
Abstract
Objectives:
This study was conducted to evaluate the clinical experience with daptomycin in the treatment of resistant gram-positive infections (GPIs) in patients with HIV infection.
Methods:
Using a retrospective, multicenter, and observational registry study, investigators assessed outcomes following daptomycin therapy in 78 patients (62 efficacy evaluable) infected with HIV and with resistant GPIs.
Results:
Overall, success rates by infection type were bacteremia 91% (20 of 22), endocarditis 91% (10 of 11), and bone/joint 100% (9 of 9). Success by pathogen was 93% (39 of 42), 93% (14 of 15), and 100% (5 of 5) for methicillin-resistant Staphylococcus aureus, vancomycin-resistant enterococci, and methicillin-resistant coagulase-negative staphylococci, respectively. Daptomycin appeared to be well tolerated, with 9% having an adverse event possibly related to daptomycin and 4% discontinuing daptomycin.
Conclusions:
In HIV-infected patients, daptomycin appears to be a useful agent for treating resistant GPIs.
Introduction
Recent studies have shown a higher burden of infection with community-acquired methicillin-resistant Staphylococcus aureus (MRSA) in patients with HIV infection than in other patients. 1 HIV has also been identified as a risk factor for vancomycin-resistant enterococcal (VRE) bacteremia. 2 However, there are only limited data on the treatment of patients with HIV infection who develop resistant gram-positive infections (GPIs). With an increasing number of reports of vancomycin failure and reduced susceptibility of gram-positive bacteria to vancomycin, alternative agents for GPIs are frequently considered. 3 –7
Daptomycin, a lipopeptide antibiotic, 8 is approved for the treatment of bacteremia caused by S aureus, including right-sided endocarditis as well as complicated skin and skin structure infections (SSSIs) caused by certain gram-positive organisms. 9 This retrospective study, which was performed to characterize the clinical experience with daptomycin in patients with HIV infection and resistant GPIs, is the first report of daptomycin use in patients infected with HIV.
Methods
The Cubicin Outcomes Registry and Experience (CORE) was a multicenter, retrospective, and observational chart review study assessing the characteristics and clinical outcomes of patients receiving daptomycin. 10 A standardized case report form and protocol were used to collect demographic and clinical information for patients treated with daptomycin from multiple institutions in the United States from 2005 through 2009. After institutional review board or ethics committee approval, trained study investigators obtained clinical information from medical records. Study methods were published previously. 10
Patient Selection
This analysis included patients with HIV infection and documented infection with methicillin-resistant S aureus, vancomycin-resistant enterococci, or methicillin-resistant coagulase-negative staphylococci (MRCoNS).
Clinical Data Collected
Clinical data collected were patient demographics; initial and final doses, dosing intervals, and length of therapy with daptomycin; previous, concomitant, and follow-up antibiotic therapy; and reason for prior antibiotic discontinuation. Patients with more than 1 reported infection were assigned to a single category using the following hierarchy: endocarditis > bone/joint infection > bacteremia > SSSI > urinary tract infection (UTI)/pyelonephritis > other. Community-phenotype MRSA was defined as susceptible to clindamycin and trimethoprim/sulfamethoxazole.
At the end of daptomycin therapy, patients were classified as having 1 of the following 4 clinical outcomes: cure, improved, failure, or nonevaluable. Cure was defined as clinical signs and symptoms resolved and/or no additional antibiotic therapy necessary, or a negative culture reported at the end of therapy. Criteria for an improved outcome were the partial resolution of clinical signs and symptoms and/or additional antibiotic therapy warranted at the end of therapy. Failure was defined as an inadequate response to therapy, resulting in worsening or new/recurrent signs and symptoms, or the need for a change in antibiotic therapy, or a positive culture reported at the end of therapy. A patient was considered nonevaluable if the investigator was unable to determine the response because of insufficient information; all other patients comprised the evaluable population. The success rate was defined as the sum of cure and improved outcomes divided by the sum of cure, improved, and failure outcomes.
