
Abstract
Study Design:
Case report.
Background:
Twenty-five percent of people living with HIV/AIDS (PLWHA) are also coinfected with hepatitis C virus (HCV). There are limited reports to assist in the symptom management of PLWHA and HCV coinfection.
Case Description:
Our case was a 67-year-old man living with HIV/HCV coinfection and other medical complications. Our intervention consisted of a 6-week progressive conditioning program, while his activity and sleep pattern were monitored using a wrist accelerometer.
Outcomes:
After completing a conditioning training, there was a 64% decrease in the number of waking episodes per night and 68% decrease in activity at night. Based on Pittsburgh Sleep Quality Index scores, the participant transitioned from being a “poor sleeper” to a “good sleeper.” A 40% decrease in pain was reported. Functional outcome measures also showed improvements.
Discussion:
There were improvements in the participant’s sleep quality and pain. The use of a commercial accelerometer may assist in objectively tracking compliance and activity changes.
Background
The current advances in antiretroviral therapy (ART) have led to an increased life span of people living with HIV/AIDS (PLWHA) by suppressing the rate of HIV replication in seropositive individuals. 1 The goal of ART is maximum viral suppression and preservation of immune function, which is monitored by viral load (VL) values and CD4 (or T lymphocyte) counts. The most recent report from the Centers of Disease Control and Prevention estimates the number of PLWHA in the United States at approximately 1.1 million, with roughly 50,000 Americans added to this total every year. 2
Chronic pain, independent of its etiology, is often reported to be associated with sleep disturbances, poor sleep quality, poor sleep efficiency, and decreased quantity of sleep. 3,4 A negative impact on sleep, pain, mobility, and endurance has been commonly associated with living with HIV infection. 5 –7 People living with HIV/AIDS have a high incidence of chronic pain, with estimates suggesting that 60% to 90% of these individuals report experiencing moderate to severe pain on a regular basis. 5 –8
People living with HIV/AIDS exhibit functional performance levels that closely resembled those observed in seronegative cohorts who are 20 years older. 5,6 Sandoval et al 5 proposed an association model between pain, sleep, and function in PLWHA and peripheral neuropathy. The authors described a relationship between these variables, where pain directly influenced sleep quality and, in turn, affected functional performance in this patient cohort. Conversely, HIV disease markers and self-reported pain did not appear to exert a direct or significant association with functional performance in this study. 5
The hepatitis C virus (HCV) shares similar infection transmission mechanisms with HIV; therefore, it is not an uncommon comorbid condition in PLWHA; of the 1.1 million PLWHA, it is reported that 25% live with HCV coinfection. 2 People living with HIV/AIDS and HCV are reported to exhibit 3 times greater risk for cirrhosis of the liver, liver failure, and liver-related death than people living with HCV infection alone. 2,9 Additionally, individuals with chronic liver damage leading to cirrhosis demonstrate decreased exercise capacity and muscle strength. People living with chronic liver damage appear to exhibit peak oxygen volumes (VO2peak) that are 60% to 82% of the predicted value for non-HCV community-dwelling individuals. 8 Thus, the systemic effects associated with HIV/HCV coinfection can potentially converge to compound the negative impact on function in these individuals.
There are limited reports to guide clinicians on how to best manage sleep disturbances, pain, and deconditioning in individuals living with HIV/HCV coinfection. Exercise-induced hypoalgesia has been reported to be effective in managing chronic pain at low to moderate levels of exercise intensity. 10 Compliance with prescribed exercises is often a major hurdle to overcome in PLWHA, as adherence is generally less than what is required to reach these conditioning and analgesic goals. 11 The purpose of this case report is to share our experience in managing sleep and pain disturbances in a person living with HIV/HCV coinfection and chronic pain while using a consumer-based wrist accelerometer to objectively monitor activity levels and sleep.
Case Description
History
The participant was a 67-year-old white man who was diagnosed with HIV infection in 2000. A review of the medical record revealed HCV coinfection, a history of chronic pain, HIV-related peripheral neuropathy, hypertension, hypothyroidism, and radiological findings of stenosis at the cervical and lumbar spinal segments without evidence of cord compression.
