
Abstract
Black/African American women represent 54% of new HIV cases among all women in the United States, face higher rates of morbidity and mortality, and are often understudied. The patient–provider relationship is an important motivator to keeping people who live with HIV retained in care and adherent to a medical regimen, thereby improving chances for viral suppression and maintaining overall better health. This scoping review sought to determine the extent of documented provider actions that encourage Black women with HIV to stay engaged in care. The review investigated five databases for peer-reviewed studies in the United States that included Black women from 2009 to 2023 and specifically described beneficial provider actions or behaviors. Of 526 records, 12 met the criteria. Studies revealed that women are motivated by providers who create a respectful, nonjudgmental emotionally supportive relationship with them rather than those who rely on an authoritative transactional exchange of information and orders.
Plain Language Summary
This review sought the perspectives of Black women with HIV on actions their providers take that help retain them in medical care.
Keywords
Introduction
According to the CDC, Black/African American people a continue to bear the highest burden of HIV compared with other races in the United States. 1 In 2021, Black people made up 13% of the population yet accounted for 40% of new HIV cases. 1 The disparity is even more acute for women as Black women comprise 54% of new cases among all women followed by white women and Latinas at 22% and 19% respectively. 2 Despite this stark disparity, relatively few studies or tailored interventions focused exclusively on Black women with HIV.3,4
Currently, the CDC estimates that, for every 100 women diagnosed with HIV, 76 have received some care, 64 are virally suppressed, and 58 are retained in care. 5 Importantly, of those prescribed antiretrovirals and retained in care, 77% achieve durable viral suppression with some HIV clinics reporting as much as 85% to 87% suppression among patients.6,7 The CDC defines having received some care as having had at least 1 viral load or CD4 test per year and retained in care as having had 2 viral load or CD4 tests at least 3 months apart per year.8,9 Patients with HIV who are not retained in care regularly are less likely to remain undetectable and more likely to see greater disease progression and mortality. 10 For this reason, retaining as many people in care as possible becomes critical to saving lives, reducing transmission and ultimately ending HIV as an epidemic.
Previous quantitative and qualitative research has found that HIV patient satisfaction with the overall clinic environment, including relationships with providers, influences patients staying in care and adhering to an antiretroviral regimen.11–15
Research suggests that patient satisfaction, however, is directly influenced by the quality of patient–provider interactions. 16 Oetzel et al's study of 344 people with HIV 16 suggests that improving patient satisfaction is a matter of improving patient–provider interaction and showed that patient–provider interaction for people with HIV actually leads to patient satisfaction with overall services as well as adherence. These researchers recommend that research and interventions be aimed at bettering this relationship. 16
Beach et al 17 also found a significant relationship between the quality of the patient-provider relationship and the patient's willingness to stay in care and achieve viral suppression. Specifically, they examined the extent to which patients’ perception that the provider knows them “as a person” influences their receptivity toward being prescribed highly active antiretroviral drugs (HAART), their willingness to adhere to a HAART regimen, and the likelihood of having an undetectable viral load. They found a strong positive correlation between patients' perception that the provider knows them “as a person” and each of these variables. Moreover, patients who felt their provider knew them as a person missed fewer appointments, had greater confidence that antiretroviral medicine was beneficial to them and reported a higher quality of life. 17 An integrative review of qualitative and quantitative research to identify the specific actions providers take to facilitate a strong interpersonal relationship could help other providers know with greater certainty what they can do to keep more patients returning to appointments and adhering to their regimens. Preliminary Google Scholar searches, however, yielded little detailed information on the nature of patient–provider relationships for Black women with HIV within the past 10 years. One qualitative study based on in-depth interviews by Okoro 18 found that women who felt that their provider knew them as a person were more confident about treatment and care, echoing Beach et al's findings. 17 As a precursor to an integrative review, scoping reviews are conducted to determine the breadth of literature on a subject and to determine the appropriateness of a research question.19–21
Objectives
The first objective of this scoping review was to gather corroborating research that identifies specific provider actions that encourage Black women with HIV to stay in care and adhere to medical recommendations. The second objective of this review was to determine if enough studies had already been conducted to develop an integrative or systematic review on this subject. The following research question guided the queries: “What provider actions help keep Black women with HIV in care?”
Methods
Following the guidance of Munn et al, Pham et al, and Tricco, et al,19–21 authors of this scoping review planned clear objectives and a search strategy in advance. Five databases were identified for medical relevance. The authors practiced with several search strategies, refining them with successive searches. By searching for a combination of these terms in the abstract, titles and/or author keywords, more results surfaced that specifically addressed Black women in relation to providers.
Eligibility Criteria
Eligibility was set to allow for a wide but relevant possibility of articles, and the researchers compared each article to the research question in order to make final selections. Papers met eligibility criteria if they discussed a qualitative, mixed-methods, quantitative experimental, or nonexperimental study on HIV-positive patient–provider relationships that included women who self-identified as Black per the definition in footnote 1. Papers must have been peer-reviewed journal articles published between January 2009 and October 2023, written in English, focused on women in the United States, specifically discussed the experiences of Black women with providers, and identified provider actions that helped women stay in care.