The safety assessment was based on the identification of adverse events (AEs), as defined by the International Conference on Harmonization. All patients receiving at least 1 daptomycin dose were included in the safety analysis. Adverse events reported from the first daptomycin dose until 30 days after the last dose were recorded.
Data Analysis
Statistical comparisons were performed using the appropriate parametric or nonparametric test. Statistical significance was defined as P < .05 and was used to determine the relevance of the data. SAS version 9.1.3 and JMP version 9.0.0 (SAS Institute Cary, NC) were used for data analysis.
Results
Of the 78 patients who met the eligibility criteria for HIV infection and resistant GPI, 62 (79%) were evaluable for outcome. Patient demographics are summarized in Table 1. The majority of patients were diagnosed with bacteremia or endocarditis followed by SSSIs, bone and joint, and UTI/pyelonephritis (Table 2). The sources of bacteremia were reported as catheter related without other sources identified (n = 10) and noncatheter related (n = 12) with sources identified as UTI/pyelonephritis (n = 3), skin wound or ulcer infections (n = 3), and spinal abscess (n = 1). Of the 6 patients with MRSA, the source of bacteremia was central venous catheter (n = 4), skin wound (n = 1), and spinal abscess (n = 1).
Baseline Demographic and Clinical Data for Evaluable Patients.a

Abbreviations: CrCl, creatinine clearance; ICU, intensive care unit; MRCoNS, methicillin-resistant coagulase-negative staphylococci; MRSA, methicillin-resistant Staphylococcus aureus; VRE, vancomycin-resistant enterococci; WBCs, white blood cells.
aData presented as n (%).
bPatients could have >1 underlying disease.
cAn additional 6 patients received daptomycin as an inpatient with unknown outpatient experience.
dOne patient was coinfected with VRE.
Success Rate by Infection Type and Pathogen in the Evaluable Population.
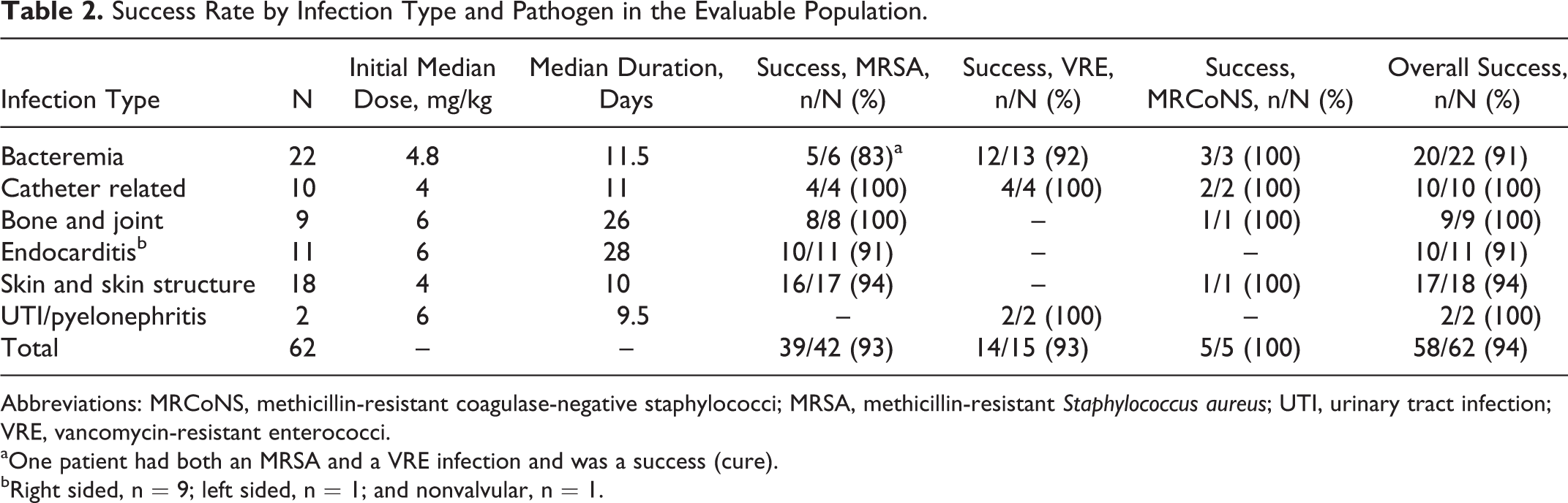
Abbreviations: MRCoNS, methicillin-resistant coagulase-negative staphylococci; MRSA, methicillin-resistant Staphylococcus aureus; UTI, urinary tract infection; VRE, vancomycin-resistant enterococci.
