
Abstract
Background:
Poor treatment adherence is a main barrier for effective antiretroviral therapy (ART) globally. HIV-related knowledge may affect understanding and utilization of HIV medical information, hence limited health literacy is a known barrier to treatment adherence.
Design and Methods:
A cross-sectional study included 494 HIV-infected individuals from the Bissau HIV Cohort in Guinea-Bissau. They completed a questionnaire designed for assessment of adherence and HIV-related knowledge.
Results:
A majority were female, 41% were illiterate, 25% did not take the medicine during the last 4 days, and 23% skipped their medicine during weekends. The most frequent reasons for not taking medicine were simply forgetting, side effects, lack of food, and being too ill to attend the clinic. Nonadherent patients had a lower level of HIV-related knowledge.
Conclusion:
Main barriers for nonadherence were side effects, food insecurity, and simply forgetting. Lack of HIV-related knowledge about ART and HIV may be a barrier to nonadherence.
Introduction
To be infected with HIV is considered a chronic condition involving lifelong treatment that allows a higher quality of life for many people infected with HIV. Low adherence to treatment is one of the most important barriers to the effectiveness of antiretroviral therapy (ART) in Africa. 1,2 Early studies in Africa on adherence have shown promising results, with adherence levels equivalent to, and in some cases exceeding, those seen in Europe and United States. However, suboptimal levels of adherence have been reported in several settings. 3 In resource-limited settings, several factors compromise adherence, and this could be intermittent drug supply, fear of stigmatization, long distance to available treatment, lack of transport to dispensing clinics, hunger, side effects, and lack of access to correct information. 4 –6 A meta-analysis of ART adherence showed that, on average, 23% of patients from sub-Saharan Africa did not adhere to ART, and the proportion of nonadherent patients ranged from 2% to 70% across the studies included in the analysis. 4 Retaining patients on ART is thus a challenge. A review of loss to follow-up in sub-Saharan Africa found that the amount of patients adhering to ART decreased over a period of 2 years, with estimated average retention rates at 6, 12, and 24 months of 79%, 75%, and 62%, respectively. 7 Nonadherence cause patients to drop out of ART, resulting in drug resistance and increased mortality. 4,7
Lifelong treatment is still a new concept in Africa, where health care systems already face many different challenges due to out-of-date equipment, insufficient number of health care providers (HCP), and in some cases low moral. 8,9 There are few studies evaluating interventions to improve adherence to ART in Africa, but more innovative interventions are needed to achieve optimal adherence to ART. 10,11
In Bissau, 9% of the population is infected with HIV. 12 Treatment has been available since 2005 and is free of charge for all patients. 13,14 In 2009, we completed the first study on HIV and adherence in the country on barriers and facilitators to adherence. This study showed that HIV-related knowledge was a determining factor for optimal adherence. 15 HIV-related knowledge may affect patient use, understanding, and utilization of health care information on HIV, hence limited health literacy is a known barrier to treatment adherence. 16 The aim of this cross-sectional study was to validate the findings of our previous study on barriers and facilitators to adherence and describe the association with HIV-related knowledge in Bissau, Guinea-Bissau.
Methods
Study Design and Participants
In a cross-sectional design, we determined barriers and facilitators for good adherence to HIV treatment. In July 2007, we established the Bissau HIV Cohort by creating a clinical database and a biorepository bank containing blood samples from the HIV clinic at Hospital Nacional Simão Mendes. 14,17 HIV-infected individuals from Bissau are referred from primary health care centers and from the blood bank to this HIV clinic, which has become the major HIV center in the country and a training center for staff. The Bissau HIV Cohort consists of approximately 4080 HIV-infected individuals but has a high rate of loss to follow-up and mortality. 8,13,14,17 We included HIV-infected individuals aged 18 years or older diagnosed with HIV and who had received ART for at least 3 months. Patients were invited to participate at their regular control visit and collection of medicine.
The national ethics committee in Guinea-Bissau approved the study. Before inclusion, the participants gave consent to participate. A local, trained nurse informed participants about the study orally in the widely spoken language Portuguese creole. Participants were informed that all data would remain confidential and that participation or declining to participate would not affect their access to treatment. All participants were interviewed by the same nurse, and all questions were asked orally as most patients were illiterate. At inclusion into the Bissau HIV Cohort, participants signed a consent form. The Bissau HIV cohort has been approved by the National Ethics Committee in Guinea-Bissau. The Cohort Study Group has an open approval to use data from patients’ medical records as long as patient confidentiality is maintained.