Medications
At initial assessment, he was on an ART regimen for HIV infection, consisting of once-daily (QD) formulation of efavirenz (EFV)/emtricitabine/tenofovir (TDF) 600/200/300 mg. To manage his pain, he was prescribed acetaminophen/hydrocodone 355/10 mg 4 times daily and QD aspirin 325 mg. He was prescribed QD lisonopril/hydrochlorothiazide 20/25 mg for hypertension and levothyroxine 25 mg to manage his hypothyroidism. He had declined HCV, citing concerns with side effects and length of treatment.
Laboratory Values
The participant’s pertinent laboratory values were as follows: CD4 (or T lymphocyte) count of 130 cells/mL, CD4/CD8 ratio of 0.22, and HIV VL of 29 RNA copies/mL. Although very small, active HIV replication was present in view of detectable HIV RNA serum levels. An undetectable VL value is noted, with HIV RNA copies of less than 20 RNA copies/mL. As of November 2010, his HCV VL was measured at 2 383 628 RNA copies/mL, and no recent HCV follow-up was conducted as he had declined treatment.
Additional Pertinent Findings
On examination, he reported a history of chronic low back and bilateral hip pain as well as neuropathic pain for the past 20 years. No evidence or reports of avascular necrosis or other significant orthopedic condition was noted. He reported a history of intravenous drug use, alcohol abuse, and smoking for the past 50 years at a rate of ½ pack/d or a 25 pack-year exposure to tobacco products.
Pain
When taking his pain medications, the participant reported 1/10 low back pain and 10/10 bilaterally at the hips. Prolonged sitting, standing postures, and walking greater than 1 block were reported as primary aggravating factors of pain at the low back and hips. The participant did not use an assistive device to ambulate or function at the household level. He was unable to identify any pain alleviating factors other than current medications.
Outcome Measures
The following outcome measures were chosen to identify changes attributed to the physical therapy program: (1) The Pittsburgh Sleep Quality Index (PSQI) to measure the quality of sleep; (2) The Oswestry Disability Index (ODI) to measure pain and disability; (3) The modified Bruce protocol for the assessment of aerobic capacity; (4) The 6-minute walk test (6MWT) to determine aerobic functional ambulation endurance; (5) Timed Up and Go (TUG) to evaluate balance, gait speed, and fall risk; and finally (6) hand grip strength to obtain a global measure of strength. The data collected from all outcome measures are represented in Table 1.
Outcome Measures.

Abbreviations: L, left; ODI, Oswestry Disability Index; PSQI, Pittsburgh Sleep Quality Index; R, right; TUG, Timed Up and Go; 6MWT, 6-minute walk test.
aGood sleeper < 5.
The PSQI cutoff scores have been reported to differentiate between “good sleepers” 5/21 or less and “poor sleepers,” with scores greater than 5/21 on this scale. 12 At the initial evaluation, the participant’s score of 7/21 categorized him as being a poor sleeper. The participant scored 24% disability on the ODI. An individual whose score is between 20% and 40% on the ODI is categorized as being associated with moderate levels of disability. Individuals with similar ODI scores are classified as having an increase in pain during sitting, lifting, and standing. 13 On the modified Bruce protocol, he was able to complete 30 seconds of stage II (2.7 km/h, 5% grade, or approximately 3.0 metabolic equivalents [METs]) with a final heart rate (HR) of 95 beats/min and a blood pressure reading of 150/65 mm Hg. The participant requested to stop the test due to bilateral calf cramps. The clinical functional measures of the 6MWT, TUG, and grip strength were assessed at the initial encounter. The participant walked a distance of 144.5 m in 3.minutes and 32 seconds; he requested to stop citing pain at the hips. He completed the TUG in 15.3 seconds and demonstrated grip strength of 33 kg on the right and 30 kg on the left hand.
Other Physical Findings from Initial Evaluation
The participant exhibited full active range of motion in both upper and lower extremities bilaterally. He had absent vibratory sensation at the right medial malleolus. He demonstrated a hyporeflexive deep tendon reflexes (DTRs) at the right patella and absent DTR bilaterally at the plantar flexors. The lumbar spine and hips clinical examination was unremarkable. We were unable to reproduce low back pain during the examination of the lumbar spine.