The authors sought to identify articles that discussed Black women independent of other patients with HIV because (a) Black people have a historical relationship with the medical establishment in the United States that creates a potential for friction, discomfort, and sometimes reluctance to engage in care14,22,23; (b) the virus predominately affects men in the United States, so more studies have been directed at men; and (c) studies that combine the experiences of all patients with HIV together may not be able to disentangle the concerns of Black women who may experience internalized racism combined with the needs and pressures of family care, and the emotional burden of acquiring HIV most likely through heterosexual contact.
A long date range was chosen due to low results from preliminary searches, but the date needed to be within the post-HAART era after which medications were much more tolerable. In 2009, the World Health Organization and the Office of AIDS Research Advisory Council in the U.S. Department of Health and Human Services updated their guidelines to start antiretroviral therapy earlier than previously issued guidelines signaling an era when HIV was manageable as a chronic illness with proper care.24,25 Studies were limited to the United States because numerous studies focus on Black women in other parts of the world that have very different healthcare systems and social contexts.
The first author conducted searches throughout 2019 with follow-up searches in each database in March 2022 and September/October 2023.
Information Sources
The following databases were searched: CINHAL, PubMed, Cochrane, Medline, and Scopus. Hand searches were conducted on the documents meeting the selection criteria. Search terms included: African American women, Black women, HIV positive, HIV seropositive, patient, provider, communication, interaction, relationship, and engagement. To expand the search, additional terms were added at a later time including: nurse, physician, doctor and case manager. Limitations on searches varied according to database availability but all included English language, peer-reviewed, and the publication date range. For those that made additional limiters possible, the United States was set as the geographic location, journal article as type of source, and female sex or gender, if available.
Supplemental Table 1 provides search strings used for 2023 updates on previous searches. Search updates were limited by date so as to not produce duplicate results. The results of new searches were added to the existing article count.
Selection of Sources of Evidence
One researcher read each title and abstract from the search outcomes, discarding immediately those that were not relevant and those that were repeated from other searches. Reasons for immediate discard were a focus on men exclusively, a focus on women outside of the United States, a focus on HIV prevention, a focus on an illness other than HIV, or the article being a type of systematic review itself. After immediately discarding those that were not relevant, 55 articles were kept to be read in detail.
Data Variables