Development of Questionnaire
The questionnaire consisted of validated and pilot-tested scales and had been forward and backward translated from original US English to Portuguese and Portuguese creole. The questionnaire was designed for assessment of adherence to treatment and description of barriers and facilitators to adherence, based on our previous findings from the qualitative study in 2009. 15 The final questions were validated in a pilot study with 12 HIV-infected individuals, in February 2012. We carefully reviewed the questions with the local nurse before the start of the study and offered supervision during the data collection to address potential sources of bias.
Measurements
Demographic characteristics
The following variables were recorded: patient identification, sex, age, address, marital status, religion, and nationality.
Other variables
The other variables assessed include attended the clinic as scheduled, number of days being late for scheduled appointments, reasons for not attending scheduled appointments, mode of transportation to the clinic, the time and expenses related to visiting the clinic, educational level, speaking Portuguese, literacy, profession, current job, salary received last month, disclosure of HIV status, satisfaction with life, and self-reported health status.
Adherence
Good adherence was defined as reporting having missed no doses of ART during the previous 4 days (taking ≥95% of the medicine).
Adult AIDS Clinical Trial Group Adherence Questionnaire
Self-reported adherence was assessed with the Adult AIDS Clinical Trial Group (ACTG) adherence questionnaires. 18 Identifying the last time patients skipped any medication (eg, within the past 4 days, within the past 30 days, and during weekends) and reasons for not taking the medication (eg, away from home, busy with other things, simply forgot, and side effects).
The Self-Rating Scale Item
Single item self-reported adherence scale that uses adjectives in a 5-point Likert-type scale “very poor, poor, fair, good, very good and excellent” to describe medication adherence for the last 4 weeks. Results were translated into percentages. 19
HIV-related knowledge
HIV-related knowledge was assessed as functional, related knowledge/functional literacy (eg, the ability to read, understand, and act on health information) and the questions were divided into 3 subgroups: (1) illness-related knowledge, (2) understanding HIV-related knowledge, and (3) treatment perceptions. Illness-related knowledge (10 questions): Knowledge of ways of transmission (eg, by a contaminated knife or needle, mosquito bites, and so on). Understanding HIV-related knowledge (9 questions): Understanding of HIV, how to translate HIV knowledge into practice (eg, can a person of good health be carrier of HIV? Do you think a person infected with HIV can get rid of the virus for good?). Treatment perceptions (10 questions): Perceptions of HIV treatment (eg, Treatment is available to reduce side effects? Can you ever stop taking your medicine?). The answers in all 3 subgroups were divided into 2 groups among adherent/nonadherent patients. Group 1: 1-5 correct answers and group 2: 6-9/10 correct answers. We used the questions from the validated HIV-related knowledge scale
19
and added questions emerging from the qualitative study conducted at the clinic in 2009.
15
Statistical Analysis
Statistical analyses were conducted using STATA 10 (StataCorp LP, College Station, Texas, USA). The primary end point was prevalence of nonadherence. We used unadjusted and adjusted (multiple) logistic regression models to determine the association between the dependent variable (adherence) and the independent variables such as demographics and HIV-related knowledge. Statistical significance was defined as P < .05.
Results
Between October 2012 and May 2013, 494 (22%) of the 2289 HIV-infected individuals receiving ART at the clinic were enrolled in the study, and 82% of the participants lived in the capital Bissau. The 494 included in this study were comparable to the remaining HIV-infected individuals in the Bissau HIV Cohort receiving ART with regard to sex, age, HIV-type, employment, educational background, literacy, and marital status. 13 Data on demographics and prevalence of nonadherence are presented in Table 1. The majority were female, and nearly half were illiterate. The majority of nonadherent participants were between 26 and 44 years, females, unemployed, without salary last month, no schooling, and unable to read.
Demographic Information and Nonadherence among 494 HIV-Infected Individuals.