Activity and Sleep Monitor
One week prior to the initial evaluation, the participant used a Fitbit Flex (Fitbit Inc, San Francisco, California, USA) accelerometer. The Fitbit Flex is a wrist accelerometer that may be worn 24 hours a day to monitor daily activity and sleep. The accelerometer synchronizes with the manufacturer’s software to record steps taken, calories burned, distanced traveled, active minutes, total hours slept, and number of times awakened during sleep. 14 The participant was instructed to wear the wrist accelerometer 24 hours a day for the duration of the intervention. Data were synced at each treatment session, and the device was monitored for battery life and proper functioning. All activity and sleep data were manually retrieved and logged.
Clinical Impression
The participant demonstrated decreased cardiovascular endurance and poor activity tolerance, based on his physical performance on the modified Bruce protocol, 6MWT, TUG, and grip strength when compared to age-matched individuals. 5,6,15,16 He was categorized as being a poor sleeper and exhibited “moderate disability” from his chronic back pain. The participant’s complex clinical picture and history of comorbidities all were deemed to negatively affect his functional status. He stated a goal for therapy to assist in decreasing fatigue and pain during daily activities. We hypothesized that a comprehensive conditioning program with close monitoring for pain and fatigue would be best suited to address his complaints. He agreed to the intervention and demonstrated compliance with all recommendations during the entire intervention.
Intervention
A conditioning program was structured as an “A-B-AB” intervention. The 3 phases of the intervention comprised (A) 3 sessions per week for 2 weeks of manual stretching and cardiovascular training, (B) 3 sessions per week for 2 weeks of resistance training, and (AB) 3 sessions per week for 2 weeks of circuit training with cardiovascular and resistance training.
Cardiovascular training (intervention A)
A cardiovascular training regimen was structured based on the American College of Sports Medicine’s (ACSM) recommendations for PLWHA and the maximum METs reached on the modified Bruce protocol. The ACSM recommends brisk walking or biking for 30 to 60 minutes, 3 to 4 days a week at 40% to 60% intensity of the Karvonen heart rate (HRtarget = [{HRmax − HRresting} × % intensity]). 17 The first 2 weeks, he trained at 40% intensity, with 100 bpm being his maximum HR. Each session consisted of three 10-minute bouts of aerobic exercise, with intermediary rest breaks ranging from 1 to 5 minutes in length. Each treatment session began with manual stretching of bilateral gluteal, piriformis, hamstring, and hip internal rotator muscles. Each session of the cardiovascular training was conducted by alternating between a treadmill and a recumbent bicycle. During week 1, the participant trained at 1.8 METs. During week 2, he exercised at 2.0 to 2.5 METs.
Resistance training (intervention B)
A recent Cochrane review by Liu and Latham 18 reported that training older adults at 80% to 90% of their 1 repetition maximum (1 RM) lead to improved physical function and strength. When training an individual at this level of effort, the authors suggested 3 sets of 4 to 6 repetitions. 18 On session 1 of week 3, the participant’s 1 RM was established using a Nautilus-NS 4000 multigym (Nautilus Inc, Vancouver, Washington, USA) for the military press, seated row, latissimus pull downs, reverse fly, leg press, knee extension, and hamstring curls. A weight lifting program was drafted to train him at the recommended 80% of the 1 RM at the rate of 3 sets of 4 repetitions for each exercise.
Circuit training (intervention AB)
During the final 2 weeks of the intervention, the participant trained using a combination of cardiovascular and resistance training. The participant would complete 3 circuits per session, with 1 circuit consisting of 10 minutes of cardiovascular exercise followed by 6 to 7 minutes of resistance exercises. The previously established cardiovascular and strength training parameters were combined for remainder of this training phase.
Outcomes
At the end of the 6-week intervention period, the participant performed the modified Bruce protocol, PSQI, ODI, TUG, and grip strength. The data obtained in the selected outcome measures are reported in Table 1.
