
Abstract
Introduction:
Middle-income countries are in need of research that uses theoretical-based models to assess factors that predict adherence to antiretroviral therapy (ART) and help in the design, implementation, and evaluation of interventions for nonadherent populations. In Mexico, the Information and Motivation and Behavioral Skills (IMB) Model of ART Adherence constructs is useful in describing and predicting adherence behaviors in various samples but has not been articulated to people living with HIV (PLWH) on ART. The aim of this was to characterize the IMB core constructs and identify correlates of ART adherence in an HIV-positive clinic sample in Mexico.
Methods:
A convenience sample of 109 HIV-positive patients attending their monthly visits at a local public hospital were interviewed with the Spanish version of the LifeWindows IMB ART Adherence Questionnaire (LW-IMB-AAQ) as well as a sociodemographic questionnaire. All participants were recruited from a hospital-based outpatient clinical care site.
Results:
Partial confirmation of the relationships proposed by the IMB Model of ART Adherence was found. As predicted by the model, only behavioral skills had direct association with all measures of self-reported adherence, and motivation was associated with behavioral skills. Information did not demonstrate significant relations to either motivation or behavioral skills, nor did it directly associate with adherence. Self-reported adherence did not associate with CD4 counts, nor did any of the IMB model core constructs.
Conclusion:
Applicability of the IMB Model of ART Adherence in this setting is discussed. The IMB Model of ART Adherence offered promise in this population and could help tailor population-specific interventions to promote high rates of ART adherence.
Introduction
Mexico continues to report fairly low HIV incidence. While its neighbors, United States, Guatemala, and Belize, have a prevalence of 0.6%, 0.8%, and 2.1%, respectively, Mexico reports that 0.37% of its population is living with HIV. 1 In Mexico, those living with HIV, as part of the universal access to comprehensive health care, have free access to antiretroviral therapy (ART), and a large proportion of the National Center for Prevention and Control of HIV/AIDS budget is used for the purchase of antiretroviral (ARV) medications. 2 In 2011, of the 225 000 people living with HIV (PLWH) in Mexico, 38,510 were on ART. About 66% of PLWH on ART have undetectable viral loads, and, in some states, this percentage is as low as 37.3%. 3 The main reasons identified for failure of ART adherence include (1) ART stock outs or lack of consistent access to ARV medications and (2) decisions to discontinue medication either because of side effects or because individuals on ART start to feel better. 4 However, with multiple and dynamic factors underlying the difficulties of ART adherence and decisions to terminate ART, it is likely that failure has multiple and presently poorly understood determinants among PWLH in Mexico.
Correlates and predictors of ART adherence across diverse populations have generally been organized into 4 categories: regimen characteristics, patient-specific factors, provider–patient relationships, and the overall health care system. 5 Within these, fairly consistent support for a relation between adherence and patient-reported symptoms, stressful life events, social or family support, 6 complexity of the regimen, and self-efficacy toward medication taking 7 have been established. Additionally, depression, 8 substance abuse, 9 and the relationship with health care providers 10 have been associated with adherence in previous research.
Numerous behavioral models have been proposed that provide guidance on how identified discrete correlates and predictors of adherence may interrelate, including the Psychological Model of Biological Health, 11 the Self-regulatory Model of ART Adherence, 12 and the Information and Motivation and Behavioral Skills (IMB) Model of ART Adherence. 13 The IMB Model of ART Adherence has proved to be useful in understanding the variables associated with adherence in different populations. According to the model, Fisher et al 14 explain that health behavior–specific information is a prerequisite to ART adherence. In order to achieve and sustain adherence, patients taking ARV medication with higher accurate information about the medication, medications’ side effects, drug interactions, and not possessing critical misinformation are needed. Motivation, according to the authors, is also a critical determinant of health behavior change and includes personal motivation and social motivation. Finally, the IMB Model of ART Adherence includes a third critical determinant for ART adherence, that is, specific behavioral skills that include an individual’s objective ability and perceived self-efficacy for the performance of adherence behaviors (see Figure 1). As we can see in Figure 1, it is not that someone who is well informed or well motivated shows high adherence, it is the behavioral skills of one that determine ART adherence. Information and Mmtivation are mobilized into actual behavior.
