequency and timing). Group discussion was audiotaped and subsequently transcribed verbatim and blinded for review, that is, deidentified participants were assigned coded labels.
Data Analysis
Transcripts were independently coded at a general level by 2 investigators based on emergent themes. The description or assignment of codes was determined by consensus among all study investigators. The selected code list consisted of themes related to PA barriers and facilitators and discussion content related to iSTEP. Interrater reliability of the coded statements had a kappa value of 0.87, indicating high rater concordance. Data analysis was performed using QSR International NVivo9 data analysis software.
Results
The participants were middle aged (47.5 years, SD = 5.6), predominantly male (95%) and Caucasian (67%), with some college education (13.2 years; SD = 3.0). The open-ended questions used to guide the focus group discussions elicited a variety of responses from participants, and our qualitative analysis uncovered an assortment of main themes for each question. These are outlined in Tables 1 and 2, including representative participant statements. Below we present the findings regarding PA barriers and facilitators and preferences for iSTEP content.
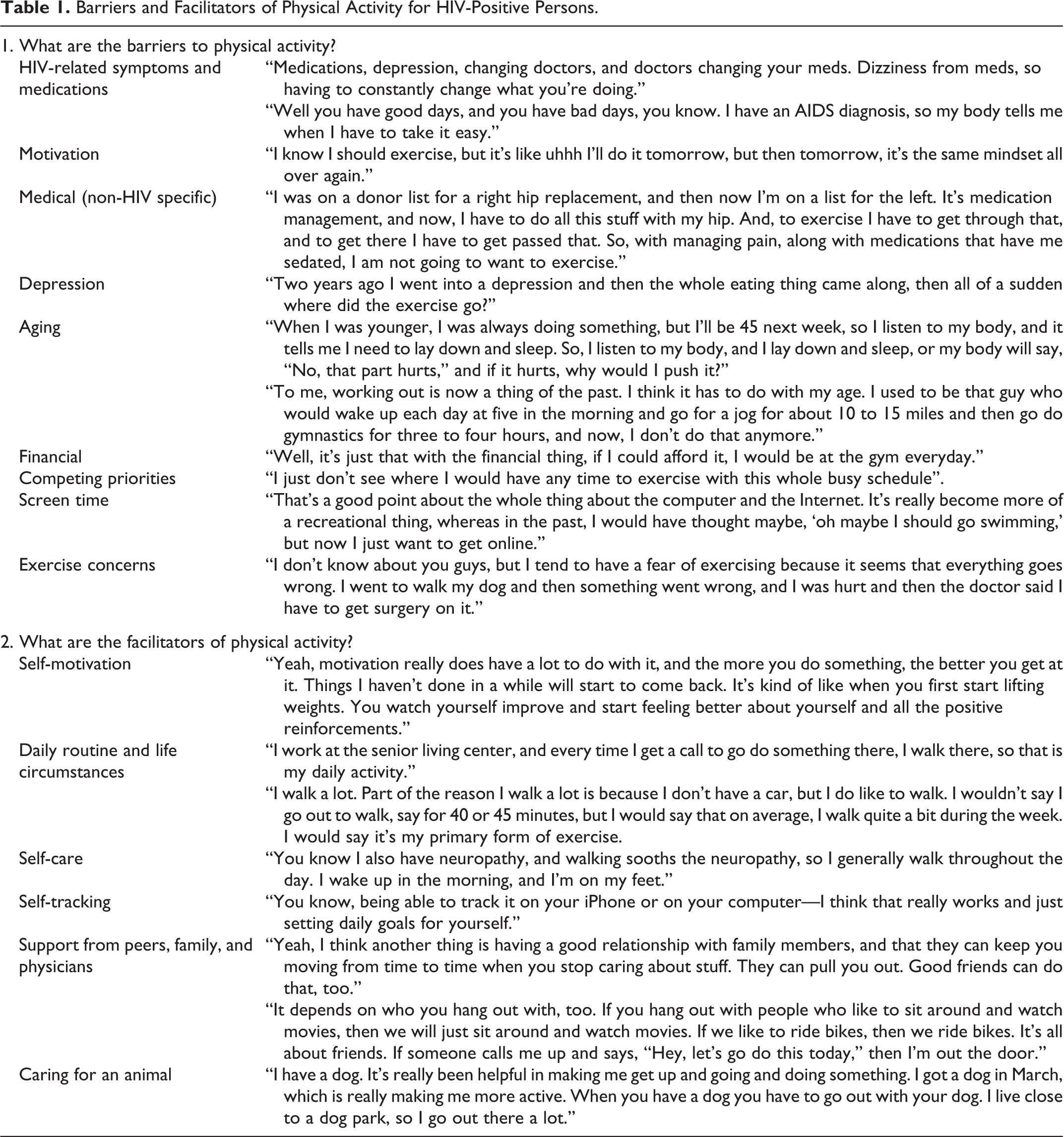
Barriers and Facilitators of Physical Activity for HIV-Positive Persons.