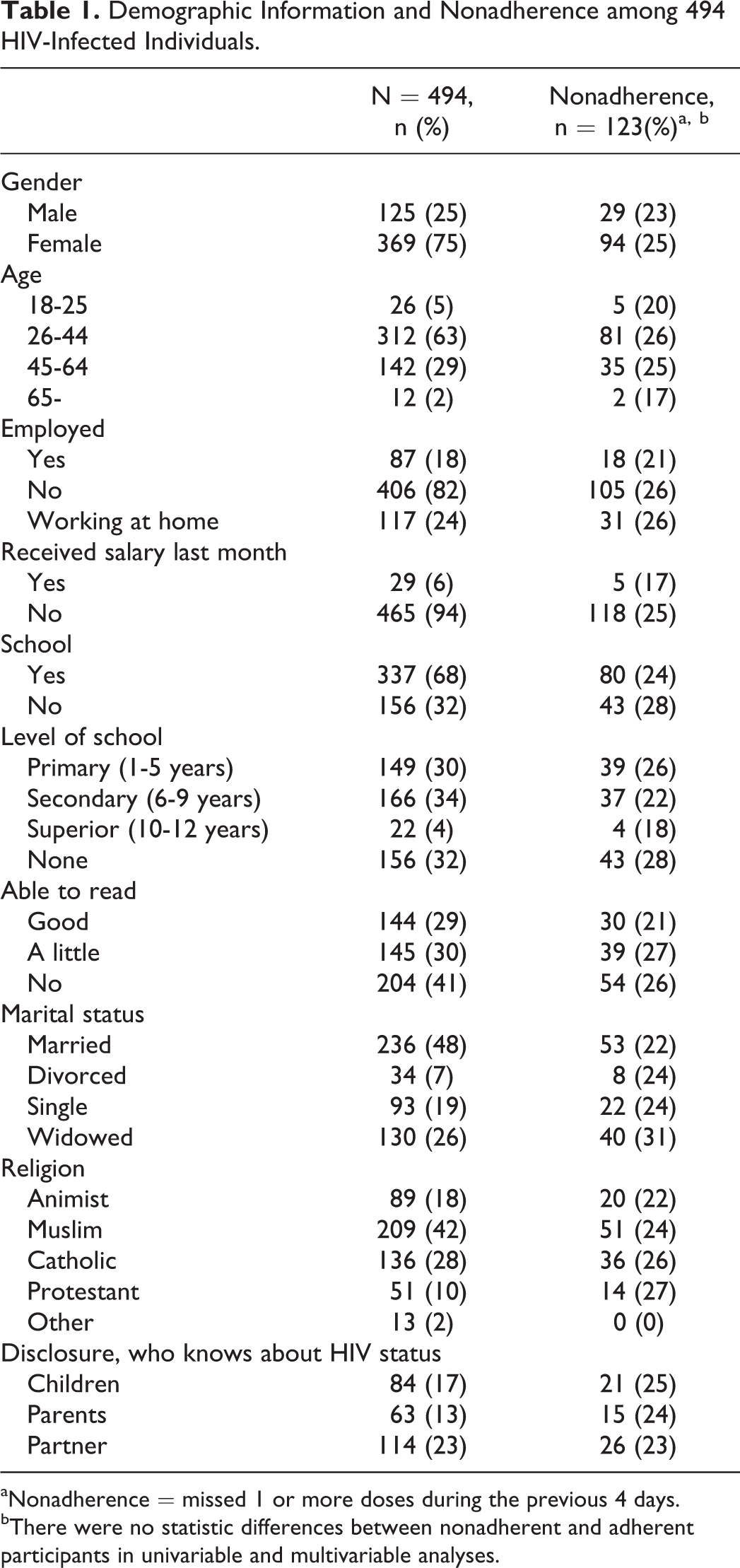
aNonadherence = missed 1 or more doses during the previous 4 days.
bThere were no statistic differences between nonadherent and adherent participants in univariable and multivariable analyses.
Univariate analysis comparing adherent with nonadherent participants did not show any significant differences regarding demographic characteristics. Nearly half of the married participants disclosed their HIV status to their spouse. More than half (218, 56%) of the participants did not attend the clinic as scheduled, and the most frequent reasons for attending late were temporary travel, forgetting the date of appointment, and lack of money. Most of the participants had less than 1 hour of transportation time to the clinic. Participants who did not attend the clinic as scheduled were at higher risk of nonadherence (odds ratio [OR]: 8.7, 95% confidence interval [CI]: 5.2-14.2; P = .01).
The data on self-reported adherence (Self-Rating Scale Item) revealed that during the last 4 weeks, 15% reported taking 40% of the medication, 30% reported taking 60% of the medication, and 3% reported taking 90% (Table 2). Results from the ACTG scale showed that there were 25% who did not take the medicine during the last 4 days, and 28% skipped their medicine during weekends. The most frequent reasons for not taking medicine were simply forgetting (23%), having side effects (15%), lack of food (8%) and being too ill to attend the clinic (4%). The most frequently reported side effects were dizziness, nausea, fatigue, and headache, and 66% did not know that treatment was available for side effects.
Adherence among 494 HIV-Infected Individuals.

