
Abstract
Objective:
To estimate trends in hospitalizations and days of care of HIV-infected individuals in US hospitals from 1982 to 2010.
Methods:
Secondary data analysis of the National Hospital Discharge Survey.
Results:
Hospitalizations of HIV-infected individuals increased from 1982 to a peak of 216 086 by 1995, fell 36% by 1997, and then decreased to 118 236 by 2010. Days of care for HIV-uninfected individuals decreased 14.7% from 6.1 days in 1982 to 5.2 days in 2010 yet dropped 62.7% from 17.6 to 7.1 days for HIV-infected individuals. Hospitalized HIV-infected individuals were more likely than uninfected individuals to be male, black, 35 to 44 years old, Medicaid recipients, and be hospitalized in the northeast, in hospitals with more than 500 beds and in government-operated hospitals.
Conclusions:
Hospitalizations and days of care for HIV-infected individuals have decreased dramatically in recent years and at rates greater than for HIV-uninfected individuals yet involve some populations and affect certain hospitals disproportionately.
Introduction
Since the first AIDS case was reported in 1981, 1 there have been many human rights, medical, psychological, social, and other improvements in HIV/AIDS care, services, and treatment which have greatly reduced the morbidity and mortality 2 of HIV/AIDS in the US. Over time, the number of people in the US known to be living with HIV has increased, 3 probably because of these improvements and a growing emphasis to identify and bring to care all those who are infected. 4,5 It is likely that improvements in HIV/AIDS care and prevention, increased HIV prevalence, and a drive to identify infections have and will continue to impact hospitalizations in the US.
From a US public health and policy-making perspective, it is crucial to understand trends in hospitalizations, days of care, and hospitalization payment sources for HIV-infected individuals at a national level, particularly in light of advances over the past 33 years and a growing HIV-infected population in the US. This information might assist health agencies in anticipating needs for future treatment services. Although previous studies of HIV/AIDS hospitalizations have been enlightening, their data are not current or have limited scope, for example, they focused on particular groups of patients (pregnant women, patients age ≥45 years), a single city or state, selected hospitals, or specific years. 6 –13 Moreover, given how HIV/AIDS disproportionately affects racial and ethnic minorities in the US, 3,14 –17 it is also essential to ascertain how hospitalizations, days of care, and hospitalization payment sources vary by patient demographic characteristics and across hospitals. Such data would help us to understand how to prioritize resources in the US and identify potential disparities in care.
This report examines hospitalizations of HIV-infected individuals from 1982 to 2010 in US short-stay hospitals. The report includes data from the National Hospital Discharge Survey (NHDS), which is a national probability sample survey conducted by the National Center for Health Statistics for the Centers for Disease Control and Prevention (CDC). 18 The objectives of this study were to (1) estimate hospitalizations of HIV-infected individuals in US short-stay hospitals from 1982 to 2010, (2) evaluate trends in days of care and source of payment among hospitalized HIV-infected persons during this period, (3) compare hospitalizations for HIV-infected individuals versus individuals with no HIV infection by patient demographic characteristics and hospital characteristics, and (4) compare these characteristics by days of care and payment source for hospitalized HIV-infected individuals.
Methods
Study Design
The 1982 to 2010 NHDS is a national probability sample survey that reports hospitalizations according to medical conditions, demographic characteristics, and other features. 18 NHDS utilizes a 3-stage sampling design, which involves probability samples of primary sampling units (PSUs) from the National Health Interview Survey sample (stage I), short-stay nonfederal hospitals (whose mean days of care is less than 30 days) within PSUs (stage II), and a sample of discharges within hospitals (stage III). The NHDS collects data from approximately 270 000 sampled hospitalizations each year from more than 400 responding hospitals in the 50 states and the District of Columbia. This sample is then properly weighted according to the sampling design to obtain national estimates. NHDS data are recorded and referred to a hospitalization level, instead of an individual or person level. Hence, this article uses hospitalizations as the reported event of interest and unit of analysis. Hospitalizations of HIV-infected individuals were identified by the first 7 diagnosis codes for each visit, using the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM codes: 042, 042.0-0.42.2, 042.9, 043.0-043.3, 043.9, 044.0, 044.9, and 279.19).