Focus Group Feedback on the Delivery and Content of an mHealth Intervention to Promote Physical Activity.

aName of park redacted for participant confidentiality.
Physical Activity Barriers
Analysis of the focus group transcripts identified 9 thematic barriers to PA among HIV-positive persons: (1) HIV-related symptoms and medications, (2) decreased motivation, (3) general medical conditions, (4) depression, (5) aging, (6) financial concerns, (7) competing priorities, (8) screen time, and (9) exercise concerns. HIV symptoms limiting PA included peripheral neuropathy and leg fat lipoatrophy as well as negative side effects of medications (eg, nausea, dizziness, and diarrhea). Decreased motivation included continuously putting off exercise until tomorrow, feeling unmotivated due to self-doubt, being comfortable with an inactive lifestyle (ie, “a body at rest stays at rest”), allowing boredom to forestall activity, and not feeling up for, or wanting to, exercise. Other medical conditions that inhibited PA included comorbidities such as Parkinson disease, hip replacements, respiratory problems, and the belief that exercise is ineffective at lowering cholesterol and triglyceride levels. Depression served as a barrier for PA in regard to not wanting to do anything (eg, not leaving one’s house). Aging encompassed “listening to the body” (eg, “if the body hurts, why push it?”), self-doubt about getting older and “having a belly,” and regarding “working out” as a thing of the past. Financial concerns were a prominent PA deterrent, with many members disclosing difficulty affording gym memberships or being too busy trying to find a job. Competing priorities (ie, busy schedules and life demands) suggested that PA was a secondary concern and thus neglected. Screen time referred to the overuse of recreational electronic media, including excessive time watching television or using the Internet. Exercise concerns included lack of knowledge of how to use gym equipment and fear of sustaining an exercise-related injury.
Physical Activity Facilitators
Seven themes emerged as PA facilitators in the focus groups: (1) self-motivation, (2) daily routine and life circumstances, (3) self-care, (4) self-monitoring fitness/activity, (5) social support, (6) animal care, and (7) incentives. Self-motivation entailed making an effort to exercise (eg, using stairs instead of elevator); wanting to reinvent oneself; setting personal fitness goals; wanting to get out of the house; and walking to avoid medical complications, to improve quality of life or self-esteem. Physical activity was encouraged by daily routine or life circumstances (walking in lieu of owning a car, choosing to walk instead of taking public transit, and maintaining a daily routine outside the house). Self-care involved walking to soothe neuropathy, preventing health conditions by performing PA, and exercising to stabilize mood. Self-monitoring via phone apps and pedometers encouraged PA. Social support from peers, family, and physicians entailed having walking/exercise buddies, caring for children, having active friends, competing with others, and listening to physician health advice. Animal care provided an avenue for PA engagement (ie, walking a dog). Incentives were regarded as effective motivators to encourage participant effort to win a competition or prize.
