
Abstract
Background:
The Indian Health Service (IHS), a federal agency, provides direct patient care to an estimated 1.9 million American Indian/Alaska Native patients across a large and decentralized network of health facilities. The IHS sought to implement HIV screening of adults and adolescents per national recommendations. The IHS facilities received technical support such as electronic clinical reminders (ECRs) and sample HIV-testing policies.
Purpose:
To determine what facility-wide policy and practices were associated with high HIV screening rates.
Methods:
Survey of clinical directors of 61 federal health facilities on use of ECRs, testing policies/standing orders, and other factors associated with HIV screening. These results were correlated with HIV screening performance results for each facility as derived from the IHS national database.
Results:
A total of 51 (84%) of 61 facilities were interviewed. In univariate analysis, factors that were correlated with higher rates of HIV screening were having an HIV screening standing order (unadjusted odds ratio [UOR] 8.7, 95% confidence interval [CI] 2.0-37.3), sexually transmitted disease (STD) screening standing order (UOR 5, CI 1.1-21.7), having an HIV ECR in place for a year or longer (UOR 10.2, CI 2.8-37.5), and inclusion of both providers and nurses in offering HIV screening (UOR 4.8, CI 1.4-16.7). In multivariate analysis, ECRs (adjusted odds ratio [AOR] 9.1, 95% CI 1.8-45.1) and STD standing orders (AOR 7.4, 95% CI 1.1-51.0) remained significantly associated with higher HIV screening.
Conclusion:
Policy and practice interventions such as ECRs and standing order/testing policies and delegation of screening are correlated with high HIV screening, are scalable across health networks, and will be used for improving other infectious disease screening indicators in such as STD and hepatitis C.
Keywords
Background
American Indian/Alaska Native (AI/AN) patients have among the fastest progression of AIDS diagnosis to death of any race/ethnicity. 1 In addition, this population has a significantly elevated death rate due to HIV/AIDS compared to whites, 2 making early detection of HIV and linkage to care a priority.
The Centers of Disease Control and Prevention (CDC) and the US Preventive Services Task Force (USPSTF) recommend 1-time HIV screening for adult and adolescents, augmenting existing screening recommendations of prenatal women and risk-based testing. 3 Studies have documented numerous barriers to HIV screening, including time constraints, competing priorities, and low perceived risk of HIV infection. 4 –6
The US Indian Health Service (IHS) is an agency within the Department of Health and Human Services responsible for providing federal health care to AI/AN people. The IHS provides health care to 566 federally recognized tribes in 34 states and serves a user population of 1.9 million. The majority of IHS health facilities are primary care clinics based in remote rural settings.
The IHS National HIV/AIDS program notified facilities of the new HIV screening recommendations in 2006 and offered technical support on an ongoing basis to implement expanded screening. Support centered on 2 central intervention options to be used at the discretion of the health facility, namely, (1) assistance deploying an electronic clinical reminder (ECR) and (2) a customizable template for facility testing policy. However, IHS is highly decentralized, and the prioritization and mode of implementation of HIV screening are largely a local decision.
Electronic clinical reminders have shown success in preventive care, including HIV screening. 7 –14 The ECRs have mixed results for some screening interventions. Barriers to successful ECRs include poor usability, time constraints, and work flow disruption. 15 –19 All federal IHS sites use the same electronic health record (EHR), allowing the ECRs to be deployed in any facility with minimal or no local modifications.
Methods
Program evaluation used 2 separate methods, that is, a national database to track screening rates by facility and a facility-based survey to document policy, practice, and other factors that were correlated with high performance.
Since 2012, IHS has monitored a cumulative national HIV screening measure defined as unique patients aged 13 to 64 having a history of an HIV test or “HIV Ever Screened,” with a nationally standardized definition.
To determine factors associated with higher performance in HIV Ever screening, IHS conducted a facility-based survey. From August to December 2013, all federal IHS facilities with an active clinical population of over 1000 persons were surveyed. The survey instrument was pilot tested and modified as needed for clarity and conciseness. The questionnaire included facility-wide variables expected to be correlated with expanded HIV screening rates. These factors included the use of the HIV ECRs, use of standing orders, clinician type ordering HIV tests, and human resources (nurse and provider vacancy estimates). For standing orders, expanded HIV and sexually transmitted disease (STD) screening policy was defined as any testing protocol that was more inclusive than screening prenatal patients.