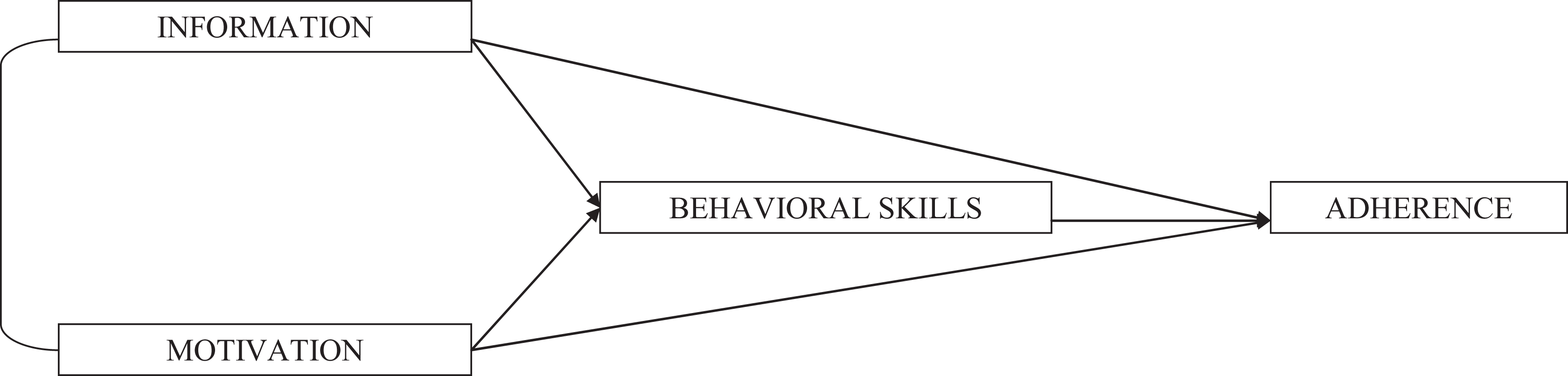
The Information–Motivation and Behavioral Skills model of antiretroviral therapy (ART) adherence.
The IMB Model of ART Adherence has been evaluated with samples of PLWH from Puerto Rico, Italy, and Mississippi and has received support for each of the proposed constructs and the mediation of the relation between information and motivation to adherence through behavioral skills. 15 –17 The applicability of the IMB Model of ART Adherence in the context of underserved, low literacy, low-income populations in unindustrialized countries remains. Low resource areas such as sub-Saharan Africa have shown favorable levels of adherence, although conditions of poverty and lack of formal education exist. 18 In Mexico, the average schooling is to grade 8.6, rates of illiteracy are 6.88% in those aged 15 years or older, 19 the average salary is less than US$5 a workday, and the society is largely characterized by collectivism. These and other factors may make the population of individuals living with HIV in Mexico unique from other populations in which the IMB model and IMB model-based measures have been demonstrated.
In preparation for developing a targeted intervention to promote high rates of ART adherence among PLWH in Mexico, we sought to evaluate the constructs of the IMB Model of ART Adherence and the associations between model’s variables within a cohort of PLWH receiving ART in Mexico using a translated version of a previously developed measure (LifeWindows IMB ART Adherence Questionnaire [LW-IMB-AAQ]). Consistent with the IMB model of adherence, we hypothesized that patient-reported adherence behaviors would be directly associated with behavioral skills and that behavioral skills would be associated with motivation and information. Although controversy remains regarding a “gold standard” measurement of adherence, 20 self-reported adherence measure was used, as we believed that in this study the assumptions behind the validity of the measure were true (self-report participants could reasonably answer the questions [when doses were taken, how many, or provide general estimate]; cognitive deficits that impact memory/recall were not present; immediate negative consequences [eg, added procedures, reprimands, and so on] of reporting nonadherence were absent; the scale used to measure adherence was reliable and valid, culturally sensitive, and worded clearly; patients knew how to respond to the scaling response options with little difficulty; and social desirability bias was minimized).
Method
Materials
Patients completed a number of instruments in this study pertaining to demography, sexual behavior, ART adherence, depression, and posttraumatic stress disorder. Scales that were not available in Spanish were translated and piloted in a group of patients from the same hospital in which the study was conducted. Paper-and-pencil surveys were completed with reading assistance provided as needed.
The sociodemographic scale included questions regarding age, date of diagnosis, gender, marital status, housing, schooling, employment status, income, and substance consumption.