Text Messaging Intervention Content to Promote Physical Activity
Several iSTEP intervention components were considered in the groups. Of note, participants held various views about SMS content to support PA, with some advocating for directive messages (eg, “Get your butt in gear!” and “Get outside!”), others encouraging the use of inspirational messages (“You can do it!,” “Your life is worth it!”), whereas a few simply wanted to be asked if they had engaged in PA rather than receiving encouragement to do so. Participants unanimously encouraged the use of messages to set PA goals based on step counts recorded via a pedometer and supported walking as a feasible option. There was a discrepancy about whether text messages related to HIV disease status were helpful. Participants requested that messages be unique for each person, as some did not mind receiving messages asking about HIV-related issues (eg, neuropathy), whereas others did not want to be asked if HIV symptoms prevented them from achieving PA goals. Discussion of personalized or generic messages revealed individual differences (eg, “I want personalized messages” versus “generic messages are fine”). Some participants supported receiving MMS graphs that charted PA progress, whereas others did not like the idea of receiving picture messages. In regard to confidentiality, many indicated that having sole access to their phone was sufficient, whereas others requested generic messages to provide additional privacy. Participants indicated varied preferences for message frequency (1 to 4 times a day) and further reported that a higher number of daily texts would lose impact. Varied preferences for text message timing were also reported (ie, messages at a specific time everyday compared to a variable range), although participants uniformly liked 2-way communications (ie, receiving and sending messages). Some advocated for additional components to help with PA adherence, such as incentives and interparticipant interaction (eg, participant competition or receiving feedback when other participants achieved goals).
Discussion
Focus group discussion yielded identification of prominent PA barriers and facilitators, informing the development of a novel SMS/MMS intervention to promote PA among HIV-positive individuals with HAND. A myriad of preferences regarding SMS/MMS delivery and iSTEP content illustrated the benefits of adopting a personalized approach to promote the acceptability and scalability of mHealth interventions.
Physical activity may represent an effective strategy to address the significant health challenges faced by an aging HIV-positive population, including the widespread incidence of cardiovascular disease, metabolic syndrome, and neurocognitive deficits that persist in the cART era. 13 Few studies have examined free-living PA (ie, performed around the home environment), although one report confirms that HIV-positive persons engage in less exercise than is recommended by the US Centers for Disease Control and Prevention. 14 Previous PA interventions with HIV-positive persons have involved rigorous PA (eg, running on a treadmill) 15 and significant participant resources (eg, supervised exercise requiring weekly travel to a gym) 16 that the focus group discussions indicated may be impractical for many persons with this disease. For example, several participants voiced concerns about the potential for exercise-related injuries and described feeling unfamiliar with gym equipment. Many participants described a lack of transportation as a barrier to “formal” PA but noted that they can and do walk to conduct errands or appointments, sometimes in lieu of public transportation. Of note, previous studies indicate that relatively small PA increases (adding 500 pedometer step counts per day) are associated with improved neurocognitive functioning, 17 which may be feasible even with physical limitations noted by the focus group participants (eg, peripheral neuropathy, hip replacements, and Parkinson disease). Thus, the aim of the iSTEP intervention will be to provide support via SMS/MMS to encourage participants to increase moderate PA (eg, the number of steps they walk).
The current study demonstrates a content development approach for promising mHealth interventions; however, several limitations deserve mention. Multiple focus groups are preferable to identify themes until saturation is reached. Our relatively small sample may not have covered additional relevant themes, and/or additional theme modifications may not have been revealed. Demographic factors may have influenced response variability in our predominately male Caucasian sample; thus, future observational and intervention studies with greater minority and female representation would help to address the needs of the diverse HIV-positive population. Although our focus group members were amendable to an mHealth intervention promoting PA, a prospective clinical trial is needed to determine actual acceptance and compliance. Despite these limitations, the perspectives of persons living with HIV remain important for developing interventions, and several thematic approaches for targeting PA engagement were explored in these focus groups.
This qualitative study demonstrates the feasibility of using focus groups to derive patient-centric intervention content to address health challenges. The study identified PA barriers and facilitators for people living with HIV and lends support to tailored intervention strategies adapted for this population. Further research may aim to (1) investigate the usefulness of SMS/MMS technology to promote PA and (2) explore the efficacy of user-controlled settings (eg, controlling message timing). Such research is strongly warranted in an effort to develop validated methods that effectively treat symptoms of HAND.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: supported by NIMH grants R21 MH100968, R01 MH099987-02S1, and P30 MH062512.