
Abstract
HIV rates are disproportionately higher in the incarcerated compared to the general population. Unfortunately, HIV sero-positive inmates report perceived discrimination and missed antiretroviral doses. Correctional facility nursing competency in HIV management may mitigate these concerns. Using validated knowledge instruments, the authors measured baseline HIV knowledge in correctional facility nurses from 3 correctional facilities in Alberta, Canada, and quantified changes after a targeted educational workshop. Basic HIV knowledge increased significantly, whereas perceived need for further HIV education significantly decreased postintervention. This study demonstrates that correctional facility nurses may not receive ideal HIV education during employment and that targeted HIV workshops can significantly increase knowledge and confidence when caring for affected individuals.
The rates of HIV infection are disproportionately higher among incarcerated individuals compared to the general population. A review of HIV prevalence in prisons in low- and middle-income countries showed prevalence rates in excess of 10% in some countries. 1 In high-income countries, HIV prevalence in prisons varies widely from 0% in Denmark to 1.5% in the United States, and to 7.5% in Italy. 2 Corrections Service of Canada (CSC) notes that federal inmates (sentences of greater than 2 years) self-reported an HIV incidence of 4.6%, which is 15 times greater than the Canadian population. 3 Thus, the high volume of HIV-infected individuals passing through the criminal justice system provides an opportunity for promoting HIV testing, treatment, and retention into care for a high-risk and vulnerable population.
Unfortunately, gaps remain in effective delivery of HIV care within correctional settings, and stigma and discrimination have been identified as barriers to testing, self-disclosure, and access to antiretroviral treatment (ART). 4,5 Among Canadian federal inmates, 60% reported missing ART doses and 67% were worried about discrimination, thereby compromising HIV treatment efficacy and follow-up. 3 In the United States, only one-third of HIV-infected prisoners meeting criteria for ART in 2007 received treatment during incarceration, and lack of routine testing and reluctance to disclose HIV-positive status for fear of stigmatization have been sited as barriers. 5 –8 In contrast, correctional facilities with a highly structured treatment program, appropriate resources with the option of directly observed therapy, and knowledgeable health care providers have demonstrated significant viral load reductions and CD4 count increases in their incarcerated population contributing to a 40% increase in the number of viral suppressed inmates on release. 9
While it is possible to achieve optimal HIV outcomes within the correctional setting, many programs continue to describe limitations such as poor access to trained HIV physicians and lack of nursing staff to facilitate the provision of onsite HIV care. Correctional facility nurses, in particular, are an integral part of health care for inmates and are often the frontline providers for this high-risk and vulnerable population. Thus, an understanding of the patient population and a baseline competency in managing HIV are prudent among correctional facility nurses in order to reduce discrimination and improve care for HIV-infected inmates. Our pilot study attempts to measure the baseline HIV knowledge of correctional facility nurses and quantify any positive changes following a targeted educational workshop.
Methods
Study Population
This pilot study was performed with health care staff employed at 3 provincial (Alberta, Canada) correctional centers including a remand facility (inmates in custody prior to court appearances), a mixed remand and provincially sentenced facility (sentences of less than 2 years), and a young offender center (inmates aged 12-17 years old). The average number of inmates at these centers was 850, 530, and 87, respectively. The number of nurses was 25, 19, and 6, respectively. Participation was voluntary with informed consent. Ethics approval was granted by the University of Alberta Health Research Ethics Board.
Study Design
Baseline demographics of the participants were obtained by survey, including level of education, time spent in health care, and previous experience and education in HIV. Before and after our educational intervention, we used several validated HIV instruments previously described to assess perceived need for additional HIV education, objective knowledge about HIV, and attitudes toward persons living with HIV (Appendix A). 10 –13 Permission for use and/or modification was obtained from the original authors. The HIV knowledge scale was adapted from Balfour et al and measured HIV treatment knowledge surrounding adherence, side effects, and drug resistance. 10 This instrument was tested in HIV patients, community health care providers, and college students with adequate 2-week test–retest reliability (rs = .83) and internal consistency (r = .90). 10 HIV transmission knowledge was assessed using Carey et al’s true/false “HIV-KQ-18” testing instrument, which demonstrated high internal consistency (α = .75-.89), test–retest stability (rs = .76), and a strong association with longer, previously validated measures (rs = .93-.97). 11 Froman et al’s “Measure of attitudes towards persons with AIDS” was used to explore feelings on the following 4 themes: homophobia, blaming the victim, fear of AIDS, and unrealistic concerns about AIDS and empathy. 12 Grading was based on a 6-point Likert-type scale, and the instrument had been tested on nursing students with good internal consistency (α = .78-.85). 13
Our pilot intervention consisted of an educational workshop developed by the current study authors and provided by an infectious diseases physician, HIV nurse, and HIV pharmacist (Appendix B). This 45-minute PowerPoint presentation reviewed national, local, and correctional facility HIV epidemiology; HIV pathogenesis and modes of transmission; treatment overview and prognosis; and HIV issues unique to correctional populations.