aOne patient had both an MRSA and a VRE infection and was a success (cure).
bRight sided, n = 9; left sided, n = 1; and nonvalvular, n = 1.
Daptomycin Dosage Regimen
The median (range) initial daptomycin dose was 6 mg/kg (3-10 mg/kg). The initial median dose for patients with bacteremia was 4.8 mg/kg, but 4 patients with bacteremia or endocarditis had their dose increased from 4 to 6 mg/kg. The dose of 1 patient with endocarditis was decreased from 5.6 to 5 mg/kg. Final median doses of daptomycin by infection type were 6 mg/kg for bacteremia, bone and joint infection, UTI/pyelonephritis, and endocarditis, and 4 mg/kg for SSSI. The doses for bacteremia and SSSI were consistent with approved labeling. 9
At the beginning of daptomycin therapy, 7 (41%) of the 17 patients with an initial creatinine clearance (CrCl) of <30 mL/min or receiving dialysis were administered daptomycin every 24 hours. However, of the 15 patients with CrCl <30 mL/min by therapy end, only 1 (7%) patient remained on a once-daily schedule.
The overall median duration and range of daptomycin treatment were 15.5 days (1-94 days). The median (range) duration of daptomycin treatment by infection type was bacteremia, 11.5 (5-28) days; bone and joint infection, 26 (12-94) days; endocarditis, 28 (7-61) days; SSSI, 10 (1-46) days; and UTI/pyelonephritis, 9.5 (9-10) days.
Previous and Concomitant Antibiotic Therapy
Before receiving daptomycin, 52 (84%) of the 62 evaluable patients received previous antibiotic therapy for a median duration of 7 days. Although the majority of patients either failed or could not tolerate the prior antibiotic regimen, they may have contributed to the clinical outcome described. The most common prior antibiotics were vancomycin (37 of 52, 71%) and linezolid (13 of 52, 25%). Data on previous vancomycin duration were available for 19 patients (median 7 days; range, 2-24 days). Overall, 15 (29%) patients failed their prior antibiotic therapy, and 14 (27%) patients switched because of allergy, toxicity, or intolerance. For those on prior vancomycin or linezolid, 9 (24%) of the 37 and 2 (15%) of the 13, respectively, switched because of treatment failure, and 8 (22%) of the 37 and 5 (38%) of the 13 switched because of allergy, toxicity, or intolerance.
Of the 62 evaluable patients, 38 (61%) received concomitant antibiotics with daptomycin. The most common concomitant antibiotics were intravenous vancomycin (8 of 62, 13%), cefepime (7 of 62, 11%), and azithromycin (7 of 62, 11%). The majority of concomitant antibiotic use was directed at other pathogens, and only 12 patients received a concomitant antibiotic with activity against the resistant gram-positive pathogen.
Safety
Thirty AEs were reported in 18 (23%) of the 78 patients. Seven (9%) patients had 12 AEs classified as being possibly related to daptomycin. There were 2 reports each of creatine phosphokinase (CPK) increase and nausea, and 1 report each of diarrhea, hiccups, liver function test (LFT) increase, lethargy, herpes simplex, renal failure, thrombocytopenia, and vomiting. None of these events were assessed as meeting the regulatory criteria for seriousness. Of the 78, 8 (10%) patients had serious AEs, but none were considered possibly related to daptomycin. Because of an AE, 3 (4%) of the 78 patients discontinued daptomycin. One patient discontinued daptomycin because of CPK elevation and increased LFTs, another had respiratory failure, and a third patient had septic shock.
