
Abstract
In Argentina, providers’ response to motivational interviewing (MI) to improve engagement and retention in care among challenging patients with HIV was evaluated. Twelve HIV care physicians participated, and their video recordings pre- and post-MI training were also obtained. One week post-training, 11 of the 12 participants were committed to using MI strategies during consult session. Of the 12 participants, 9 demonstrated appropriate utilization of MI techniques and change in HIV education provided during consultation (Z = −2.375, P = .018). Motivational interviewing appears to be a viable strategy to enhance engagement and retention in challenging HIV-positive patients.
Introduction
Since the development of combination antiretroviral therapy (cART) to inhibit viral replication, 1 individuals living with HIV infection have the opportunity to control their illness and live longer, healthier, and productive lives. However, in order to obtain the maximum benefit of cART and to prevent the development of drug-resistant viral strains, medication adherence needs to be strictly maintained. 2 Unfortunately, not all HIV-infected patients achieve the high levels of adherence necessary to maintain treatment success. Adherence to medication is a complex issue that involves multiple factors such as patient-related factors (health beliefs, depression, substance abuse, literacy, stigma, and nondisclosure of HIV status), 3 and provider-related factors (communication skills and length of appointments). 4,5 Structural, economic, and environmental determinants are also important, such as health care facility accessibility, clinic hours, transportation, income, and employment. 6,7
To overcome barriers to engagement, adherence, and retention in care, interventions have been developed to increase patients’ motivation to engage in health behavior. Motivational interviewing (MI) 8 is an example of an effective counseling strategy designed to promote health behavior and achieve optimal health outcomes that has been utilized with individuals with HIV to reduce risk behavior and substance abuse and to enhance medication adherence 3,9 –11
Motivational interviewing is a collaborative, patient-centered form of guiding to elicit and strengthen motivation for change, as behavior change is not the sole responsibility of the patient but a shared endeavor. Motivational interviewing involves a patient-centered approach to consultation whereby the patient presents reasons for change while the facilitator provides support. Motivational interviewing techniques are used to identify ambivalence within the individual to facilitate behavior change from the patient’s perspective, 12 eliciting barriers to adherence and assisting in overcoming those barriers. Studies suggest that health care providers using this method of interaction can often encourage patients with chronic conditions to follow their medication regimen, to reduce unhealthy habits, and to take constructive action on their own behalf. 13,14
The demand for professional training in MI has grown in recent years, 11 and most MI training for health care practitioners has been provided in the form of workshops. Such workshops typically include an introduction of the philosophy and principles of MI followed by demonstration of the method and guided practice in learning the skills. Although the length of training for health care providers is variable, but the mean time has been 9 hours. 15 The training elements typically include the basic MI skills, MI spirit, recognizing and reinforcing change talk, and rolling with resistance. Physicians utilizing MI engage with patients in an empathic, nonjudgmental manner and pose simple but strategic questions to motivate change; when patients resist change, the physician “rolls” with it, instead of fighting against it. If and when the patient is ready to initiate a change, the physician supports their decision.
The HIV/AIDS national program in Argentina provides universal access to ART for the estimated 110 000 HIV-positive patients (HIV prevalence 0.4% among adults). Despite this universal access program, around 30% of those on ART do not achieve an undetectable viral load (VL) and 25% have poor appointment attendance and inadequate engagement and retention in health care services. 16 Although MI has been used among Spanish-speaking populations for chronic conditions as a client-centered strategy, 17,18 MI has not previously been utilized in Argentina among physicians providing HIV health care to nonadherent and disengaged patients. This study examined the impact of MI training on uptake and utilization of MI strategies and “adherence-targeted” strategies during routine consultations by private and public HIV health care physicians in Buenos Aires, Argentina. In addition, we examined providers’ perceptions of the feasibility and acceptability of using MI to improve patient engagement and retention in care. We theorized that MI would be an acceptable and feasible strategy for Argentine health care providers in clinical settings in both public and private health care.
Methods
This article presents data that were derived from a larger study conducted in Buenos Aires, Conexiones y Opciones Positivas en la Argentina (COPA). Data presented were collected from April 2013 to December 2013. Prior to study onset, institutional review board and ethics committee approval were obtained from the US site and the 2 Buenos Aires sites. HIV health care physicians from both sites were invited to participate in the study, and 12 (n = 6 each site) were enrolled. Following provision of informed consent, physicians provided a video recording of a routine medical consultation with a patient who had provided consent for video recording.
Assessments
Videotapes
A baseline video recording during a routine medical consultation with an HIV-positive nonadherent patient was obtained from every physician participating in the study. All videos were reviewed and coded by the US team for the use of MI techniques, targeting adherence and engagement in care. In addition, videos were scored using the Standard Of Care (SOC) quality checklist. The video recordings provided the foundation for the development of the workshop on MI techniques and enabled the team to tailor to the workshop to the needs of the local physicians.
Follow-up videos were made by participants 1 to 2 months following the workshop training. Participants videotaped a new session with a different HIV-positive nonadherent patient. Videos were coded for MI techniques and scored against the SOC quality checklist.
