
Abstract
Patients treated in the specialized service at a midsized city in Brazil participated in a cross-sectional study that aimed to identify the risk factors for delayed diagnosis of HIV/AIDS. Through interviews and review of medical records, information was collected on sociodemographic and clinical characteristics and diagnoses. The study included 403 patients, of whom 216 (53.6%) were male and 311 (77.1%) had ≤8 years of education. According to the criteria adopted in this study, 162 (40.2%) of the participants had a late diagnosis of AIDS. Only 19 (4.7%) were diagnosed by routine examinations and 45 (11.2%) presented with AIDS-defining disease at the time of diagnosis. After adjustments, the results showed that having more education was protective against a late diagnosis for women. With the advance of the AIDS epidemic to small town and rural Brazil, vulnerable populations now include low-income and less educated women, most of whom have had monogamous relationships throughout their lives.
Introduction
HIV infection, the source of AIDS, currently represents a pandemic. It is a disease with a complex and variable epidemiology, which makes it necessary to evaluate carefully its regional characteristics. According to the Brazilian Ministry of Health, there have been 608 230 AIDS cases in Brazil between 1980 and 2011—constituting one of the highest rates in Latin America. In 2010, the incidence of AIDS in Brazil was 17.9 per 100 000 inhabitants. 1 The rates in the southern (28.8) and northern (20.6) regions remained above the national average. Conversely, the southeast (17.6), midwest (15.7), and northeast (12.6) regions have rates less than the national average. Additionally, the number of new cases is on the rise in the northern and northeast regions of the country. In the Minas Gerais State, the incidence rate in 2010 was 12 per 100 000 inhabitants (1). In Divinópolis, the city where the present study was conducted, the incidence rate in 2007 was 4 per 100 000 inhabitants, one of the lowest rates in the Minas Gerais State.
Specifically in relation to HIV/AIDS, it was initially believed among community and health professionals that the virus was restricted to high-risk groups such as men who have sex with men (MSM), individuals with hemophilia, individuals who inject drugs, and sex workers. Such beliefs were widespread in the general population and among health professionals. However, after more than 30 years since the diagnosis of the epidemic, there have been significant epidemiological changes; currently, there is a significant increase in the spread of the virus among heterosexuals and individuals over 50 years of age. In addition, records demonstrate a trend toward internalization and feminization of AIDS in Brazil as well as an increase in new cases among young women and men. 2,3 “Internalization” refers to growth of AIDS epidemic in Brazil, which started in its big cities and moved to midsized and small cities.
The Brazilian Health System offers the following network of services: counseling and testing centers, which focus on multiprofessional work and provide preventive and diagnostic testing for HIV, syphilis, hepatitis B, and hepatitis C; ambulatory care services for sexually transmitted diseases and HIV/AIDS; and specialized care services for sexually transmitted disease (STD)/AIDS Special Outpatient Service [SAE]. 4,5 The quality of care provided in these services, in addition to early diagnosis, is an important factor for reducing AIDS-related morbidity and mortality.
Despite the Brazilian public health policies aimed at controlling HIV/AIDS primarily through the provision of a network of health services and distribution of specific free antiretroviral therapy, there are still a large number of cases of late diagnosis and treatment. Among the causes for the delay in diagnosis and treatment of HIV are lack of awareness among patients with the risk of HIV infection, difficulty accessing and completing anti-HIV drug therapy, the late start of monitoring within the health services system, and the inappropriate use of health services. 6
Considering the epidemiological scenario of the disease, it is necessary to understand the clinical and epidemiological profile of patients in midsized cities and to identify potential high-risk groups in order to provide them with the proper means of prevention, early diagnosis, and effective treatment.
Methods
Area of Study
Divinopolis is a midsized city located in the Minas Gerais State in southeast Brazil. Its population is approximately 200 000 inhabitants, and the public health service consists of 1 philanthropic hospital, 1 emergency care service, 32 primary care units, and 1 specialized center called the SAE. The SAE is a public institution that serves a consortium of 55 municipalities in the midwest area of the Minas Gerais State.