Accelerometer Data
There are few reports in the literature appraising the validity of quantifying sleep and activity by accelerometers, such as the one used in this case report. Commercially available accelerometers have been compared to the gold standard of polysomnography to evaluate the validity and reliability of the quality and rate of disturbances recorded during normal sleep. 19 The authors reported that the accelerometer used in this report had a high intradevice reliability ranging from 96.5% to 99.1%. 19
The accelerometer data were analyzed using the Statistical Package for the Social Sciences (SPSS) version 20.0 (IBM, Armonk, New York, USA). The accelerometer data retained were screened for extreme values and are represented in Table 2. A total of 5 outlying data points of waking episodes (WEs) and activity at night (AAN) were deemed to represent extreme values (>2.5 standard deviation) influencing the data set. One of the extreme values was from the baseline phase, 2 were from intervention A, and 2 were from intervention B. No additional extreme accelerometer data were identified. Waking episodes and AAN were incrementally reduced throughout the intervention period. By the end of the circuit training phase, both surrogate markers of sleep quality had been reduced 64% for WE and 68% for AAN compared to the baseline values. The rate of change during the intervention for WEs and AAN is represented in Figure 1. A repeated-measure analysis of variance (ANOVA) was performed on the accelerometer data collected to evaluate the significance of the change in WEs per night and AAN during the different training phases. The training effect was deemed to potentially exert a confounded influence on the different phases in this conditioning program. Thus, a 2-tailed Dunnet t post hoc analysis was chosen to compare each respective training phase and baseline data to establish a threshold of significant changes in sleep quality during the intervention.
Accelerometer Data.
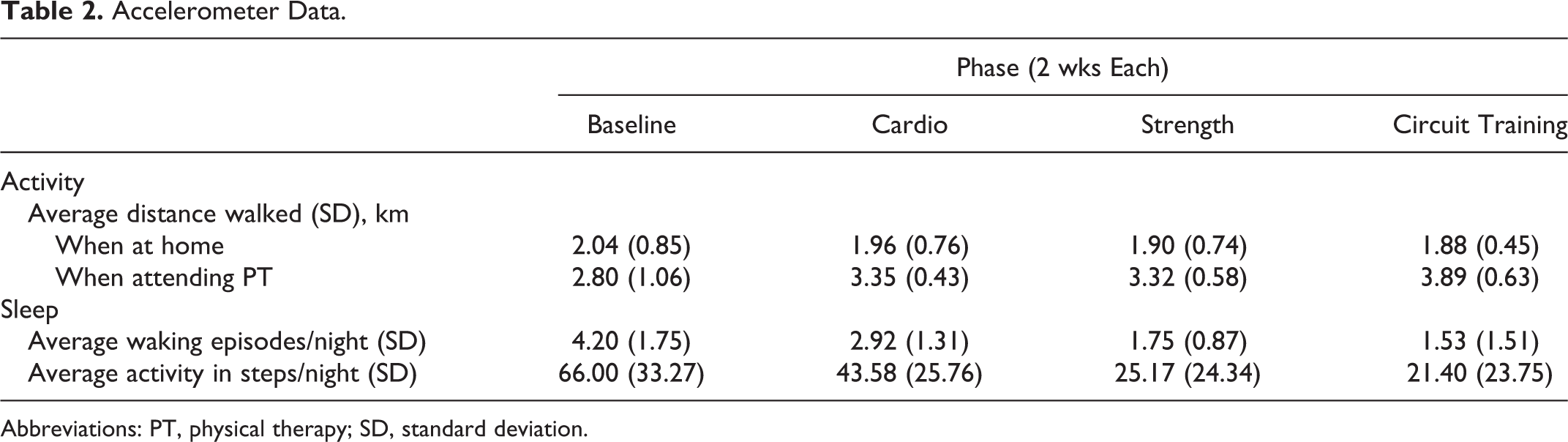
Abbreviations: PT, physical therapy; SD, standard deviation.

Accelerometer data.
The assumption of sphericity was confirmed in both WEs and AAN (P > .13). The repeated-measure ANOVA was significant for WEs (F 3,21 = 6.82, P = .002) and AAN (F 3,21 = 3.48, P = .034). The strength of the observed effect size (partial η2) attributed to the intervention was 0.49 for WEs and 0.33 for AAN. The post hoc analysis using Dunnet t found significant difference between the circuit training phase (P < .001) for both WEs and AAN. Also, during the strength training phase, the number of WEs (P < .001) and the amount of AAN (P = .001) were found to be significantly reduced when compared to the baseline data. The mean differences for each phase of the intervention and its comparison to baseline data are reported in Table 3. When including the extreme accelerometer values in the post hoc analysis, significant changes in activity were noted at the end of the 6-week program and baseline activity (P < .001).