Adherence to ART
An interviewer-delivered Spanish version of the 3-day Adult AIDS Clinical Trials Group (AACTG) 21 was used. CD4 counts (continuous variable) and viral load (a dichotomous variable of “undetectable” or “detectable” was created with participants being classified as undetectable if their viral load was below 400 copies/mL and detectable if it was at least 400 copies/mL dichotomus variable) were extracted from patient’s medical record. Information, motivation, and behavioral skills were measured using LW-IMB-AAQ. 22 This scale includes 9 items regarding information about the regimen, correct ART utilization, medications’ side effects, drug interactions and heuristics, and implicit theories concerning adherence scored as 3 for correct, 2 for unsure, or 1 for incorrect. Total scores could range from 9 to 27 points. Ten motivation items (attitudes and beliefs about outcome of adherent and nonadherent behaviors, evaluation of these outcomes, and perceptions of significant others support for adherence and motivation to comply significant others’ wishes) used a 0 to 4 Likert-type (very hard to very easy) response scale. Total scores ranged from 0 to 40 points. Finally, the behavioral skills items represented objective and perceived abilities for acquiring, self-cueing, and self-administering ART, incorporating the regimen into the ecology of daily life, minimizing side effects, updating ART-related facts as necessary, acquiring social support and instrumental support for adherence, and self-reinforcing over time. Participants used a 0 to 4 Likert-type scale (totally agree to totally disagree) to answer the items. Total scores ranged from 0 to 56 points.
Design and Procedure
This cross-sectional study was conducted in a local public hospital near Mexico City. Between November 2009 and August 2010, a total of 109 patients enrolled into the study. All participants were recruited at 1 site. One of the authors invited patients who attended their monthly checkup visits at an HIV/AIDS clinic to participate in a study about adherence behaviors. After receiving an explanation of the purposes of the study, the confidentiality of the collected data, and that participation would not have an impact on the care that the patient received, all patients approached agreed to participate. The interviewer was not affiliated to the care patients received at clinic. Survey completion averaged about 40 minutes. Procedures were approved by the Hospital’s Department of Education and Research.
Statistical Analysis
Data analysis was conducted using SPSS version 17 (SPSS Inc, Chicago, Illinois). In preparation for main data analyses, scale distributions and characteristics were examined. Specific to the LW-IMB-AAQ, reliability and factor structures were examined via factor analysis with varimax rotation to explore factor structure. Scales for information, motivation, and behavioral skills were established and examined for cross-sectional association with self-reported adherence defined as schedule adherence, and last time when a dose was missed in the past 3 months (both continuous variables) as well as past 3 days’ adherence, past weekend adherence being dichotomous variables. We did not find a normal distribution of the data. Bivariate analyses were used to investigate associations between outcomes of ART adherence and IMB model variables. Associations were significant at P < .05. A significant relationship was found neither between socioeconomic variables and self-reported measures of adherence nor with IMB model variables.
Results
Participants
A total of 109 adult patients, 63% men and 37% women, aged from 18 to 69 years old participated in this study (mean 37.67, standard deviation [SD] 10.97). Inclusion criteria are (1) provision of informed consent, (2) able to read and write Spanish, (3) receiving ARV treatment, (4) ≥18 years old, and (5) agreement to have CD4 count and viral load test results collected from their medical records. Authors did not obtain data related to disease state of the participants. No monetary reimbursement for participation was provided to recruited participants. Current treatment of the participants included monthly checkup visits at the hospital, which included clinical examination, medication review and potential adjustment, and potentially medication pickup. Additionally, every 3 months laboratory tests for CD4 count and viral load were repeated. In contrast to systems of clinic care that allow for 3- or 6-month intervals between clinical care visits, this standard of care is intensive. The insurance source of the sample source was the Seguro Popular via the Servicios de Atención Integral, which are located on Hospitals of the Mexican Department of Health (Secretaría de Salud).
Sample Characteristics and Adherence levels
Seventy-one percent of the patients reported living with their families, 62% reported having children, most of the patients had either elementary and/or middle high studies (62%), and 58 reported a monthly income (calculated in U.S. dollars) of US$125 to US$150. Twenty-six percent of the participants defined themselves as men who had sex with men (MSM), while 74% described themselves as heterosexual. Descriptive statistics of the study sample are reported on Table 1.
Demographic Characteristics of the Participants.