Outcomes
Successful outcomes were reported in 58 (94%) of the 62 patients (Table 2). Overall success rates (cure/improved) by type of infection were 91% (55%/36%) for bacteremia, 91% (55%/36%) for endocarditis, 94% (44%/50%) for SSSI, 100% (56%/44%) for bone and joint infection, and 100% (50%/50%) for UTI/pyelonephritis. Overall, surgical intervention data were available in 29 of the 62 evaluable patients. Successful outcomes were numerically higher in those patients undergoing any surgical treatment, 15 (100%) of the 15 versus 11 (79%) of the 14, P = .09. The subgroup of patients with catheter-related bacteremia was treated successfully. Success was not statistically different between those patients with bacteremia with or without a catheter source (100% versus 83%, P = .48). In all, 10 patients with catheter-related bacteremia had surgical data reported and 5 patients had their catheters either exchanged or removed during daptomycin therapy. Overall success rates by type of pathogen were 93% for MRSA and VRE and 100% for MRCoNS. In the subset of patients with community-phenotype MRSA, the success rate was 94% (17 of 18). Of those who failed prior vancomycin, the success rate was 100% (9 of 9). The receipt of concomitant antibiotics did not change the outcomes; success rate with concomitant antibiotics was 34 (89%) of 38 and 100% in those without concomitant antibiotics. Outcomes in those patients where the concomitant antibiotic was active against the resistant gram-positive isolate produced similar results, success rate of 10 (83%) of the 12.
Discussion
This analysis of CORE 2005-2009 data is the first report of real-world experience with daptomycin in the US patients with HIV infection and resistant GPIs. Among the efficacy-evaluable patients, the most frequent causative pathogen was MRSA (68%; 42 of 62), followed by VRE (24%; 15 of 62) and MRCoNS (8%; 5 of 62). The use of daptomycin, a bactericidal antibiotic, in this population demonstrated an overall success rate of 94% in patients with difficult-to-treat infections, including bacteremia, bone and joint infection, and endocarditis. Overall success rates by type of pathogen were 93% for MRSA and VRE and 100% for MRCoNS.
A recent systematic review by Huson and colleagues showed that the incidence of community-acquired bacterial bloodstream infections is markedly higher in HIV-positive adults (20.0%) than in HIV-negative adults (9.2%) and that the odds ratio (OR) for developing a bloodstream infection is significantly greater in HIV-positive adults (2.48; 95% confidence interval [CI], 2.10-2.93). 11 Treatment with antiretroviral therapy (ART) reduces the overall incidence of bacterial bloodstream infections, 11,12 but bacteremia remains more common in HIV-infected patients than in other patients, irrespective of ART. 11,12 The mortality rate for bloodstream infections in HIV-infected patients is considerable, ranging between 7% and 46%. 11 Given the poor outcomes often associated with these infections, the success rates of patients with bacteremia in the present study, ranging from 93% for MRSA to 100% for MRCoNS, are noteworthy.
A single-center, retrospective cohort study of HIV-infected adults with S aureus bacteremia found that 87 (66%) of the 131 patients had MRSA and that 47 (36%) of the 131 patients had community-associated MRSA (CA-MRSA). 13 Patients with CA-MRSA had nearly 3 times the odds of developing endocarditis as other patients with S aureus bacteremia, and this association was statistically significant (OR, 2.73; 95% CI, 1.30-5.71). Furthermore, CA-MRSA was associated with nearly 3 times the odds of in-hospital mortality (OR, 2.93; 95% CI, 0.78-10.96). In this study, outcomes for patients with community-phenotype MRSA—94% success rate—were similar to the overall MRSA results.