Study Design
A cross-sectional study was conducted in the SAE. The initial screening of patients was conducted by reviewing medical records, after which a questionnaire was administered to all eligible patients once informed consent was obtained. The inclusion criteria were having a diagnosis of HIV (confirmed by anti-HIV enzyme-linked immunosorbent assay and Western blot tests) and being a regular user of the service. We considered regular users to be all patients who had medical consultation in the SAE in the last year. Individuals presenting mental problems and prisoners were excluded for the following reasons: patients with mental problems were not able to answer the questionnaires and prisoners were not allowed to stay alone with the interviewers—a policeman was always present because the SAE did not have a room with security bars. Given the inability to guarantee the same privacy for prisoners as for other participants, the ethical committee did not allow their participation. Children waiting for confirmatory tests were also excluded.
The questionnaire asked about sociodemographic characteristics, access to diagnostic and treatment services, knowledge of HIV/AIDS, risk behaviors, comorbidity (diabetes, cardiovascular disease, dyslipidemia, Chagas disease, and other sexually transmitted diseases), and use of alcohol and tobacco. All interviews were conducted by a physician or a nurse. Regarding illicit drugs, 2 questions were asked at different times in the questionnaire. The first asked the patient how he or she got HIV/AIDS, with one of the options being the use of injectable drugs. The second question asked whether he or she was a user of illegal drugs (injectable or not). Data on CD4 count and viral load of HIV were collected by undergraduate medical students. A delayed diagnosis was defined as a CD4 count of <200/mm3 at the first clinical evaluation or the presence of AIDS-defining illnesses upon admission. This definition is recommended by the US Centers for Disease Control and Prevention 7 and the Brazilian government. 8
Statistical Analysis
The analysis was performed using EPIINFO3.5.1 and STATA 11. The variables were summarized as percentages in each category, and between-group comparisons were made using a Pearson chi-square test. A univariate analysis was conducted to calculate crude odds ratios for categorical and binomial variables associated with late diagnosis (outcome variable). All variables with a P value <.20 in the univariate analysis were included in the multivariate model. To identify associated factors by sex group, univariate and multivariate data analyses were performed separately for men and women. In the final model, only significant variables (P < .05) were retained.
Ethical Issues
All patients received a study identification number, and only this number was included in the database for analysis. All interviews were conducted in a private room, and all patients gave written informed consent before being enrolled in the study. This study was approved by the local ethical committee (number 31/2010).
Results
In all, 720 HIV sero-positive patients were regularly followed by the SAE during the period of study. Among them, 263 (36.5%) were excluded, and 54 (7.5%) refused to participate in the study. Consequently, 403 (54%) patients signed the informed consent form and answered the questionnaire. Most of the participants were male (53.6%), 269 (66.75%) were younger than 41 years old, 179 (44%) were single, and 311 (77.2%) had a low level of education (≤8 years). Female participants were predominantly heterosexual (90.3%) and a higher percentage of them fell into the low-income group compared to male participants (42.8% vs 10.2%). We also found a significant difference in marital status, years of education, whether the patient had been referred to the specialist by a doctor or not, and drug use (Table 1).