Mean Differences for Accelerometer Data.

Abbreviation: CI, confidence interval.
aStandard error = 0.59.
bStandard error = 11.36.
c P < .001.
d P = .001.
Clinical Outcomes
Postintervention, the participant scored a 4/21 on the PSQI. At completion of the intervention, pain in his hips was reported at 6/10. On the 6MWT, the participant was unable to walk for the entirety of the 6 minutes. However, he increased his distance walked by 42 m and increased time walked by 43 seconds. In relation to the modified Bruce protocol, there was an improvement of 1 minute and 30 seconds, with a final HR of 96 bpm and a blood pressure of 140/80 mmHg. Postintervention, there was no significant changes in the ODI, TUG, and grip strength.
Discussion
This case report aimed to describe the effect of exercise on sleep and pain in a participant living with HIV/HCV coinfection. The clinical picture was further complicated by the convergence of multiple comorbid conditions, with all individually impacting sleep and pain. The participant also transitioned from being categorized as a poor sleeper to a good sleeper based on PSQI scores and accelerometer data. The positive impact on sleep quality concurs with similar reports in the literature. Ciccolo et al 20 reported improvements in sleep quality in PLWHA following an aerobic or resistance training program. Additionally, Lira et al 21 reported that moderate exercise training reduced the number of nighttime WEs and Rapid Eye Movement (REM) sleep latency in older adults.
In addition, the staged intervention resulted in improved activity tolerance as seen by increased distance walked per day, time completed on the modified Bruce protocol, and 6-minute walk distance. The participant traveled to the clinic using public transportation. On treatment days, his average distance walked was 36% to 106% greater than the days he did not come to the clinic (see Figure 2). Lastly, incorporating commercially available accelerometers in therapeutic interventions may assist clinicians in monitoring compliance and overall impact of clinical recommendations.

Average walking activity.
The reported MCID for the 6MWT is 54 m (95% confidence interval: 37-71 m) for a complete trial. 22 At the end of the intervention, the participant increased his 6-minute distance walked by 42 m and the total time walked by 43 seconds. It is likely that only moderate improvements occurred in his physical conditioning, as the participant’s ability to train at optimal cardiovascular workload might have been limited by eliciting neural fatigue with sustained activity.
People living with HIV/AIDS and living with cirrhosis of the liver as well as older adults have been reported to have decreased peak VO2 capacity and exercise tolerance. 5,8,23,24 Noting that the participant was 67 years old and living with HIV/HCV coinfection, we expected that the cardiovascular deficits would summate. As such, his low level of exercise tolerance was lower than that seen in individuals living solely with HCV or community-dwelling seronegative older adults. An exercise program focusing on cardiovascular fitness has been shown to be an effective conditioning intervention in PLWHA, correlating to the highlighted findings in this case report. 20
A 4/10 point decrease in pain was reported at the hips. The Minimal Clinically Important Difference (MCID) for the numeric pain rating scale is reported to be 2/10. 25 There was no significant change in the ODI score postintervention, whereas most objective measures of physical performance improved. We hypothesized that the participant’s decrease in pain and sleep disturbances may not have been large enough to impact the composite disability classification.
Of similar importance is the fact that the participant exhibited depressive affect throughout the intervention. We recommended individual counseling, however, he declined this recommendation.
In summary, the findings of this case report suggest that a comprehensive exercise program may improve sleep quality, pain, and cardiovascular fitness in individuals living with HIV/HCV coinfection. It is possible that people with systemic diseases that affect sleep quality and cardiovascular capacity could also benefit from comprehensive conditioning program. Cognitive–behavioral therapy to address chronic pain and sleep should be considered alongside a comprehensive conditioning program to maximize outcomes in pain management. The improvement in function, sleep quality, and pain reduction may be slow to become apparent, taking up to 6 weeks to manifest in this case. Lastly, incorporating common consumer-based accelerometers as biofeedback and compliance tools may further assist in reaching desired therapeutic goals in challenging populations.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.