Each facility’s clinical director was sent up to 3 e-mails to set up a time to complete the survey by phone interview. The clinical director could include or delegate the interview to others suitable to answer policy and practice questions on behalf of the facility.
National screening data are passively collected and aggregated 3 times a year onto a national database on the IHS health information platform, the resource and patient management system. HIV Ever Screened is embedded within a larger set of nationally reported preventive care indicators in IHS.
Survey response data were entered and analyzed using Predictive Analytics SoftWare (PASW) (v19, Chicago, Illinois, www.spss.com). A high rate of HIV screening was defined as 35% or higher, representing the top 2 quintiles of the facilities. Bivariate correlates of having an Ever Screened proportion of
Results
We surveyed 51 of 61 eligible federal sites, for a response rate of 84%. The sites had a median active clinical population of 13- to 64-year-olds of 5741 persons (range 1140-48 635). All sites had been using EHR for at least 4 years, and 47 (92.2%) of 51 used an ECR of some type. Of the sites that used an ECR, 12 (25.5%) said the clinicians used reminders consistently, while 35 (74.5%) said their usage varied widely by clinician. Of the 51 sites, 32 (62.7%) had deployed the national IHS HIV ECRs for screening of persons 13 to 64 years of age, and 21 (41.2%) had the ECRs in place for a year or longer.
Fourteen (27.5%) sites had standing orders for expanded HIV screening and 11 (21.6%) had standing orders for STD screening (chlamydia, gonorrhea, and syphilis). In 22 (43.1%) sites, providers (physician, nurse practitioner, and physician assistant) usually ordered HIV tests, and nurses usually ordered tests in 8 (15.7%) and both providers and nurses ordered HIV tests in 21 (41.2%) sites. For respondent estimates on human resource constraints, 22 (44.9%) of the 49 sites had a provider vacancy rate >20% at the time of survey. For nurse vacancies, 7 (17.5%) of 40 estimated the vacancy rate at >20%. Nearly all sites, 48 (96%) of 50, had a clinical applications coordinator (CAC; or medical informaticist), and 26 (52%) of 50 had a full-time CAC for a year or longer.
In univariate analysis, factors that were correlated with higher rates of HIV screening were having an HIV standing order, an STD standing order, an HIV ECR in place for 1 year or longer, and inclusion of both providers and nurses in offering HIV screening (Table 1). In multivariable analysis controlling for having HIV and STD standing orders in place, having an ECR in place for >1 year, and HIV screening performed by staff other than physicians, the ECRs (adjusted odds ratio [AOR] 9.1, 95% confidence interval [CI] 1.8-45.1) and the STD standing orders (AOR 7.4, 95% CI 1.1-51.0) remained significantly associated with >35% HIV screening coverage.
Policy, Practice, and Human Resource Variables by HIV Ever Screened Rates among 13- to 64-Year-Olds, IHS Federal Facilities.a
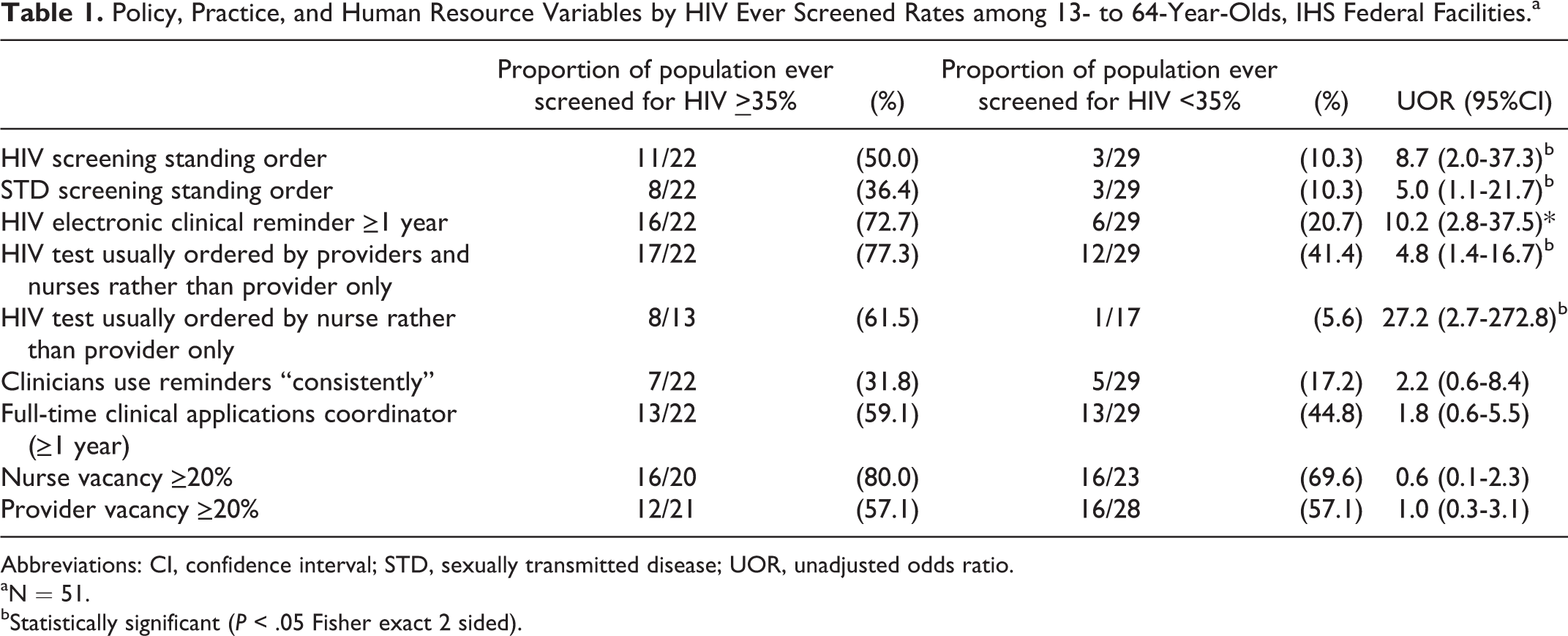
Abbreviations: CI, confidence interval; STD, sexually transmitted disease; UOR, unadjusted odds ratio.
aN = 51.
bStatistically significant (P < .05 Fisher exact 2 sided).