None of the participants answered all questions about HIV-related knowledge correctly. Overall, there was an association between the number of correct answers in HIV-related knowledge and HIV-infected individuals who were adherent. Those who answered 6 to 9 questions correctly had a higher adherence compared with those who only answered 1 to 5 questions correctly (Figures 1 –3).

Illness-related knowledge score and adherence among 494 HIV-infected individuals.

Understanding HIV-related knowledge score and adherence among 494 HIV-infected individuals.

Treatment perceptions score and adherence among 494 HIV-infected individuals.
In univariate analysis, the treatment perceptions and illness-related knowledge score showed significant differences between the adherent and the nonadherent group when answering these questions wrongly: By mosquito bites? (OR: 1.8, CI: 1.4-3.0; P > .01); HIV is contracted because of traditional causes (OR: 1.7, CI: 1.1-2.6; P > .03); can you be cured of HIV by traditional medicine? (OR: 1.8, CI: 1.1-3.0; P > .02); is it a good idea to take a break from ART? (OR: 2.3, CI: 1.2-4.6; P > .04); HIV medication can be taking at different times of the day at weekends and holidays? (OR: 2.3, CI: 1.0-5.2; P > .04). There were no significant differences in the group of understanding HIV-related knowledge.
In multivariate analysis, the treatment perception score and the illness-related knowledge score of the questions are as follows: by mosquito bite (OR: 2.1, CI: 1.3-3.6; P > .01); HIV is contracted because of traditional causes (OR: 1.9, CI: 1.1-3.0; P > .01); you can be cured of HIV by traditional medicine (OR: 1.7, CI: 1.0-2.9; P > .04); and there is no treatment for side effects (OR: 0.6, CI: 0.4-1.0; P > .04) were independently associated with the group of the nonadherent patients.
Discussion
In this cross-sectional study, we showed that 25% of the HIV-infected individuals had not taken their medicine during the last 4 days, 23% skipped their medicine during weekends, and only 16% had remembered to take 80% or more of their medicine during the last month. An adherence level to treatment of ≥95% is required for effective suppression of HIV and to prevent the development of drug resistance. 20,21 This indicates that 84% of the HIV-infected individuals in this study are at risk of developing drug resistance and virological failure.
The most frequent reasons for not taking medicine were simply forgetting, running out of pills, traveling, side effects, lack of food, and feeling too ill to attend the clinic. Simply forgetting, running out of pills, and traveling are similar to reasons given for nonadherence among HIV-infected individuals in both high- or low-income countries. 22,23 Side effects, lack of food, and feeling too ill are specific barriers to adherence in Africa and have also been described in other African studies. 24 Our study showed that 30% of the HIV-infected individuals experienced side effects and that 66% did not know that treatment was available to avoid some of these. A review of determinants for adherence to ART among HIV-infected individuals in Africa found that side effects often resulted in irregular medication intake. 25
We found that many were illiterate which is also reported in other African settings. 26 When comparing the adherent with the nonadherent participants, none of the demographic variables differed significantly between groups. This may indicate that being illiterate is not a predictor of nonadherence, and this has also been found in other studies. 27,28 A study by Peltzer et al 27 in KwaZulu-Natal found greater adherence among those with lower levels of education. 27 Another study 28 reported that those with good discussions with the HCP about adherence were more adherent and had a better understanding of consequences of suboptimal adherence irrespective of literacy status. 28 We suggest that being illiterate may not be a barrier to nonadherence, and the information to the HIV-infected individuals given by the HCP at the clinic is more important to adherence. Another reason for nonadherence could be related to disclosure of HIV status. In our study, only 48% disclosed their HIV status to their spouse and few disclosed it to family or friends. We have previously described that patients reported being afraid of disclosing their HIV status because they feared stigmatization and rejection from family and friends. 15 Different studies have reported that HIV-infected individuals are more adherent to ART when supported by family. 24,27,29 Expecting and fearing rejection because of stigma is associated with more need for constricted social networks. 30 By discussing disclosure with the HCP, a study from South Africa 31 showed that HIV-infected individuals improved adherence. We suggest that HCPs should be part of interventions designed to assist HIV-infected individuals in reducing disclosure-related stress, making effective disclosure decisions, and obtaining communication skills for effective disclosure to increase adherence.