The following data were extracted from relevant articles: publication information, primary purpose of the study, theory or framework (if any), study design, setting, sample, number of groups, protocol, instruments used, analytical method, findings, provider actions discussed, other unique findings, and recommendations. The primary purpose of the study was placed on an Excel spreadsheet in order to understand how many and which studies set out to examine patient–provider relationships or if discussion on patient–provider relationships emerged out of a different purpose.
Articles were kept for the final scoping review if the results included specific references to African American or Black women and if the authors described provider actions to help keep women in care based on these data. The final evidence table was reduced to those data that contributed to answering the research question: What provider actions help keep Black women with HIV in care? Twelve articles were retained for the final review. See Figure 1: “PRISMA flow chart” for the inclusion and exclusion process.
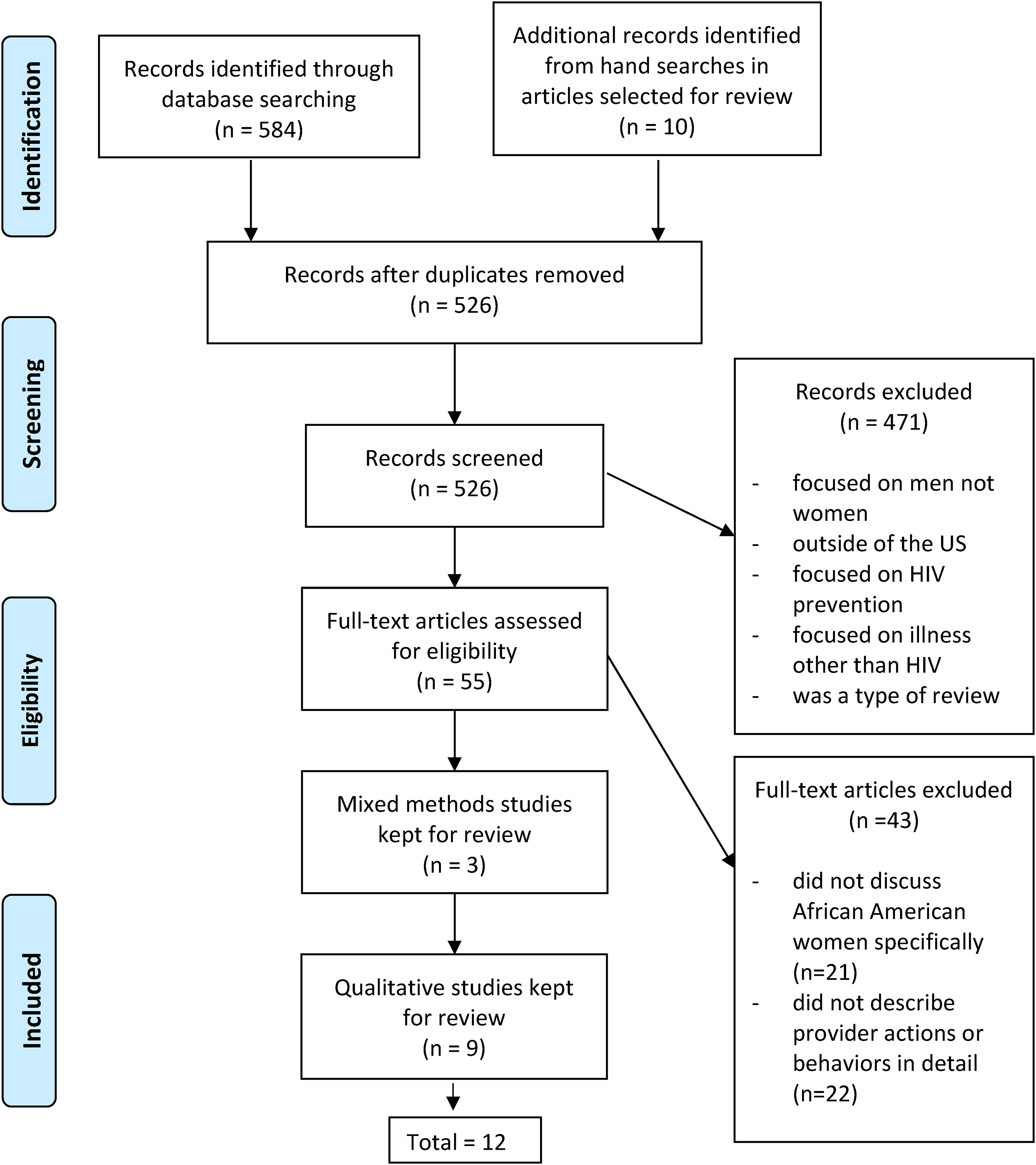
PRISMA flow chart.
Ethical Approval and Informed Consent
Ethics approval and informed consent were not required for this systematic review.
Results
The first author grouped the studies according to those that were exploratory and those focused on an intervention. The purpose of this grouping was to identify how many studies attempted to address this population's needs through intervention and if insights gained from those interventions added value to insights gained from the exploratory studies. Two of the 9 involved an evaluation of an intervention.26,27 Commonalities among the sample, settings, findings, provider actions, and recommendations were also identified. Participant information from the 12 final studies was synthesized in order to understand overall sample characteristics including the average age and the range of years since diagnosis.
Characteristics of Sources
Table 1 summarizes each source including the citation, study purpose, design, and theoretical framework used (if any), data collection method and setting, sample size, and provider actions identified by study participants.
Evidence Table.
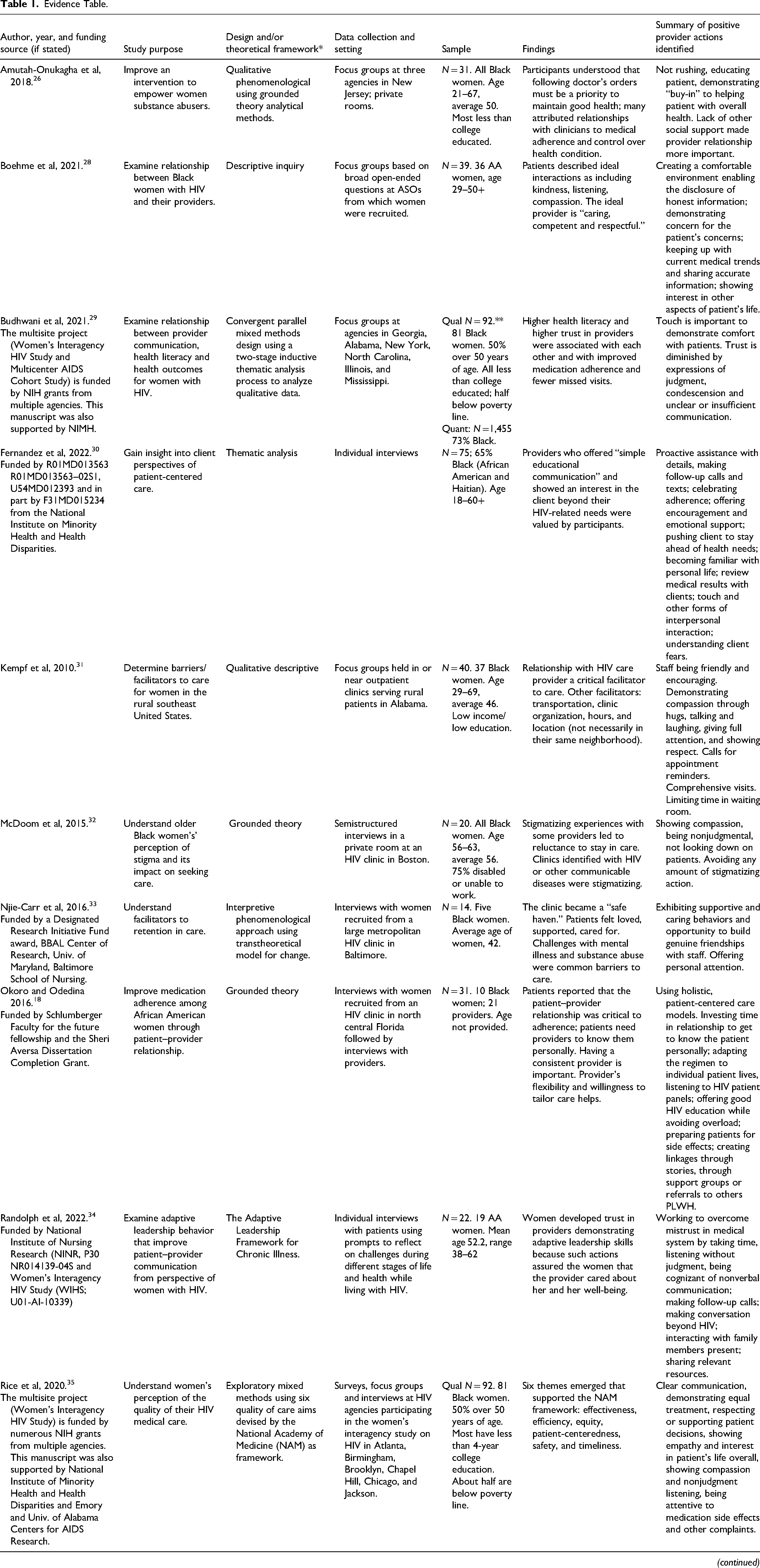
*Contains information as described in the articles.
** Budhwani et al and Rice et al are studies conducted on the same sample.
Types of Studies and Appraisal
Nine of the studies that met the criteria were qualitative and three were mixed methods, although the portions that yielded data relevant to this research question were qualitative. Each study was analyzed for its contribution to the research question as well as its overall quality based on concepts offered by Malterud. 37 Malterud37,38 argues that the value of qualitative studies to medical research lies in their ability to answer questions related to human behavior that cannot be understood through controlled experiments. As human beings, both patient and practitioner behaviors are informed by opinions and experiences. Understanding the communications and interactions involved in health outcomes requires the kind of contextualized observation and inquiry that can be accomplished through qualitative studies. 37