Time since HIV diagnosis on patients from this sample ranged from 1 to 173 months (mean 66.66 months, SD 40.96). The average number of pills in one’s daily ART regimen was 2.40 per day (range 1-4 pills, with 60% taking 2 pills per day). Median of CD4 counts was 555, and 87% of the patients had undetectable viral loads. The ART mostly used by this sample was tenofovir (TDF)/emtricitabine. A third agent was used by some patients, efavirenz (EFV) being the most common. No data were obtained regarding the duration of treatment. Using self-reported adherence measures, 43% of the sample reported following scheduling instructions “most of the time” and 40% of the sample “all the time.” Seventy-six percent of the sample answered that they did not forget taking medications on the last weekend. Regarding adherence on the last month, 46% of the sample reported that they “never missed taking their medication,” while 18% did it “more than 3 months ago.” Schedule adherence was associated with viral load; however, other measures did not associate significantly with cross-sectionally assessed self-reported adherence.
Variables of the IMB Model of ART Adherence
Results show that psychometrical characteristics of the LW-IMB-AAQ Spanish version were good. The information scale showed an internal consistency of α = .538. Factors obtained for the motivation and behavioral skills were similar to those identified with the original LW-IMB-AAQ sample, and coefficients were high and significant in all the cases. Motivation items comprised personal and social motivation to adhere to one’s regime, and the scale showed a Cronbach α (estimate of the reliability of a psychometric test) internal consistency of .759. Items from the behavioral skills scale showed α = .784.
The mean knowledge score of the information component of the LW-IMB-AAQ for this sample was of 23.06 on a scale of 0 to 36, SD 3.065. This score was measured as a continuous variable. Mean motivation score for this sample was 26.36, on a scale of 0 to 40, SD 9.330. Mean behavioral skills score on the whole sample was 40.96, on a scale of 0 to 56, SD 11.080.
Correlates of adherence
No associations were found between total information scale and adherence outcomes. Motivation total scale, as predicted, showed significant associations with behavioral skills total scale (r = .417, P = .000) but not with information or self-informed measures of adherence. Behavioral skills total scale was directly associated with 2 self-informed adherence measures: adherence on the last weekend (r = .272, P = .005) and last time a dose was missed in the past 3 months (r = .196, P = .043). Also, we found that adherence in the last 3 months was correlated with adherence during the last weekend (r = .329, P = .001) and adherence to schedule (r = .398; P = .000). No associations were found between viral load and CD4 counts and self-reported adherence (see Table 2).
Pearson Correlations among Variables of the IMB Model of ART.
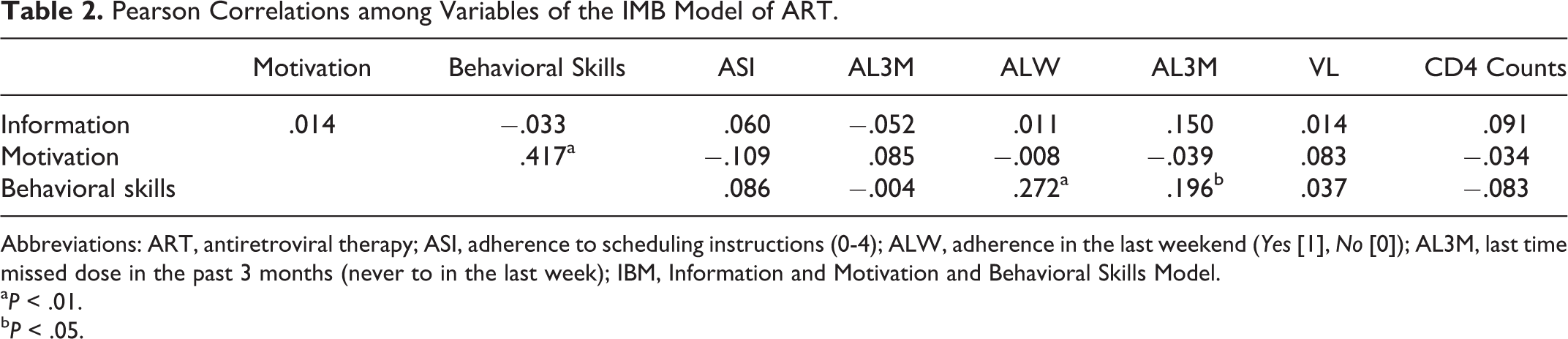
Abbreviations: ART, antiretroviral therapy; ASI, adherence to scheduling instructions (0-4); ALW, adherence in the last weekend (Yes [1], No [0]); AL3M, last time missed dose in the past 3 months (never to in the last week); IBM, Information and Motivation and Behavioral Skills Model.
a P < .01.
b P < .05.