HIV-related knowledge and health literacy influence adherence. 32 –35 A study from the United States found that patients with low literacy were 3.3 times more likely to be nonadherent to ART. 35 We investigated the degree of functional health literacy 36 in 3 subgroups of HIV-related knowledge questions, illness-related knowledge, understanding of HIV-related knowledge, and treatment perceptions. We found that lack of HIV-related knowledge about ART/HIV was a barrier to adherence, as none of the HIV-infected patients in our study answered all questions in a way perceived as correct by the authors.
In the group of questions on illness-related knowledge and treatment perceptions, participants who were adherent answered most questions correctly. In the understanding of HIV-related knowledge group, there was no difference among adherent and nonadherent participants, which perhaps indicates that the HIV-infected individuals may have difficulties transforming their HIV knowledge into practice. Our findings suggest that HIV-infected individuals with better HIV knowledge may increase their adherence to ART. This has also been found in other studies. Adherence rates to ART among participants who reported having good discussions with their HCPs about adherence issues were also higher. 28 A study from South Africa 32 showed that HIV-infected individuals with marginal literacy skills benefitted from adherence counseling regardless of pictographic tailoring, and patients with lower literacy skills required more intensive or provider-directed interventions. 32 Many recent studies have shown that ART adherence improves after increasing HIV knowledge and that greater health literacy or HIV-related knowledge is associated with better health outcomes. 37 Moreover, screening tools could be used to identify those in need of interventions. 38 In the HIV clinic in Bissau, there is no structured intervention to prepare HIV-infected individuals to start ART. Our study provides new knowledge on the importance of health literacy which should be taken into consideration when HIV-infected individuals start treatment.
We suggest that this knowledge could be used to develop specific interventions in clinical practice to provide newly diagnosed HIV-infected individuals better and consistent information about HIV, ART/side effects, and the importance of adherence.
A possible way to overcome low HIV-related knowledge and increase adherence could be to establish group interventions at the clinic. In a randomized study from Nigeria on HIV-infected women on ART, 39 the effect of group sessions compared to the control group was tested, and 6-month follow-up reports showed significantly higher levels of adherence to ART, higher knowledge of HIV, and significantly more women from group sessions returned for follow-up.
There are several limitations to this study. Of the 2289 HIV-infected individuals on ART, 494 (22%) were interviewed, and we do not have adherence and HIV-related knowledge information of those not included. Many HIV-infected individuals are lost to follow-up 8 and are not represented in this survey, thus constituting a source of bias. Those who do not attend the clinic may lack HIV-related knowledge because they are less exposed to information from HCPs. Most likely, this has underestimated our findings.
The data were obtained by interview with 1 trained interviewer. There may be recall bias or linguistic interpretations, despite using a trained interviewer, pilot testing, and supervised the interviewer continuously. The design of our study was cross-sectional, thus we cannot establish cause–effect relationships but merely show association.
This is the first quantitative study about ART adherence and HIV-related knowledge/health literacy in Guinea-Bissau. The findings from our previous qualitative study were confirmed in this quantitative study. Lack of HIV-related knowledge about ART/HIV was a barrier for optimal adherence in this cohort. Our findings indicate that greater efforts are needed to educate HIV-infected individuals sufficiently about HIV, ART, and lifelong treatment.
We suggest that HIV-infected individuals with poor HIV-related knowledge may benefit from medication adherence programs and culturally targeted interventions to increase health literacy and to improve adherence. Future research should focus on developing, investigating, and evaluating interventions on adherence and HIV-related knowledge in HIV-infected individuals.
Footnotes
Acknowledgments
The authors are grateful to the participants and the staff at the HIV clinic at Simao Mendes Hospital in Bissau, specially the local nurse Cedina Umaru Cande, who performed all interviews, without whom, this study would not have been possible. The Bissau HIV Cohort study group consists of Amabelia Rodrigues, David da Silva, Zacarias Da Silva, Candida Medina, Ines Oliviera, Lars Østergaard, Alex Lund Laursen, Morten Sodemann, Peter Aaby, Anders Fomsgaard, Christian Erikstrup, Jesper Eugen Olsen & Christian Wejse (chair).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Aarhus University Research Foundation and Bodil Pedersen Foundation, Denmark. The HIV clinic is supported financially by its collaboration with International Epidemiologic Databases to Evaluate AIDS (IeDEA) and West African Platform for HIV Intervention Research (WAPHIR). The authors acknowledge the National Cancer Institute (NCI), the Eunice Kennedy Shriver National Institute of Child Health & Human Development (NICHD) and the National Institute of Allergy and Infectious Diseases (NIAID) of the U.S. National Institutes of Health (NIH), as part of the International Epidemiologic Databases to Evaluate AIDS (IeDEA) under Award Number U01AI069919.