Data Analysis
Hospitalizations of HIV-infected individuals were expressed as a function of 100 total hospitalizations (hospitalizations of HIV-infected plus individuals with no HIV infection) per year along with corresponding 95% confidence intervals (CIs). To characterize trends of hospitalized HIV-infected individuals over time, a piecewise linear regression model was fit for the data; 4 pieces that depicted obvious changes in trends were estimated. A similar regression model was fit for hospitalized HIV-uninfected individuals. Corresponding relative differences in hospitalizations over time were calculated.
Mean days of care and their 95% CIs were computed for hospitalizations for HIV-infected and -uninfected individuals over time. Unadjusted differences in mean days of care between these hospitalizations across all study years were compared using t tests. Multivariable linear regression models of days of care, adjusting for patient demographic and hospital characteristics, were then fit to estimate the adjusted differences in mean days of care.
Payment source proportions and corresponding 95% CIs were estimated across all study years. Unadjusted relative differences in proportions between hospitalizations for HIV-infected and HIV-uninfected individuals over time were calculated. Adjusted differences in payment source proportions between hospitalizations for HIV-infected and HIV-uninfected individuals in 2010 were calculated based on the results of multivariable linear regression models.
Mean age for hospitalizations was estimated for each year of the study (medians cannot be estimated with NHDS data). Linear regression models were created to estimate trends in mean age over time. Median age of the US population over the study period was obtained for comparison purposes from US Census data (www.census.gov). All other patient demographic and hospital characteristics, stratified by HIV/AIDS status, were summarized for the entire study period and compared using 2 sample t tests or Pearson chi-square tests, as appropriate. Univariable and multivariable logistic regression analyses were performed to compare hospitalizations for HIV-infected versus HIV-uninfected persons by demographic and hospital characteristics across all years and for representative years. These representative years corresponded to milestone changes in HIV/AIDS antiretroviral therapy (ART)—1987 (zidovudine [ZDV]), 1995 (protease inhibitors [PIs]), and 2006 (once-a-day treatment combination pill and widespread use of combination therapy)—and the most recent year of HIV/AIDS data in NHDS (2010). Odds ratios with corresponding 95% CIs were estimated.
Hospitalizations for HIV-infected individuals out of all hospitalizations, days of care, and payment source were plotted by demographic and hospital characteristics along with corresponding 95% CIs for each survey year (eg, hospitalizations for HIV-infected males of all male hospitalizations). Differences in hospitalizations, days of care, and payment source by each demographic and hospital characteristic were estimated. For demographic and hospital characteristics with multiple categories (eg, expected payment source), differences were estimated between the category with the highest proportion of hospitalizations versus all other categories. Corresponding 95% CIs of the differences were calculated assuming independence among hospitalizations. t Tests were used to compare selected groups by demographic and hospital characteristics.
All analyses were adjusted for the multistage sampling design of the surveys weighting scheme, where the weights were reciprocals of the probabilities of the sample, of the sample, with adjustment for nonresponse and population weighting ratios. 19 All data were analyzed using SAS 9.3 (SAS Institute Inc, Cary, North Carolina, USA) and STATA11 (STATA Corporation, College Station, Texas, USA). The α = .05 level of significance was used for all comparisons.
Results
Hospitalizations of HIV-Infected Individuals
Of the estimated 1079 million hospitalizations in the NHDS database from 1982 to 2010, 0.3% were HIV-infected individuals and 99.7% were of HIV-uninfected individuals. Hospitalizations of HIV-uninfected individuals decreased from 42.5 to 34.1 million from 1982 to 1988, remained steady around 34 million from 1988 to 1997, and then increased to 38.8 million from 1997 to 2010 (Figure 1). Hospitalizations of HIV-infected individuals increased rapidly from 1982 to a peak in 1995 (216 086), fell sharply by 1997, and then decreased steadily through 2010 (118 236). Per the results of the piecewise linear regression model, there was on average a 4.27% increase in hospitalizations of HIV-infected individuals each year before 1995. After 1995, on average there has been a 1.32% decrease in hospitalizations of HIV-infected individuals each year.