Malterud 37 offers guidelines to help readers of qualitative studies ascertain their usefulness for the topic at hand by encouraging readers to assess three major factors: (1) reflexivity (based on the degree to which authors disclose their role and motivations); (2) transferability (based on the study design and sample); and (3) interpretation and analysis (based on details of data extraction). 37 All of the studies met most of Malterud's criteria for rigor. If the researchers fell short of Malterud's criteria, it was in documenting reflexivity. Only the authors of two papers explicitly described their personal positions and backgrounds in relation to their research topic. The others discussed academic knowledge to frame the topic but not their personal positions and motivations. The two that did so were Black women, perhaps motivated to explain a shared identity with their research participants.
Nevertheless, the studies in aggregate were clear about their aims, rationale for the design and choice of theory, sample selection, the characteristics of their samples, and analytical methods. They all made appropriate and informative use of quotes to illustrate key points and present the participants’ voices distinctly from their own. Overall, the contribution of these studies to medical research is that they provide a window into what this population needs, wants, and values in their care, enabling providers to plan in advance for beneficial interactions that can reduce patient attrition.
Study Purposes
Each of the studies described provider actions that help keep Black women in care and identified responses tied specifically to this population. Two of the studies were aimed at evaluation and quality improvement for interventions, while the rest were exploratory. Only 4 of the exploratory studies set out to understand patient–provider relationships specifically. Three studies sought to understand women's perceptions of their quality of care in multiple arenas including but not limited to the patient–provider relationship. Five studies sought to ascertain general barriers and facilitators to care for women in a particular service area and learned that a good patient–provider relationship was an important motivator to staying in care and then went on to describe those provider actions. Conversely, the studies collectively revealed that negative interactions with providers can be a deterrent to staying in care.
Study Designs and Theoretical Frameworks
All of the studies used a type of qualitative design to guide the research, including qualitative phenomenological, qualitative descriptive, interpretive phenomenological, thematic analysis, and grounded theory. Not all of the studies described using a theoretical framework, but those that did use the transtheoretical model for change, 33 intersectional theoretical framework, 36 the National Academy of Medicine's quality of care aims, 35 and the Adaptive Leadership Framework for Chronic Illness. 34
Data Collection and Settings
Data were collected via telephone interviews or via in-person focus groups or interviews that were conducted in the clinics from which participants were recruited. Four of the studies used focus groups, 8 used in-depth interviews, and 1 included interviews with providers in addition to patients.