Lower vacancy rates of providers or nurses at the time of survey did not have a significant association with higher screening rates, nor did having a CAC full time for a year or longer.
Conclusion
Standing orders (both HIV and STD based), inclusion of nurses in ordering HIV screening, and use of ECRs >1 year were all correlated with high HIV screening rates. These policy and practice interventions may help compensate for other challenges such as human resource and time constraints. These interventions streamline and facilitate both the identification of which patients are due for screening and the ordering of the appropriate test prior to or during the patient visit.
Greater inclusion and responsibility for nurses in preventive care through standing orders and protocols have been identified as an important tool to decrease the burden on providers. 21 –24 In IHS, delegation of HIV and other screening measures are essential in maximizing the care in each medical visit. The lack of correlation of a CAC with higher HIV screening rates was unexpected, as CACs are integral in deploying clinical reminders and monitoring local data. However, some sites with no CAC are able to get regional or national support remotely for tasks such as deploying ECRs and generating screening data updates.
There are limitations to this project. All facilities were offered support for HIV screening as a standard of care, which precludes a control group and allows only for observing correlates of high HIV screening. Persons completing the survey may have had incomplete knowledge of provider-level practices. In addition, answering on behalf of the health facility necessitated estimates or recall by the interviewee, which may result in some bias. Despite the high response rate (84%), our sample size was small, limiting our ability to show statistical significance for some variables that were probable contributors to higher screening rates.
Although routine, 1-time HIV screening of persons aged 13 to 64 is an essential part of the IHS response to HIV/AIDS. Clinicians will need to continue to pursue risk-based testing to ensure that patients with HIV/AIDS are diagnosed and linked to care as soon as possible to reduce outcome disparities in HIV/AIDS outcomes in AI/AN people.
The policy and practices that are correlated with higher HIV screening are scalable across IHS and can be applied to other screening measures. The ECRs, standing orders, and in services are offered to facilities that want to target similar nationally recommended screenings such as annual chlamydia screening among young women 25,26 and hepatitis C screening among persons born from 1945 to 1965. 27,28 This multicomponent sharing of best practices can be effective across a health network. 29 Special attention may be needed for tribal sites that have migrated to private sector EHR platforms, as electronic reminders may require extensive customization and expense.
Footnotes
Authors’ Note
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention or the Indian Health Service.
Acknowledgements
The authors would like to thank the CA and Rockville GPRA offices of IHS and Dr Thomas Sequist.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.