Standard of Care Quality Checklist
An SOC quality checklist 19 was administered to 12 physicians “pre- and post-MI” video recordings (see Table 1). The SOC quality checklist contains 34 items (“Yes, No, and Don’t Know”) designed to assess the existing SOC delivered at the site. Clinicians in the clinical setting typically utilize techniques to increase knowledge about disease and treatment options, persuasive communication about treatment adherence, and collaborative problem solving to deal with anticipated problems. Thirty-four items were coded from the videos and scored to indicate whether the standard care item was applied during the video. The resulting 6 subscales, education systematically provided (eg, HIV, treatment, and side effects information, range = 0-9), method of provision of information (eg, charts and verbal, range = 0-3), systematic planning of medication intake (tailoring and daily dosing, range = 0-12), standard support in consecutive visits (adherence problem solving and feedback on laboratory results, range = 0-6), general support services (telephone support, deliveries, and referrals, range = 0-5), and other types of standard care (eg, adherence monitoring, feedback, and self-monitoring, range = 0-1).
Standard of Care Quality Checklist.

Acceptability and Feasibility
Feasibility and acceptability of MI questionnaire of 9 items (see Table 2, English translation) were completed immediately after finishing the workshop sessions. The postworkshop questionnaire was designed to collect information about the acceptability of the MI workshop, MI principles, and willingness to include MI with nonadherent or difficult patients. Participants were asked to score the questionnaire statement using a Likert scale of 1 to 7, ranging from 1 (strongly disagree) to 7 (strongly agree). A similar second questionnaire of 6 items was completed 1 to 2 weeks postworkshop to evaluate the acceptability and feasibility of using MI techniques with their difficult patients (see Table 3, English translation).
Providers’ Acceptability and Feasibility Questionnaire I After Workshop.a

Abbreviation: MI, motivational interviewing.
an = 12.
bScoring on a 6-point Likert scale from 1 = strongly disagree to 6 = strongly agree.
Providers’ Feasibility and Acceptability Questionnaire Two Week Postworkshop.a

Abbreviation: MI, motivational interviewing.
an = 11.
bScoring on a 6-point Likert scale from 1 = strongly disagree to 6 = strongly agree.
Training Workshops
Trainer Workshop
The initial training for MI trainers was designed to provide experienced HIV clinical psychologists and psychiatrist with an overview of MI techniques. The incorporation of MI into clinical practice was based on the principles of collaboration, evocation, and honoring the patient’s autonomy described by Rollnick et al. 20 The training began as a review and conference call discussion of the training manual among the team members. A trainer workshop was then conducted in the Buenos Aires clinics, as two 3.5-hour sessions and included additional revision as required.
Health Care Provider Workshop
Four clinical psychologists with experience in interacting with HIV/AIDS-infected patients working on public hospital (2) and private organization (2) provided the training. The health care provider workshop was provided as 2 half-day sessions. The first session was focused on the principles of MI and incorporation of MI techniques into regular patient visits. Providers were taught to use patients’ motivation, energy, and commitment to elicit motivation to change rather than imposing it. A sample video produced by the team, illustrating a session utilizing MI techniques between a health care physician and an HIV-positive patient, was presented in segments. Each segment presented different MI techniques, including open-ended questions, active listening and summaries, recognizing ambivalence, and eliciting change talk. In addition, segments include illustration of the spirit of MI, using patients’ desires, abilities, reasons, and needs for change to honor the patients’ autonomy. At the conclusion of the first session, providers were asked to take home their own preworkshop video recording and to view and evaluate the videos, considering the feasibility of introducing MI techniques into their typical consultations.
During the second session, participants shared briefly their experiences with viewing their own consultations and their opinions with regard to incorporating MI into their consults. Participants were grouped in pairs and practiced the MI techniques reviewed in session 1. Participants interchanged roles several times, either acting as a nonadherent HIV-positive patient or acting as a physician, to incorporate the MI skills into their existing techniques (Figure 1).
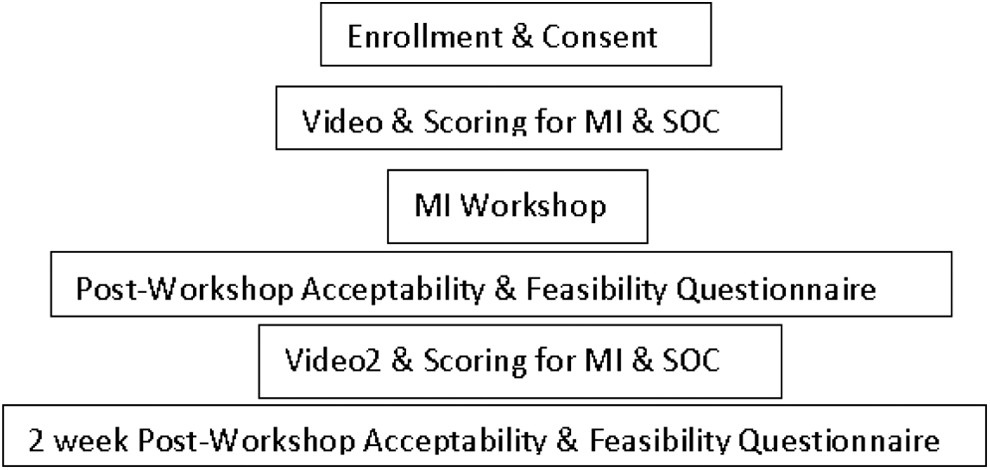
Study flowchart.