Participants were recruited from HIV or infectious disease clinics in urban centers on the East Coast and in the Southeast, with the exception of 1 study in Chicago and 1 study that included women living in rural Alabama. None covered Western locales.
Samples
In total, these studies included 331 women who identified as African American or Black. The participants ranged in age from 21 to 69 and the average age across studies ranged from 42 to 57.18,26–36 Not all studies reported on the socioeconomic status of participants, but those that did described a large proportion of participants as having less than a 4-year college degree with many being low income or living below the poverty line.26,27,29,31,32,35
Synthesis of Results
Of the studies that met the criteria, 5 were exploratory examining the barriers and facilitators to care, 2 were conducted to test or demonstrate the efficacy of an intervention, and 5 aimed to understand patient perceptions of quality care particularly the relationship with providers.
Exploratory Studies
The exploratory studies revealed 6 important themes for retaining women in care: provider relationships and staff attitudes; structural and organizational factors at clinics; whether or not clinics felt like safe spaces; the development of patient-centered partnerships; the extent to which women perceived that they were judged by providers; and, a need for formal supports to counteract stigma and emotional isolation.
Provider Relationships and Staff Attitudes
All of the studies provided examples of provider and staff actions and attitudes that contributed to beneficial patient–provider relationships, with Okoro et al, Kempf et al, and Rice et al's work resulting in a veritable checklist of recommendations as indicated in the evidence table.18,31,35 Kempf et al 31 offered the most specific examples of provider actions in a study to determine barriers and facilitators to care for women in the rural Southeastern United States. These researchers conducted focus groups using a descriptive inquiry approach in order to allow the women to discuss what was significant to them. 31 Participants in their focus groups named 2ff“strong incentives” to maintain regular appointments at their clinic: their relationship with their provider and being made to feel welcome by other staff (Kempf et al 31 , p. 517). When participants in this study were met with friendliness, encouragement, understanding, caring, and respect by providers and clinic staff, they enjoyed their visits. 31 Similarly, Rice et al 35 and Okoro et al 18 underscored the importance of understanding the patient as a whole person, listening, and being nonjudgmental in all interactions.
Allowing for an Emotional Connection
Throughout these studies, women who seemed satisfied with their clinics and/or providers used strong words to describe an attachment. Women used emotional terms like “love” and “spiritual connection” in relation to providers with whom they worked well.26,31,33 Some expressed genuine sadness when a provider relationship ended. 27
Patient Health Literacy
Budhwani et al 29 explored the relationship between patient health literacy, the quality of patient–provider communication, and the impact of these two variables on patient outcomes related to medication and appointment adherence. Patients in this study who indicated greater health literacy reported higher quality patient–provider communication which was associated with fewer missed appointments. Through the qualitative portion of this mixed methods study, researchers found two important actions that increased trust: touch and respectful communication. In contrast, other actions diminished trust: unclear communication and expressions of judgment. The researchers also observed an association between higher patient health literacy and higher trust in providers arguing that providers should actively seek to help increase patient literacy, as it could result in improved relationships with providers. 29
Structural and Organizational Factors
Some participants’ desire or ability to return to a clinic was influenced by how well the clinic operated.31,35 For these participants, additional provider actions that helped them stay in care were: more comprehensive visits, such as getting blood work done on the same day; and shorter time in the waiting room so they wouldn’t have to risk being seen by people who may not know their HIV status; appointment reminder calls the day before each appointment; and providers encouraging the importance of keeping appointments in a compassionate manner.31,35
Clinics as Safe Spaces
Participants in one study viewed their HIV clinic as a “safe haven” and reported behaviors among clinic staff that were “supportive and caring.” 33 In this safe haven, participants described a sense of “being loved, cared for [and] at peace.”33 The clinic staff were an important part of these patients’ social support system along with family and friends; and staff commitment to the women's health was a motivating factor in keeping appointments. 33 The study included more newly diagnosed participants than the other studies. Most of the patients in this study were newly diagnosed and those who were not had recently returned to care. Moreover, the responses of the newly diagnosed were so similar to responses given by those who had been in care for many years that it indicated this study's clinic understood and applied effective retention strategies from the start with its new patients.
Patient-Centered Partnerships
One study by Okoro and Odedina sought to compare providers' perceptions of what they needed to do to create an effective patient–provider relationship with women's views. 18 They determined that patient-centered care was critical to adherence and kept appointments and defined patient-centered care as a partnership between the provider, the patient, and that patient's close social support individuals. 18 This was the only study in the current review that also sought providers’ input by interviewing a range of healthcare professionals: nurse practitioners, registered nurses, a pharmacist, physicians, social workers, community health workers, and a public health professional. The findings showed it was important for the provider to “know the patient as a person,” be able to educate her on the benefits and potential side effects of certain medications, and take time to understand the woman's life overall. 18 The providers understood that a quality patient–provider relationship was important to maintaining their patients’ adherence and that the relationship-building process required additional labor on their part, but was necessary to earn this population's trust. 18
Providers in the Okoro and Odedina 18 study acknowledged the importance of figuring out how to create a partnership with each new patient and that rushing appointments led to negative perceptions among patients. Providers sought ways to meet individual patient needs such as flexible appointment schedules and mailing medications to rural patients. 18 Providers also observed the benefits of finding a point of motivation for their patients to stay in care, such as the patient's children, and used that as a way to encourage women to stay healthy. 18 Patients wanted a consistent provider; even postponing appointments if the doctor with whom they had a relationship was away, so as to avoid having to begin a new provider relationship 18
Participants in the Rice et al study 35 perceived higher quality of care when their providers listened to them, sought to work with them in a participatory manner, and eschewed stigmatizing actions like avoiding touch or using excessive protective gear. Echoing the Okoro and Odedina study, their participants reiterated the importance of being able to develop long-standing relationships with providers and explained that switching providers created distress.