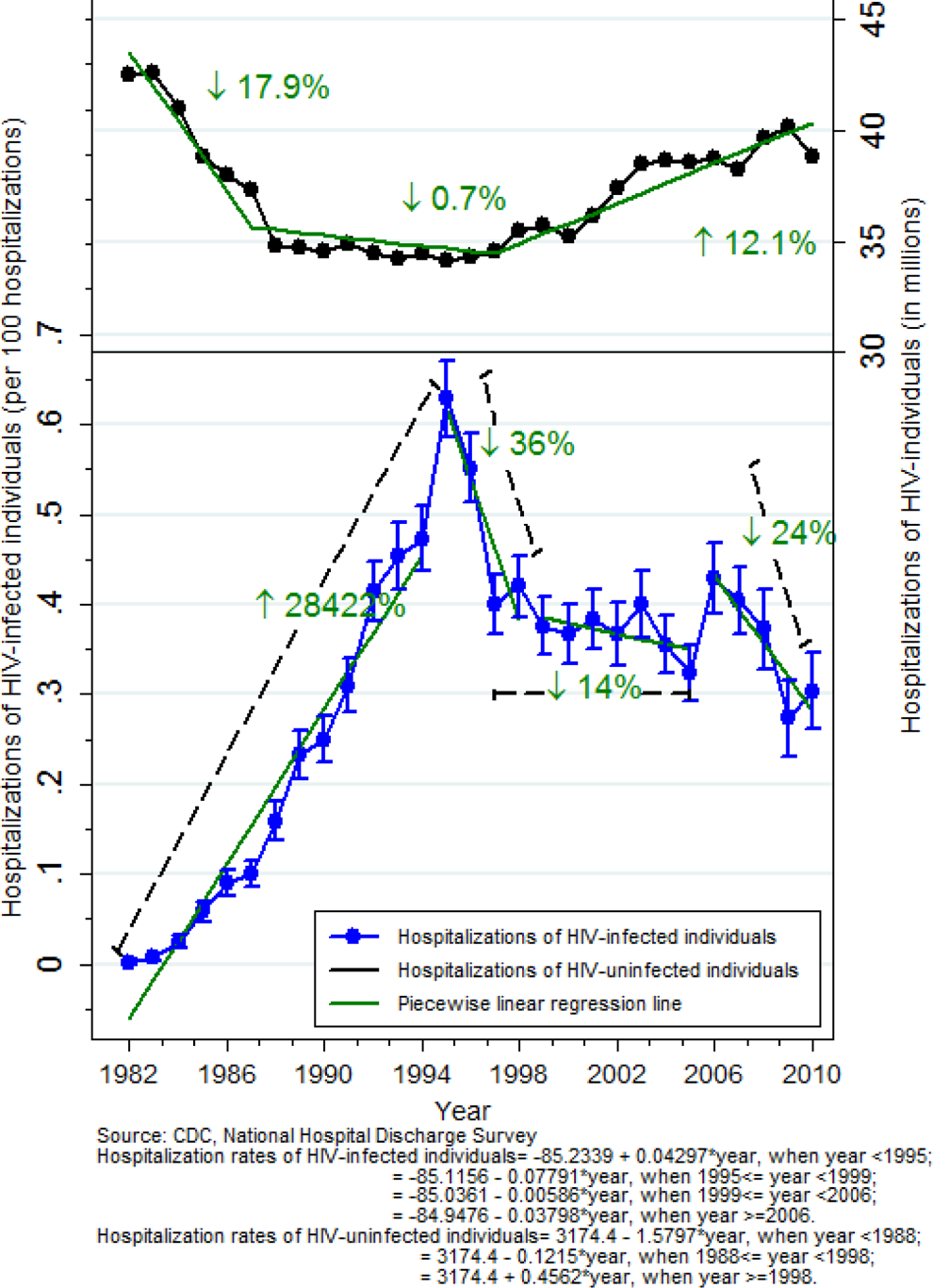
Hospitalizations of HIV-infected and HIV-uninfected individuals, US, 1982 to 2010.