This study’s outcomes are consistent with recent articles independently reporting on the outcomes of daptomycin for resistant GPIs. Carugati and colleagues reported an in-hospital mortality rate of 14% for high-dose daptomycin patients with MRSA left-sided endocarditis. 14 Murray et al studied MRSA bacteremia with vancomycin minimum inhibitory concentrations >1 mg/L and showed that daptomycin success in those patients with or without endocarditis was 60% (12 of 20) and 86% (56 of 65), respectively. 15 Casapao et al published results from a multicenter study of high-dose daptomycin for enterococcal infections. The overall clinical success rate in this group of patients with primarily bloodstream infections (71%) and VRE (83%) was 89% (193 of 218). 16 White and Seaton reviewed daptomycin comparative studies for complicated SSSIs and found a success rate of 81% (60 of 74) in the subset of patients infected with MRSA. 17 Our data are not directly comparable to these studies because of differences in outcome definitions and follow-up, but a success rate of 83% to 91% for bacteremia and endocarditis and >90% for other GPIs after daptomycin therapy is promising in this population.
Daptomycin was well tolerated in the present population of patients with HIV infection, frequent and severe comorbidities, and complicated drug regimens. Only 4% of patients discontinued treatment because of an AE, a rate within the range from previous controlled trials. 9,18 The AE profile of daptomycin in these patients was similar to that observed in 547 clinically evaluable patients with S aureus bacteremia, endocarditis, or skin infection included in a CORE 2005-2008 study. 18 In the cohorts of patients with HIV infection in the present study and in the previously referenced report, 18 incidence rates were 23% and 15%, respectively, for any AE, 9% and 6% for AEs classified as possibly related to daptomycin, and 0% and 0.4% for serious AEs possibly related to daptomycin.
Creatine phosphokinase increases, sometimes marked, have been reported with daptomycin use. 9 In the comparative study of daptomycin versus standard therapy for S aureus bacteremia and endocarditis, for example, CPK elevations were reported in 6.7% of daptomycin-treated patients and led to treatment discontinuation in 3 (2.5%) of the 120 patients. 19 In the present study, CPK increases were reported at a slightly lower frequency, in 2 (3%) of the 78 patients. One (1%) patient discontinued daptomycin due to CPK elevation (and increased LFTs).
Several limitations of the present study should be noted. This was an observational, retrospective study involving a limited number of patients with no comparator arm. Data were not collected on patients’ ART regimens or viral burdens, and limited data were available on the extent of their immunosuppression. Similarly, there were limited data on previous infections and surgical intervention at the site of infection. Finally, investigator assessment was performed at the end of therapy.
In summary, data from this observational retrospective study show promising results concerning the use of daptomycin in HIV-infected patients with resistant GPIs, including those caused by MRSA, VRE, and MRCoNS. The safety profile of daptomycin in patients with HIV infection appears to be similar to that observed in other patients. Based on these findings, prospective controlled studies are warranted to further evaluate daptomycin for the treatment of this medically complex, difficult-to-treat population.
Footnotes
Authors’ Note
Data were presented in part at ID Week, San Francisco, CA, USA, October 2-6, 2013. KCL designed methods and was involved in collecting all data. All authors discussed analyses, interpretation, and contributed to and approved the article. Manuscript assistance was provided by ApotheCom, Yardley, PA, USA. This assistance was funded by Cubist Pharmaceuticals.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Jihad Slim is on the speakers bureau for Cubist Pharmaceuticals, Forest Laboratories, Gilead, Abbvie, Jansen, ViiV, Merck, Genentech, and Bristol-Myers Squibb. Humberto Jimenez is on the speakers bureau for Bristol-Myers Squibb. Darren Culshaw, Hina Patel, and Kenneth Lamp are employees and stockholders of Cubist Pharmaceuticals.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research described in this report was funded by Cubist Pharmaceuticals, Lexington, MA, USA.