Fernandez et al 30 sought to understand clients’ perspectives on patient-centered care as it was enacted by medical case managers and medical care providers. The women interviewed highlighted that interpersonal practices enacted by their care providers were facilitators to their retention in care. In addition to efforts at interpersonal communication, the actions that women responded to included proactive steps to contact them, help them through paperwork if needed, offer appointment reminders, and guidance on health or life-related concerns. 30 Similarly, Boehme's participants described their ideal providers engaging in practices that could be described as patient-centered care. 28 These providers demonstrated care by taking time with their patients, focusing on the things that concerned them, working to stay informed of new developments in treatment, and engaging as if they were friends.
Enabling Self-Determination
Randolph, et al 34 used the Adaptive Leadership Framework for Chronic Illness to explore how both providers and women with HIV adjust to become patient- and self-advocates during the clinical encounter. For patients, this can entail changing behaviors or increasing skills and knowledge to adjust to a diagnosis; for providers, this can mean rousing the patient and their family to take action in order to keep ahead of medical and health challenges. 34 For women with HIV the most outstanding adaptive leadership trait Randolph, et al heard was “my provider cares about me.” 34 This sense of caring, they report, emerges from and is increased by communication and taking time to build trust. Adaptive Leadership in this article aligned closely with concepts of patient-centered care identified in other studies. In the adaptive leadership framework, providers would proactively connect patients with resources, especially newly diagnosed. In an adaptive leadership scenario, a caring provider will encourage the patient to seek new information and make life adjustments to be in charge of her health care.
Perceived Judgment by Providers
The ongoing role of HIV stigma in women's perceptions of how providers may judge them was a lingering concern for women over 50, despite observing improvements in provider compassion over time. 32 McDoom et al revealed that the experience of stigma from providers in the early days of the epidemic led to ongoing mistrust of providers and reluctance to remain in care when relationships faltered. 32 The stigma women experienced was related to stereotypes associated with HIV such as intravenous drug use or promiscuity. 32 For women in this study, perceptions of what the doctor thought about them affected their interest in staying in care. Despite what the provider might intend to convey, women did not want to engage in care if they thought the doctor “looked down on them,” was not truly interested in their health, or had an otherwise “negative attitude” toward them (McDoom et al, 32 p. 99).
Formal Supports to Counteract Stigma and Emotional Isolation
Both of the studies that focused on older women argued that formal supports, such as providers, clinic staff, and AIDS service organization staff, became an increasingly important source of social support as women with HIV age.32,36 Ageism combined with HIV-related stigma made it difficult for older women to find support among informal sources such as family, friends, churches, or social groups compared with other chronic illnesses that disproportionately affect Black women, such as diabetes and breast cancer. 36 Warren, et al 36 stressed that providers and HIV advocates sometimes became the only consistent and trustworthy support for some women.
Studies Designed to Evaluate an Intervention
The 2 studies designed to evaluate interventions revealed that the quality of the relationships with providers and demonstrations of provider commitment played a role in determining whether or not patients would persist with care.26,27 These studies emphasized that providers need to be willing to take time with patients, to expect that it takes time to build trust, and to be authentic in their interactions. Participants in both highlighted the importance of having a deep affinity for their providers, even a “spiritual connection” as one participant explained, in order to have a productive relationship that supports medication adherence.
Taking Time and Demonstrating Buy-in
Of the two studies that examined an intervention, one was conducted to gain participant feedback on Project THANKS, an intervention for people with HIV who abuse substances. 26 Through focus groups, women in this study explained that a good relationship with their providers motivates them to keep appointments and adhere to medication. Women noted that the providers they liked did not rush, answered questions, provided education on HIV, and showed they “bought-in” to help the women be healthy. 26
Professional Health Navigators and Their Authenticity
The other intervention-related study was developed to evaluate patient experiences with nurse guides in a program created to help women of color with HIV navigate medical and other resources. 27 Most participants were newly diagnosed, had not previously engaged in care, or were returning to care. For the newly diagnosed patients, education from the nurse guides on the survivability of HIV was critical. It was important to have someone to discuss the side effects of medication. The nurse guide showed genuine, not artificial or “phony” concern; was friendly; actively found solutions; was easily accessible by phone; and called the patients to check in on them (Sullivan et al 27 , p. 52). Participants felt as though they could talk candidly to the nurse guide, who then supplemented the lack of social support in other areas of their lives. 27 The nurse gave them instruction on how to ask questions during appointments and cleared up confusion about information offered by physicians and other providers. 27
Both intervention studies reinforced the insights offered by the exploratory studies chiefly by demonstrating that patient motivation and adherence improved when relationship-building strategies were deliberately employed. In both studies, effective patient–provider relationships developed when providers took the time to show genuine concern, responded to the women's questions, and helped patients learn about HIV and their medications.