Hospitalization Days of Care
Mean days of care for hospitalized HIV-uninfected individuals decreased from 6.1 days in 1982 to 5.2 days in 2010, while mean days of care for hospitalized HIV-infected individuals dropped rapidly from 17.6 to 6.6 days during the period (P < .02 for the change between hospitalizations for HIV-infected and HIV-uninfected individuals; Figure 2). After adjusting for patient demographic and hospital characteristics, days of care for hospitalized HIV-infected individuals decreased 62.7% from 1982 to 2010, while hospitalizations for HIV-uninfected individuals decreased 14.7%. The adjusted differences in days of care between hospitalizations for HIV-infected and HIV-uninfected individuals were Δ11.4 days in 1982, Δ8.4 days in 1987, Δ4.2 days in 1995, Δ3.1 days in 2006, and Δ1.4 days in 2010.

Estimated days of care among hospitalized HIV-infected and HIV-uninfected individuals, US, 1982 to 2010.
Hospitalization Payment Source
Figure 3 depicts changes in payment source for hospitalizations over time. As shown, private health care insurance was the predominant payment source in the early years of the US HIV epidemic; but by 2010 it accounted only for 8.5% of hospitalized HIV-infected individuals (a 86.1% relative decrease since 1984), while Medicare, Medicaid, and self-pay accounted for 35.0%, 36.4%, and 21.3%, respectively, of payment sources in 2010. Among hospitalizations for HIV-uninfected individuals, there have been steady relative increases in Medicare (37.6%), Medicaid (113.7%), and self-pay (103.1%) as payment sources from 1982 to 2010, with a concomitant precipitous drop in private health care insurance as a payment source (67.3%). After adjusting for patient demographic and hospital characteristics, the differences in payment source between hospitalizations for HIV-infected and HIV-uninfected individuals in 2010 were private health care (Δ8.5%), Medicare (Δ1.3%), Medicaid (Δ18.3%), and self-pay (Δ2.0%).

Estimated hospitalizations of HIV-infected and HIV-uninfected individuals by payment source, US, 1982 to 2010.
Differences by Patient Demographic and Hospital Characteristics
Mean age has increased at a relatively faster rate from 1982 to 2010 among HIV-infected (relative increase 40.8%) than HIV-uninfected hospitalized individuals (relative increase 17.2%; P < .01; Figure 4). Mean age among HIV-uninfected hospitalized individuals remains greater than HIV-infected individuals (48.8 versus 45.9 years in 2010, Δ2.9 years; P < .01), but the gap has narrowed substantially since 1982 (41.7 versus 32.6 years, Δ9.1 years; P < .01). In comparison, per the US Census, the median age in the US population has also increased, yet at a slower (22.0%) rate than among hospitalized HIV-infected individuals (30.5 years in 1982 versus 37.2 years in 2010; Δ6.7 years).

Estimated mean age among hospitalized HIV-infected and HIV-uninfected individuals, US Census median age, US, 1982 to 2010.