Statistical Analysis
Data were analyzed using SPSS version 19.0.0.1. Descriptive statistics such as frequencies (%) were calculated for categorical variables. Means and their standard deviation were calculated for continuous variables. Normality of the data was checked both by histogram and by Kolmogorov-Smirnov test. Differences between pre–post workshop scores for perceived need for education, knowledge, and attitude were normally distributed and analyzed by paired t test. In order to compensate for the repeated type 1 error of multiple paired t tests, Bonferroni adjustment was used by multiplying the P value of each comparison with the total number of paired t tests applied. The significance level for P value was set at .05. The pre–post scores and their differences are reported as mean ± standard deviation.
Results
Baseline Demographics
Of the 35 participants in the pilot study, 22 were licensed nurses and the remaining 13 participants were from psychology (n = 8), pharmacy (n = 2), or administration (n = 3). Of the 22 nurses, 8 (36.4%) had registered nurse (RN) diplomas, 9 (41%) had a bachelor’s degree in nursing (BN), and 2 (9%) were registered psychiatric nurses (RPNs). In Canada, registered nurses have completed a registration examination and obtained either a diploma or a baccalaureate degree in nursing. Registered psychiatric nurses have completed a registration examination and diploma in psychiatric nursing. Fifty percent were employed full-time and 20 (91%) were from either the remand facility or the mixed remand/sentenced facility. Seven (32%) had prior experience in acute care, 3 (13.6%) had prior experience in correctional facility care, and 7 (32%) some combination thereof (Table 1).
Sociodemographic Characteristics of Health Care Staff in Correctional Facilities in Alberta, Canada.

HIV
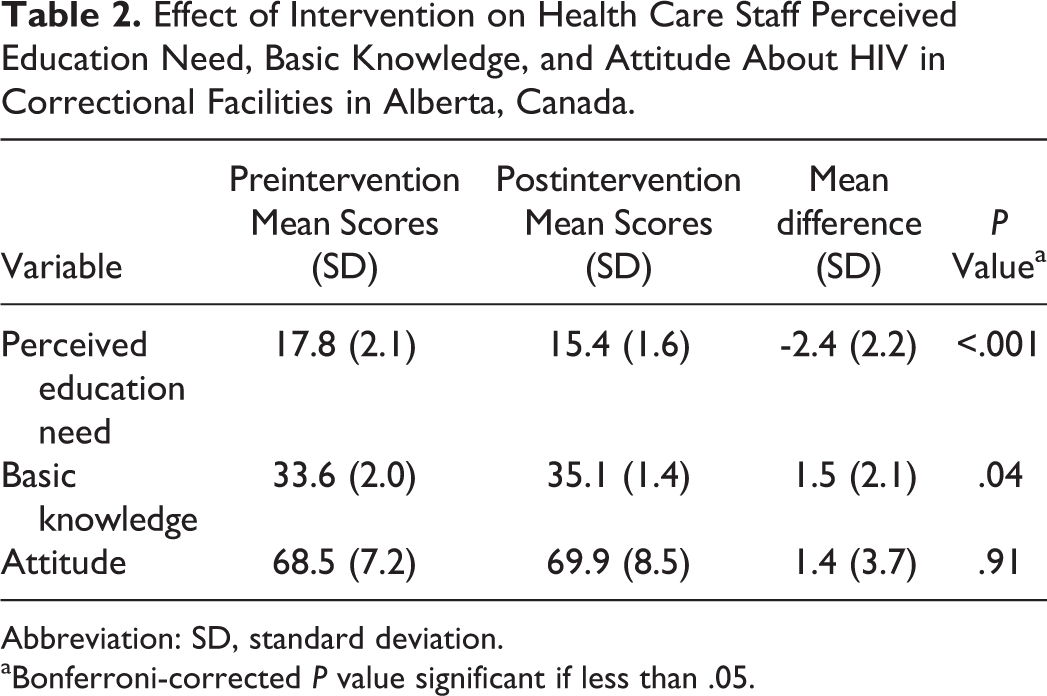
During their employment in correctional facilities, 5 (22.7%) nurses received formal HIV education, 14 (63.6%) sought independent learning, and 18 (81.8%) had prior experience in caring for individuals living with HIV, usually with over 20 patient encounters. At baseline, the perceived need for further HIV education scored at 17.8 ± 2.1 and decreased by 2.4 ± 2.2 (P < .001) postintervention. Nursing attitude toward people living with HIV (ie, degree of empathy and desire to optimize care) at baseline scored at 68.5 ± 7.2 and did not change significantly postintervention (P = .91). Conversely, the basic HIV knowledge score significantly increased by 1.5 ± 2.1 (P = .04) from a baseline of 33.6 ± 2.0. The major deficiencies in baseline HIV knowledge included principles in optimizing medication administration to reduce resistance development and inconsistent awareness of methods to prevent perinatal transmission in pregnant HIV women (Table 2).