Discussion
This review sought to determine the scope of existing literature that identifies provider actions that help keep Black women with HIV in care and was guided by the research question, “What provider actions help keep Black women with HIV in care?” All study types were under consideration, however only 9 qualitative studies and 3 mixed methods studies discussed responses to the research question with sufficient detail to be instructive. The articles found through these searches offer viable practice recommendations. These 12 studies provide helpful insights through participant direct quotes on what works for them individually and through the authors’ aggregation and analysis of all participant input. This limited number of articles offers valuable foundational material for a future systematic review, especially with increasing guidance on reviews now available such as that provided by Peters, et al. 39
The findings show that a combination of provider interpersonal skills and functions of the clinic help women stay in care. Patient-centered care that considers their needs as a whole person is important to this population because some women may not find the social support needed to manage HIV and associated comorbidities elsewhere.
This review reveals that many Black women with HIV are motivated by an emotional connection to their providers and/or clinic staff and a sense of safety within the clinic or practice. Provider and staff attitudes are crucial because emotional support from providers is an important motivator for return appointments overall, in some cases counteracting a lack of emotional support elsewhere due to the stigma associated with HIV.22,27,33,36
Multiple recommendations on provider actions that improve relationships and support retention in care are offered in these studies. Foremost, taking time to demonstrate buy-in with authentic interest is foundational to a trusting relationship. Addressing mental health concerns and substance abuse challenges helps keep patients adherent to medication.22,26 Comorbidities are often challenging for women to manage even when HIV is under control, therefore providers should be prepared to discuss these.26,36 Providers should seek something that motivates each woman individually to keep her returning for appointments and regularly listen to patient advisory panels so that they can stay mindful of women's views. 18 Offering women training to improve their own health literacy can improve their relationship with providers and enable them to help other women with HIV. 18 Providers should be cognizant of women's struggles with stigma, avoid any type of judgmental behavior, and use touch to signal comfort with the woman's serostatus.27,29,31,32
While individual provider actions are motivators to appointment and medication adherence, women also wish to experience HIV clinics as welcoming places where they will not be deemed promiscuous or guilty of other socially unacceptable behavior. Ideally, clinics are places where they can see “friendly faces,” feel encouragement, and concern, love, caring, genuine friendship from the staff and where they can be at peace.31,33 Some clinics may need to remove the words HIV and AIDS from their name. 32
In addition to friendliness, women evaluate clinics based on organizational and structural factors. Their quality measures include limited time in the waiting room so as to avoid other people; reminder calls or texts for appointments; completing blood work on the same day; information and resource sharing; offering self-care programs for patients and HIV education programs for families; and utilizing patient navigator programs staffed by authentically engaged practitioners.18,26,29,31,33,36
Implications for Public Health
Together, these studies emphasize the importance of the following 11 themes in facilitative provider actions across time and location: (1). Provider relationships and staff attitudes heavily influence women's experience during clinical encounters. (2). Providers who allow for an emotional connection can engender trust. (3). Patient health literacy and adaptive leadership enhance trust in providers and are worth the effort to foster. (4). Structural and organizational factors at the clinic are as important to retention as interpersonal relationships. (5). The most highly regarded clinics are those that feel like safe spaces. (6). Women prefer patient-centered partnerships in which they are seen as decision-makers over didactic instructions about their health. (7). Providers who enable self-determination create a feedback loop that increases trust in the provider. (8). Any actions that can convey judgment on the part of providers must be assiduously avoided. (9). Providers and other health care workers are the formal supports that can counteract stigma and emotional isolation for women who may not have social support elsewhere. (10). There is no substitute for taking time and demonstrating buy-in to women's success at managing their health. (11). The availability of authentic professional health navigators is an important enhancement to be employed more often.
Many Black women with HIV have to manage multiple social, economic, and personal hurdles when it comes to maintaining the medical regimen that will enable them to lead long and healthy lives. For public health officials, the articles included in this study demonstrate that providers are key figures in women's choices to stay involved in care. Ending HIV as an epidemic requires that the vast majority of people with HIV achieve undetectable status. Four decades into the HIV epidemic, shame, fear, and stigma continue to stymie African American's engagement in care. 40 Provider actions that are patient-centered, nonjudgmental, and anticipatory can be the defining line for many Black women needing to remain in care. The 12 articles in this scoping review are a testament to the essential role of providers and make a case for both their training and their support by clinic management.