Across all years of the study, hospitalizations of HIV-infected versus HIV-uninfected individuals were more likely to involve males, Medicaid as the payer source, hospitalizations in the northeast, hospitals whose bed size is more than 500, and hospitals operated by nonprofit organizations and government agencies (Supplemental Tables 1-3). Several changes in hospitalized HIV-infected individuals over time are noteworthy (Figure 5 and Supplemental Figure 1). Although males predominated among hospitalized HIV-infected individuals, the gender gap had narrowed by 2010 to Δ = 3.5% (males > females), when hospitalizations of HIV-infected individuals were 3.2 times greater among males than females. By 2010, the gap among hospitalized HIV-infected individuals between survivors and decedents had narrowed substantially (Δ0.5%). Hospitalizations of HIV-infected individuals were similar among blacks and whites from 1982 to 1985 (P < .26), then increased significantly among blacks from 1986 to 1995 (Δ0.06% to Δ17.0%; P < .01). This difference remained steady from 1996 to 2007 (Δ16.9% to 17.6%; P < .40), then decreased 51% by 2010 (Δ8.7%; P < .01). By 2006, hospitalizations of HIV-infected individuals among government-operated hospitals had increased to a peak of 12.1% but had fallen to 5.2% by 2010.

Estimated hospitalizations of HIV-infected individuals, by demographic and hospital characteristics, US, 1982 to 2010.
Estimated days of care among hospitalized HIV-infected individuals have not differed substantially over time by age-group, gender, race, expected source of payment, region, hospital ownership, or hospital bed size (Supplemental Figures 2 and 3). However, days of care were generally greater for patients who died during their hospitalization versus those who survived, but this difference had narrowed by 2010 (6.9 versus 11.9 days, survivors versus decedents; P < .05).
For payment source among hospitalizations of HIV-infected individuals, Medicaid and Medicare predominated by 2010 for 35- to 44-year-olds, males, and blacks as compared to other demographic groups (Supplemental Figures 4-11). Also by 2010, private health care insurance was slightly greater among males than females, and self-pay/no charge/other was greater among blacks than other race/ethnic groups and slightly greater among males than females.
Discussion
Although hospitalizations of HIV-infected individuals in US short-stay hospitals increased dramatically from 1982 to 1995, they have fallen substantially since then and at rates much greater than for hospitalizations of HIV-uninfected individuals. The reduction in hospitalizations of HIV-infected individuals is likely associated with breakthroughs in antiretroviral (ARV) medications to combat HIV and consequent reductions in AIDS-related mortality, as well as the many other advances in HIV/AIDS care and services, since the total number of people living with HIV infection has increased in the US. It is possible, however, that medical practice changed over time and patients living with HIV/AIDS were less likely to be admitted for a given medical condition, but reductions in HIV/AIDS morbidity and mortality over time support the contention that improvements in treatment have led to reductions in hospitalizations and days of care in hospitals. Of relevance to public health planning, there has been pattern of slow decline in hospitalizations of HIV-infected individuals in recent years, despite more people living in the US with HIV/AIDS and an emphasis on identifying those who are infected.
Average days of care have also declined among hospitalized persons with or without an HIV infection. The decrease among hospitalized HIV-infected individuals is also very likely because of the improved HIV/AIDS care and services and the conditions associated with it. As an alternative explanation, trends toward shorter hospital stays and fewer resources could be because hospitals have reduced days of care for all patients. However, the reduction in days of care among hospitalizations for HIV-infected individuals was greater than for uninfected individuals over the study period. In fact, US hospitals can now anticipate that days of care likely will be similar for patients with and without HIV.
Changes in payment source over time have been relatively similar between hospitalizations for HIV-infected and HIV-uninfected individuals. Private health care insurance has decreased substantially as the predominant payor source. Unfortunately, a significant proportion of hospitalizations have self-pay/no charge/other (which usually reflects no health care insurance). Hospitals can anticipate that Medicare and Medicaid will be the predominant payor source for hospitalized HIV-infected individuals, perhaps even more for Medicare as the HIV-infected population ages and fewer perinatal HIV infections occur.