To provide guidance for targeting of future intervention content, we examined the specific items from the behavioral skills measure that associated with adherence outcomes. Two items from the behavioral skills scale were significantly associated with the following scheduling instructions: (B4) “How hard or easy is it for you to get your HIV medication refills on time?” (r = .207; P < .032) and (B8) “How hard or easy is it for you to take your HIV medications because the pills are hard to swallow, taste bad, or make you sick to your stomach?” (r = .194; P < .044). Five items from the behavioral skills scale showed to be significantly associated with adherence on the last weekend: (B2) “How hard or easy is it for you to stay informed about HIV treatment?” (r = .349, P < .000); (B6) “How hard or easy is it for you to manage the side effects of your HIV medications?” (r = .204, P < .037); (B8) “How hard or easy is it for you to take your HIV medications because the pills are hard to swallow, taste bad, or make you sick to your stomach?” (r = .212, P < .030); (B11) “How hard or easy is it for you to take your HIV medications when you do not feel good emotionally (eg, when you are depressed, sad, angry, or stressed out)?” (r = .302 P < .002); and (B14) “How hard or easy is it for you to talk to your health care provider about your HIV medications?” (r = .359, P < .000). Self-reported adherence on the last weekend was not associated with CD4 counts but was associated with adherence on the last 3 months (r = .329, P < .001). Finally, we found associations between self-reported adherence on the last 3 months with 1 item of the information scale: “I know what to do if I miss a dose of any of my HIV medications (eg, whether or not to take the pill(s) later)” (r = .208, P < .032) and 4 items of the behavioral skills scale: (B2) “How hard or easy is it for you to stay informed about HIV treatment?” (r = .290, P < .002); (B6) “How hard or easy is it for you to manage the side effects of your HIV medications?” (r = .196; P < .042); (B13) “How hard or easy is it for you to take your HIV medications when you do NOT feel good physically?” (r = .221, P < .022); and (B14) “How hard or easy is it for you to talk to your health care provider about your HIV medications?” (r = .256, P < .007; Tables 3 and 4).
Spearman Correlations between Behavioral Skills Items and Measures of Adherence.

Abbreviations: ASI, adherence to scheduling instructions (0-4); ALW, adherence in the last weekend (Yes [1], No [0]); AL3M, last time missed dose in past 3 months (never to in the last week)
a P < .01.
b P < .05.
Pearson Correlations among Variables of the IMB Model of ART.a

Abbreviations: ART, antiretroviral therapy; IMB, IBM, Information and Motivation and Behavioral Skills Model.
a P < .05.
b P < .01.
Discussion
The present research aimed to describe predictors of adherence in the middle-income country of Mexico, using variables from the IMB Model of ART Adherence. Results showed that items of the behavioral skills scale were associated with self-reported adherence measures and not with CD4 counts or viral loads. Significant but low correlations were found between the 2 behavioral skills items and adherence to scheduling instructions. Adherence on the last weekend was correlated with 5 behavioral skills items, and adherence on the last 3 months was correlated with 4 behavioral skills items. Behavioral skills total scores were correlated with patient’s motivation. Information toward treatment did not show relationship with motivation or adherence behaviors, and these findings are similar to previous research done in the United States. 22 The fact that only behavioral skills items showed correlations with the adherence measures used may suggest that as the IMB model predicts, there is evidence to think that behavioral skills are a critical prerequisite of adherence. Research should be made in order to confirm the influence on behavioral skills that adherence information and adherence motivation have.
As research to evaluate factors associated with adherence to ART in Brazilian HIV-infected patients, 23(p1251) “our study noted both parallels and differences between factors related to adherence compared to those identified in U.S. and European populations.” Several comments were made regarding these findings. (1) This research tested a theoretical-based model which has shown to be effective in explaining adherence behaviors. This model, though, is in a process of being evaluated in particular populations such as the one included on this research, with particular sociodemographic characteristics such as low income, low levels of education, primarily heterosexual, poor reading and writing abilities, and low substance use, among others. So, in the future, cultural variables could be taken into account, as the population in this study is mainly collectivist, where 70% of the patients reported living with their families. These results resemble that obtained in Thailand through a qualitative study on Thai population, 24 applying the IMB Model of ART Adherence. These findings suggest that some modifications to the model could be made in cultural settings with more collectivistic worldviews, particularly in the motivation variable. (2) Patients from this population showed to be highly adherent, with 87% of the population having undetectable viral loads. This information confirms that populations in resource-limited settings can be as adherent, if not more adherent, as populations in countries with easier access to ART medication and medical services. Other research conducted in South Africa 25 shows this tendency. Finally, (3) taking into account the data obtained in this investigation, there is still inconsistency in establishing whether the characteristics of participants are associated with self-reported adherence. Our study found that adherence was not related to demographic variables, similar to other findings, 26 in which ethnicity, gender, and age were related to adherence, and also we did not find any relationship between self-reported adherence and variables such as poor psychological well-being, having relatives to remind the patient to take therapy, or having children unlike other studies that have found such relationships. 27
Contrary to expectations, information showed no correlation with motivation or self-reported measures of adherence. Results from this research are similar to other findings, 28 which suggest that treatment information may not differentiate between adherent and nonadherent patients. Although information was generally high, in this study, it seems that being well informed is not as important for taking medication on the last week as being well skilled for doing so.