Limitations
This review has limitations in both the process and outcomes. Hand searches were limited to those that met the final criteria, but could have been more exhaustive had the researcher scanned articles that did not meet the criteria. Searches did not include other illnesses that disproportionately burden Black women which might augment the information found in this article. The search was limited to HIV not only because it was the topic of interest, but also because the social stigmas historically tied to this virus make it potentially dangerous for people to be open about their status, and to be suspicious of some providers.
An important limitation on the total body of evidence is that the average age for participants was older, even when studies were not intentionally seeking older women. This could be the result of self-selection among participants indicating that older women are more comfortable discussing HIV and perhaps there is greater internalized stigma among younger women. Conversely, it could mean there is less stigma among younger generations and therefore less of a need to gain social support from providers. This conundrum is unaddressed by this work and calls out for new research in the area.
Aside from Chicago, these studies were limited to the East Coast and Southeastern states, leaving the Mid-West, West, Northwest, and Southwest states unexplored. Other regions are important to study as they include locations where the Black population is smaller, possibly resulting in fewer options for informal support and less familiarity among providers in engaging with Black patients.
It is notable that two-thirds of the articles are found in journals that focus on HIV, women's health, or on low-income populations. Four of the 12 articles were published by AIDS Patient Care and STDs indicating a strong interest in this population by this journal. None of the articles were found in journals targeting wide, generalized public health audiences. Lastly, the studies identified for the review were qualitative based on smaller samples of self-selected participants and so may not capture the variety of opinions of the diverse population of Black women with HIV.
Strengths
In regard to the first objective, the final pool of articles offers enough corroborating information for providers and clinicians to understand what this population seeks in providers and what providers can do to be effective at engendering beneficial relationships. Many other articles acknowledge that the patient–provider relationship is important to women, including ones read in the process of this review but not included in the final analysis,41–47 however they don’t describe what providers actually do to create a strong relationship as these articles do. Moreover, this pool included interventions that showed progress in patient–provider relationships can be made by following some of the action steps women describe.
The qualitative data in these articles allows for the voices of women to be documented and amplified. This review highlights the voices of an often-marginalized population experiencing a complicated and highly stigmatized virus in a way that can lead to improved patient–provider relationships within the scope of HIV care and beyond. Moreover, by limiting the searches to HIV, which remains a socially complicated illness, this study illuminates the extra steps some providers and clinics undertake in order to better support a population that may face racism and marginalization in healthcare settings.
The database searches were conducted and repeated over a period of 48 months in 5 databases. The studies in the pool were reduced to those that explicitly stated actions providers could undertake to make improvements in the relationships with Black women seeking HIV care and therefore this collection of studies serves as actionable best practice guidance for providers.
With regard to the second objective, this review met the objectives of a scoping review, which is to determine the breadth of the existing literature. This review shows that there is an opportunity for future researchers to expand on the twelve articles retrieved.
Conclusion
In conclusion, provider relationships for this population cannot be simply transactional. Being a technically competent provider is insufficient for building trust and keeping patients returning. This review demonstrates that providers are successful when they are attentive to the whole patient rather than just her HIV concerns. Such training should be part of HIV provider education and offered through continuing education credits. Providers should be able to discuss or consider care coordination with patients’ other providers, offer functional mechanisms for staying in care such as appointment reminders, foster medication self-management related to HIV management, and remain keenly aware that they are an important source of emotional support for a population that may not get that support elsewhere. Providers who are not prepared to give emotional support to these patients should work alongside professional health navigators or other clinicians who can. Providers in management roles need to foster facilities that are supportive, unbiased about patients’ sexuality, and completely devoid of judgment and stigma. 33
The limitations in the pool of studies point to the need for future research. The fact only four studies set out to understand patient–provider relationships suggests there is room for research that hones in on this important social interaction. Published studies to date leave out participants from major regions of the country revealing that the voices of many women remain unheard.
Supplemental Material
sj-docx-1-jia-10.1177_23259582231224232 - Supplemental material for The Provider's Role in Retaining Black Women With HIV in Care: A Scoping Review
Supplemental material, sj-docx-1-jia-10.1177_23259582231224232 for The Provider's Role in Retaining Black Women With HIV in Care: A Scoping Review by Kenja S. Hassan and David W. Coon in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
sj-pdf-2-jia-10.1177_23259582231224232 - Supplemental material for The Provider's Role in Retaining Black Women With HIV in Care: A Scoping Review
Supplemental material, sj-pdf-2-jia-10.1177_23259582231224232 for The Provider's Role in Retaining Black Women With HIV in Care: A Scoping Review by Kenja S. Hassan and David W. Coon in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Footnotes
Authors' contributions
Kenja Hassan served as the primary author in collaboration with David W. Coon. The authors collaborated on the search methods, eligibility criteria for the articles included in the review, analysis of the data, description of findings, drawing conclusions and final edits on the manuscript. Kenja Hassan had the idea for the project and conducted the searches.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Notes
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.