Despite finding differences within demographic and hospital characteristics in the proportion of hospitalizations that were among HIV-infected versus HIV-uninfected individuals, days of care did not vary according to demographic and hospital characteristics among those with an HIV infection. This distinction probably is due to differences in who is more likely to be hospitalized for HIV/AIDS, which reflects the demographic distribution of those with HIV/AIDS across the US (eg, more likely among males and increasing in prevalence among blacks and Hispanics) and access to medical care. It is reassuring that once an HIV-infected individual is hospitalized, demographic characteristics do not appear to be an important factor in days of care. In fact, days of care only differed by survival status among those hospitalized with HIV/AIDS. It is likely that patients who died during their hospitalization had more serious conditions than those who survived. This finding could be helpful in planning for care among patients living with HIV/AIDS with a poor prognosis than those who survived, which might reflect in some cases a late diagnosis of an HIV infection. Unfortunately, it does appear that lack of insurance predominates among blacks than other racial/ethnic groups, which indicates a disparity regarding ability to pay for these hospitalizations.
To our knowledge, this research is the largest analysis of trends of long-term hospitalizations among HIV-infected individuals for short-stay hospitals in the US. Thus, it fills a critical absence in our knowledge about these hospitalization trends for in the US. However, trends in hospitalizations of HIV-infected individuals require continued monitoring of the epidemic for planning of HIV/AIDS-related services. Because this is predominately an epidemiologic study, future studies regarding these hospitalizations should also examine other potential reasons for differences in hospitalizations that this study could not examine, for example, poor health care services, drug use, socioeconomic status, and disease severity.
There are several limitations to this study. First, data collected in the NHDS are not population based, so that the estimates from this study might not be completely representative of all hospitalizations in the US from 1982 to 2010. Moreover, hospitals with average days of care of more than 30 days for all patients are excluded in the NHDS as well as hospitalizations at federal, military, and Veterans’ Administration hospitals and hospitals with fewer than 6 beds. 18 Second, data from the NHDS cannot be used to estimate incidence rates. In a given year or across years, the same person could have been hospitalized more than once. As such, the data reflect hospitalizations but not the incidence rates of hospitalizations among those with HIV/AIDS in the US population. Third, since only the first 7 diagnosis ICD-9-CM codes were recorded for each visit, our ability to identify hospitalizations of HIV-infected individuals might be artificially low because other diagnosis ICD-9-CM codes could have been reported preferentially for a patient visit. As a result, a given patient with HIV/AIDS with a diagnosis during his or her hospitalization that was considered more important, or had a higher billing potential, might not have been identified as such in the database. Furthermore, it is not possible to determine how many of these hospitalizations were or were not because of these patients’ HIV/AIDS status. It is also possible that for conditions not due to HIV/AIDS in the latter years of the study, the diagnosis of HIV/AIDS might no longer have been considered relevant, so was not captured in the NHDS data set and could have impacted estimates in this study. Finally, the number of HIV/AIDS hospitalizations in 1982 and 1983 in the NHDS database is fewer than 30 samples (before inflation according to the sampling scheme), which indicates that the sample might not convincingly represent the true distribution of these hospitalizations in those years.
Conclusion
Hospitalizations of HIV-infected individuals and days of care for these hospitalizations have decreased dramatically in recent years and decreased at rates greater than for hospitalizations of HIV-uninfected individuals. However, hospitalizations of HIV-infected individuals disproportionately involve certain populations and affect certain types of hospitals. However, once people with HIV/AIDS are hospitalized, it is reassuring that days of care are similar despite patient demography and hospital characteristics. Differences remain, however, in payment source along demographic characteristics. These trends in hospitalizations, days of care, and payment source should assist in public health planning for HIV/AIDS-related hospital care in the US.
Footnotes
Acknowledgements
Miao Tai was supported on a graduate assistantship from the Brown University Department of Emergency Medicine. This manuscript was prepared in partial satisfaction of her Master of Biostatistics thesis from Brown University. We wish to thank Wentao Guan for his assistance with the final preparation of this manuscript.
Authors’ Note
Preliminary findings from the study were presented at the 2012 National Summit on HIV and Viral Hepatitis Diagnosis, Prevention, and Access to Care, Washington, DC, November 27, 2012.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.