Results
Participants
Infectious diseases physicians (n = 12) specialized in HIV care from public and private practice participated in the workshop intervention. All participants reported the willingness to try MI with their patients (score 6.0) as well as a technique well suited to working with difficult patients (score 5.7) and that MI would be helpful in understanding how to guide patients rather than imposing, to use open-ended questions rather than closed questions, to practice active listening and summarize, recognize ambivalence toward change, and to evoke commitment from patients. In addition, participants felt comfortable using the techniques during the practice session and expressed the willingness to use MI with their difficult patients. However, only 7 of the 12 participants thought MI would fit in their practice or would have enough time to use the techniques in their time schedule (score 4.8; see Table 2).
At 2 weeks postworkshop intervention, of the 12 participants, 11 responded to the questionnaire (see Table 3). Participants agreed or strongly endorsed using MI skills (score 5.3). Nine participants felt comfortable using MI skills with their difficult patients (score 5.3), practicing active listening and summarizing (score 5.0), used empowerment to evoke commitment (score 5.0), and perceived having enough time using MI during their regular visit (5.3). Two participants reported they were not comfortable using MI skills and 1 did not have enough time to include MI during a routine visit.
Video Coding
Twelve participants completed a video recording. Nine participants illustrated appropriate utilization of at least 1 of the MI techniques following training. The use of open-ended questions and active listening illustrated by all participants and the application of short summaries and positive feedback were observed in 6 of the 9 recordings. Six participants were able to introduce teaching and guiding more than directing, 4 participants gave positive feedback, and empowerment and teach back was practiced once. At the end of the consult, 2 participants used the MI scale techniques as a method of quantifying patient willingness to be adherent. The remaining 2 participants did not apply MI techniques and 1 participant’s video recording was unreadable.
Standard of Care
At baseline, participants provided an average of 1 element of each of the SOC subscales (education mean = 1.6, type of education provided mean = 1.0, systematic planning mean = 1.6, support in consecutive visits mean = 1.1, and general support mean = 0). At postintervention workshop follow-up, a Wilcoxon signed rank test indicated that the number of elements of the SOC provided significantly increased for the education, Z = −2.375, P = .018; general support, Z = −2.12, P = .034; and follow-up support, Z = −2.32, P = .02 and showed an increasing trend in systematic planning, Z = −1.69, P = .09. For example, after MI training, physicians inquired about possible difficulties with adherence, determined the underlying causes of nonadherence and patient- and provider-generated solutions, and the providers inquired about side effects and gave feedback about the effectiveness of the treatment using VL and CD4 results.
Discussion
This study examined the uptake of MI techniques following a training workshop designed for routine physician consultations with challenging patients in Buenos Aires, Argentina. Overall, MI was well received among HIV health care providers, and reactions were generally favorable and consistent with the results of other studies. 21 As hypothesized, MI was found to be an acceptable and feasible strategy for Argentine health care providers in clinical settings in both public and private health care.
This is the first time that MI has been introduced among HIV physicians at public and private facilities in Buenos Aires, Argentina. Previous MI research has shown that workshops may produce some immediate gains in MI competence. 22 For busy physicians with limited time for both formal training and interaction with patients, MI can provide positive results in as little as 5 minutes. 9,21,23 However, these gains do not always endure. 24 The current study found that the majority of providers found MI to be feasible in the time frame allowed, and short-term follow-up suggests that many providers were able to maintain the use of the techniques. Motivational interviewing is not a simple counseling approach to master, and research suggests that it may be difficult to suppress prior counseling habits. In addition, there is a tendency for training to decay over time unless there is a systematic posttraining support, supervision, and training. 8 Future studies should provide longer term follow-up and emphasize the availability and utility of support services in maintaining MI.
The present study was developed to explore and address the feasibility of HIV health care providers integrating MI skills as an additional tool in the already complex management of nonadherent, disengaged HIV-positive patients. In contrast with previous studies designed to improve provider adherence counseling, 25 this study found the use of MI to include improvement in the provision of adherence counseling strategies, for example, planning of medication intake, exploring difficulties with adherence, generating solutions, discussion of side effects, and providing feedback about effectiveness of treatment and adherence.
The primary limitations of this research are associated with the small sample size and brevity of follow-up for this pilot study. Although MI was well received by the providers participating, the process of HIV management is lengthy, and providers may need more intensive training and practice using MI techniques to fully incorporate their routine use in care.
In conclusion, MI appears to be an acceptable and feasible strategy, which can enhance the provision of adherence consultation in the delivery of more comprehensive clinical care for challenging patients. Large-scale, long-term studies addressing provider skill maintenance in the engagement and retention in care of challenging patients are needed to evaluate the usefulness of MI as a tool in the HIV care armamentarium in Argentina.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.