Sociodemographic Profile of Participants According to Gender.
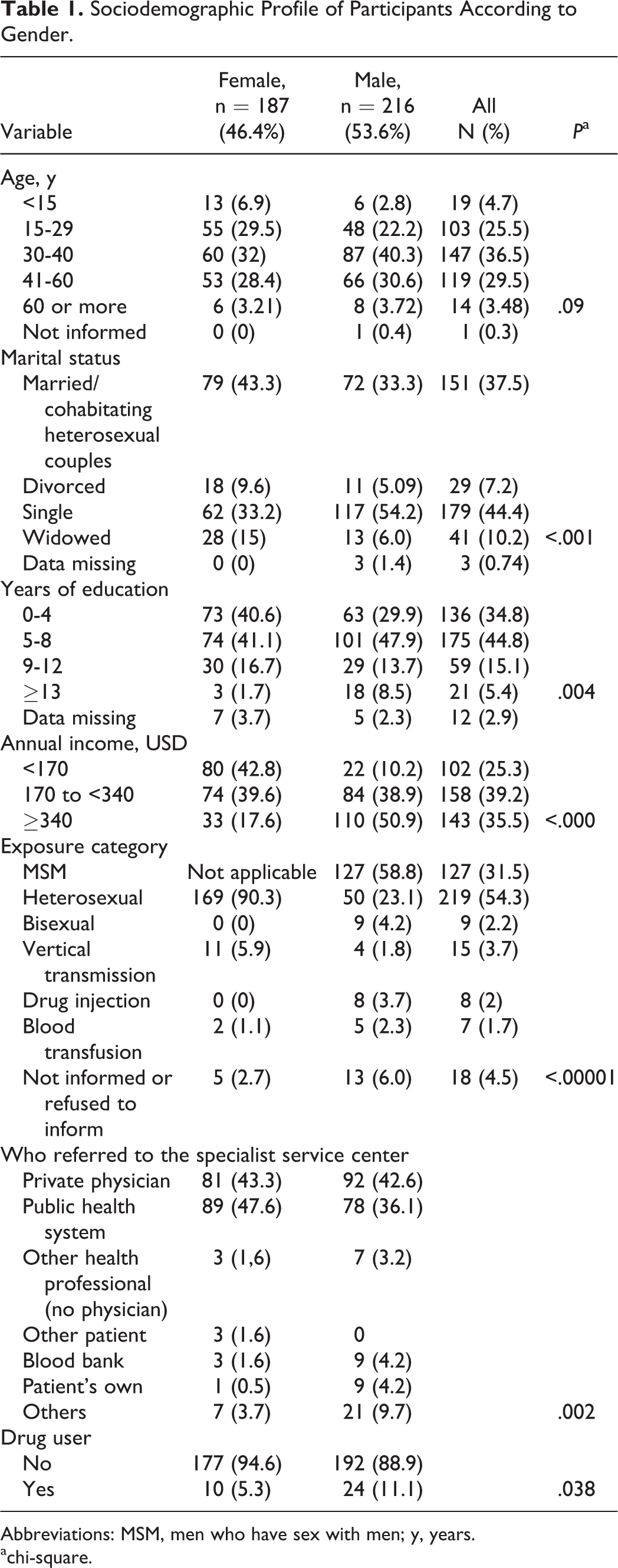
Abbreviations: MSM, men who have sex with men; y, years.
achi-square.
According to the criteria adopted in this study, 162 (40.2%) of the participants had a late diagnosis of AIDS (Table 2). Compared to patients with early diagnosis, a higher percentage of patients with late diagnosis fell into the low-income group (41.5% vs 26.5%).
Late Diagnostic of AIDS According to Demographic and Health Care.

Abbreviation: MSM, men who have sex with men.
achi-square.
Only 19 (4.7%) were diagnosed by routine examinations, and 45 (11.2%) presented with AIDS-defining disease at the time of diagnosis. The main comorbidities identified were cardiovascular disease (12.7%), dyslipidemia (8.2%), and diabetes mellitus (3.9%). After diagnosis, 279 (69.2%) patients presented to the SAE within 30 days, but 54 (13.4%) presented between 30 and 90 days post-diagnosis, and 67 (16.6%) patients presented more than 90 days after the confirmatory test. We omitted this information for 3 (0.8%) patients. Regarding alcohol and tobacco use, 72 (18%) patients reported having at least 1 alcoholic drink per week and 166 (40%) smoked more than 20 cigars per day.
A multivariate analysis indicated gender differences in the risk factors associated with late diagnosis. For women, but not men (Table 3), only more years of education was associated with having an early diagnosis. Among men, drug use had a stronger association with the likelihood of delayed diagnosis. Patients who had previously admitted to the physician their risk behavior had a significantly better likelihood of receiving an early diagnosis. According to Hosmer and Lemeshow goodness-of-fit test (P > .32), our model fits the data well.
Adjusted Odds Ratios for Delayed Diagnosis among Men and Women.

Abbreviation: CI, confidence interval.
aNo women included in these categories.
Discussion
Our results indicate that women represent almost 50% of infected patients in the region of study. This high percentage may reflect the feminization of AIDS in Brazil 5 and other countries. 9 The great majority (90%) acquired the infection through heterosexual relationships. In recent years, the spread of the AIDS epidemic among women has been accompanied by an increase in the number of infected heterosexual partners, pointing to a major change in the epidemiological profile of HIV-positive people in many countries, including Brazil. 1 In Brazil, the ratio of male to female infected patients ranges from 1.5 to 2 men for every 1 woman. By comparison, in sub-Saharan Africa, women are 1.4 times more infected than men. 9
Among men, acquiring the infection through sex with other men is still common (12%), followed by vertical transmission for children (4%) and injectable drug use (2%). Similar results have been observed in Tanzania, Nigeria, India, and other countries in Latin America. 9 Two percent of the patients reported being infected because of a blood transfusion although the transfusion occurred many years ago. One percent reported multiple forms of transmission.