Effect of Intervention on Health Care Staff Perceived Education Need, Basic Knowledge, and Attitude About HIV in Correctional Facilities in Alberta, Canada.
Abbreviation: SD, standard deviation.
aBonferroni-corrected P value significant if less than .05.
Discussion
Among the 22 correctional facility nurses in our pilot study, less than a quarter had received formal HIV education, despite this patient population being overrepresented. Rather, nurses often relied on previous patient encounters or independent learning to supplement their knowledge. Correctional facility nurses have likened themselves to an isolated specialty and previously voiced concerns regarding balancing autonomy in the face of limited on-site physician availability. 14 Providing regular education on this commonly encountered infection can provide them with the skills necessary to provide optimal health care as well as alleviate anxiety and misconceptions about caring for inmates with HIV. This is particularly important, as correctional facility nurses, by survey, are less likely to refer their clients to other resources and more likely to act as primary health care providers. 14
Our study demonstrated that correctional facility nurses benefited from the educational workshop as indicated by a significant increase in overall HIV knowledge and decreased need for further HIV education postintervention. Of note, positive attitude toward individuals living with HIV did not increase postintervention. A variety of explanations are possible. Firstly, attitudes are more intrinsically fixed compared to knowledge and may not be as amenable to change following a short 45-minute workshop. Alternatively, given their line of work and interest in this patient population, correctional facility nurses may already be empathetic to persons living with HIV with minimal room for improvement. This is the more likely explanation, given the already high preintervention attitude score (68.5 ± 7.2).
There is an ongoing need for the development of innovative approaches for addressing improvement in HIV care delivery services within incarcerated populations. Our pilot study employed a simply constructed “educational outreach visit (EOV)” as one potential strategy for improving HIV care delivery within the correctional environment. Educational outreach visits are defined as “a personal visit by a trained person to health professionals in their own settings.” 15(p2) A systematic review of 69 randomized studies of EOVs with objective outcome measures demonstrated this type of intervention alone or in combination with other interventions can be effective in improving desired health professional practices. 15 Another successful approach is the use of “local change teams (LCTs)” that operate on the following 5 principles: (1) understand and involve the customer; (2) fix key, important problems; (3) pick a powerful change leader; (4) get ideas from outside the organization; and (5) use rapid cycle testing. 16 A modified version of LCTs was evaluated in the HIV Services and Treatment Implementation in Corrections Study, which compared LCTs to HIV training alone in 9 correctional facilities in the United States. 17,18 Local change teams doubled the odds of successful delivery of HIV services (point estimate for odds ratio = 2.14) and increased health care staff perceptions of the value of HIV services compared to the control group. 19,20
From a public health viewpoint, the disproportionate burden of HIV in incarcerated populations presents both a challenge and an opportunity. Correctional facilities provide an opportunity to engage a traditionally “hard to reach” demographic that often slips through the conventional community-based health system. For these individuals, prison presents an opportunity for diagnosis, disease management, education, counseling, and treatment that may not be as readily available in the general community. Within the enclosed population of a correctional facility exists a missed opportunity to optimize care—care that will improve the health of the inmate and concurrently decrease transmission to the general public upon release from prison. If correctional facility nurses can be armed with a good foundation for the diagnosis and management of HIV, they can serve as a valuable resource and extend the principles of public health to our correctional system—a feat that would better both the inmates and the general public. Our study demonstrates that simply designed workshops can improve knowledge in correctional nurses caring for inmates with HIV.
Although our pilot study is one of the first to demonstrate a need for increased HIV education among correctional facility nurses, and the value of dedicated educational workshops, there are several limitations. The sample size was small and lacked a comparison group, making it difficult to generalize our findings. Secondly, attitudes and perceived need for further education was assessed using nursing self-report from a group of voluntary participants, raising the possibility of bias and preference toward providing socially desirable answers. Thirdly, although we attempted to use validated instruments to measure HIV knowledge, any underlying limitations to the knowledge instruments would also impact our study results. Lastly, although we demonstrated an increase in knowledge postintervention, we do not have tangible evidence that our intervention leads to real-life improvement in patient care. Areas of future study to examine these outcomes include the measurement of number of missed antiretroviral doses and patient-perceived HIV quality of care.
Patients with HIV are overrepresented in correctional facilities. Our pilot study demonstrates that correctional facility nurses may not always receive essential training during employment, which can contribute to suboptimal patient care. Directed HIV educational sessions can significantly increase their knowledge, ultimately leading to improved HIV care in incarcerated populations.
Footnotes
Appendix A
Appendix B
Acknowledgments
The authors wish to acknowledge the significant contributions of Chantal Ho and Tammy George. The authors also acknowledge the health care and security staff of the participating correctional facilities for their support of the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.