Two possible explanations could explain the lack of association between information and the other variables of the model. Information included in the instrument used in this research may not have included the kinds of information content that would be most influential in this population. Elicitation research, as suggested by other authors, 29 could examine the kinds of information toward treatment that would be most influential. Alternatively, the information content included may have been appropriate but because some items asked participants to rate their sense of being informed (eg, I know what the possible side effects of each of my HIV medications are), rather than testing for actual knowledge, the scale may more accurately reflect one’s perceived, versus actual, fund of information. It may be that perceived knowledge has less of an association with adherence-related behavioral skills than actual knowledge. However, we do note that other studies have used similar items and did demonstrate a relationship between information and behavioral skills. Our study, however, did not find a relation between information and either behavioral skills or adherence within our targeted sample.
The critical role of behavioral skills found in our results is similar to previous research in PLWH in Mexico, where the only predictor of adherence behaviors was the perceived difficulty in doing the behavior. 30 In our work, motivation was associated with behavioral skills and behavioral skills with adherence behaviors. Motivation, which includes both personal beliefs and beliefs about support from important others, positively associated with behavioral skills. Behavioral skills, which include use of adherence promotion strategies in diverse situations and one’s overall sense of efficacy in doing so related to self-reported measures of adherence.
In moving from model evaluation to the development of targeted intervention approaches, the current results suggest that both motivation and behavioral skills should receive specific attention. Joined with other theories of critical drivers of ART adherence (eg, Psychological Model of Biological Health 31 ), skills building to leverage strategies successfully implemented in the patient’s past history (eg, with other regimens or for other conditions) may be an efficient strengths-building approach. Past experiences with following schedules, using cues, and organizing the environment to facilitate pill taking likely will strongly influence the future use of such skills-sets. In terms of motivation, addressing social motivation in terms of patient–provider communication, relationship, and trust 32 may further contextualize adherence within important social and structural systems. Multiple studies have used the IMB model to direct intervention content. 33 For the population we targeted, similar approaches to promoting motivation and skills may be beneficial.
Results of the current study should be considered within the context of several limitations. Although all the participants who were invited agreed to participate, the study may have a selection bias. Participants in this study were the ones who routinely attended to their medical appointments. Replication of findings with samples that have greater variability in viral load, rates of adherence, and rates of HIV care use is needed. A second limitation concerns instrumentation. The measures for this study were intended to be self-administered. Early in the data collection process, reading and writing limitations in the sample required revision to data collection to allow for direct assistance in reading and marking responses for some participants. This could have resulted in participants generating social desirable answers. Additionally, while support for a significant association between following of regimen requirements and viral load was evidenced, we did not find significant associations with our other measures of adherence and viral load or CD4 counts. This is likely because of the limited variability in these biological measures in this sample and the cross-sectional assessment of factors that have known temporal relationships (nonadherence precedes viral failure). Also, this research did not include previous elicitation work regarding the scales items, and we used a tool developed in the United States for translation and use in Mexico. In the future, this could be added with the purpose of better understanding Mexican patients’ adherence to ART. Finally, the population of this study does not represent the HIV/AIDS epidemiological panorama in Mexico, which includes mainly MSM.
Despite the limitations noted, the current work suggests that the IMB model characterized adherence within this sample well, with the exception of the information construct. Motivation and skills were critical and intervention approaches that target these appear appropriate. Future research should target the identification of effective methods for enhancing personal and social motivation and skills that are culturally competent and sensitive to the unique context of living with HIV in Mexico.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.