Individuals with low levels of education, particularly women, are of concern and need to be studied further. Contrary to our results, some authors 1 have found that the level of education is high among HIV-positive patients in Brazil. A possible explanation for this is that most of our participants are poor and do not represent all infected people in the Divinopolis region. Because of prejudice, patients often seek care from a private physician instead of a public center or they look for treatment in another city in order to maintain their privacy. In a large city, many treatment services are offered, and it is easier for a patient to remain anonymous. In a midsized city, where only one treatment center is available, it is more difficult to go unrecognized.
After adjusting for other variables, having higher income was protective against a late diagnosis for women. With the advance of the epidemic to small town and rural Brazil, vulnerable populations now include women with low income and low education, most of whom have had monogamous relationships throughout their lives. The feminization of AIDS is a very complex phenomenon, considering the large gender inequalities in Brazil, where women may still be oppressed or subjugated by marital or stable relationships. Previous studies have reported that the feminization of AIDS became a national trend during the 1990s. 10 –12 In general, cultural issues involved in the feminization of the epidemic include the construction of female identity, fulfillment of gender roles, and power relations between genders. Brazilian studies indicate that the social norm of fidelity to partners among women promotes a sense of protection against the HIV virus, an issue observed especially among the poorest women. Discussions of prevention of STDs and AIDS would be considered unnecessary or even undesirable among stable couples, as it introduces the suspicion of sexual infidelity.
Sexist attitudes, gender asymmetry, and female subjugation still affect relationships between couples in Brazilian society. In this sense, when dialogue on prevention, which specifically involves the adoption of condom use by the couple, is introduced by the woman, she runs the risk of drawing suspicions of infidelity and promiscuity. 10 –12 Studies show that the dissemination of information among women about prevention and adoption of safe behaviors to contain the AIDS epidemic is not enough. In addition to information about means of infection, attention should be paid to the following components of female sexuality: the hierarchy that organizes the process of socialization of men and women in Brazil, the romantic ideals that guide monogamous relationships, economic dependence on partners, the practice of assessing partners based on experience, and the persistence of stereotypical ideas regarding who is at risk. These notions ultimately hinder discussions of risk and adoption of preventive measures, and they maintain the widespread misperception that such women have a very low disease risk. 10 –12
This scenario may also affect the timing of diagnosis. We found that almost 30% of patients delayed starting treatment more than 30 days. This finding is similar to that of a national study 13 but contradictory to the findings from other regional studies. 14 Most patients received the diagnosis after the manifestation of a minor sign, such as a mild or moderate immunological problem or an AIDS-defining disease. Notably, most patients were below 40 years old and single.
The finding that injectable drug use was significantly associated with having a delayed diagnosis among males should be viewed from 2 aspects. The first one is that the relationship between injectable drug use and risk behavior is well established, but patients may omit to provide this information during their routine visits. Our results show that patients who have admitted to drug use were less likely to have a delayed diagnosis. Castilla et al 15 found that fewer individuals with a history of injecting drugs had late HIV diagnoses, but Fernandes et al did not find the same result in a study conducted in Belo Horizonte, Brazil. 15 The apparent contradiction in the results—that is, we observed drug use to be a risk factor but the admission of drug use to the doctor was protective—deserves discussion. These findings could be explained by differences in the routine AIDS tests used by doctors, depending on the information they receive from patients. Patients who more readily report drug use have a greater opportunity for diagnosis than do others. Clearly, the relationship of trust between doctors and patients may be an important factor in early diagnosis, as the patient will be more sincere with a doctor he or she trusts. In the public services, patients do not always have the option to choose their doctor, in addition to shorter examination times. These factors may hinder the development of a good doctor–patient relationship and thus contribute to late diagnosis.
Conclusion
Our study shows that HIV/AIDS has some unique and important epidemiologic characteristics. Although some follow the epidemiological trends observed in Brazil, others indicate a change in the profile of infected individuals. Thus, local health care professionals and authorities need to conduct specific interventions, respecting and coordinating with national policies, while keeping in mind the characteristics of the region, with the aim of reducing the regional incidence of HIV/AIDS and ensuring accessibility to health services for diagnosis and treatment.
Although our research was conducted in a Brazilian region, we report issues that may be found in other regions and developing countries. Factors associated with delayed diagnosis may be related to gender, access to health services, and local characteristics. Prevention campaigns must consider these characteristics in order to obtain better results.
Footnotes
Acknowledgments
We would like to thank the SAE, the PROPE/UFSJ, CNPQ, and FAPEMIG for awarding scholarships to the medical students who worked on this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.