
Abstract
We report the psychometric properties of 2 Spanish-language scales designed to measure (1) opinions about HIV in the community and particularly among health care workers and (2) observed acts of stigma toward people living with HIV/AIDS (PLWHA) by health care workers. The Opinions about HIV Scale included 3 components (policy, avoidance, and empathy) and 9 items, while an adapted version of the HIV/AIDS Stigma Instrument–Nurse, designed to capture acts of stigma, included 2 components (discrimination related to clinical care and refusal to share or exchange food/gifts). Scales demonstrated good reliability and construct validity. Relative to community health workers, treatment supporters were more likely to have stigmatizing opinions related to avoidance and empathy. We offer 2 Spanish-language scales that could be used to identify populations with high levels of stigmatizing opinions and behaviors toward PLWHA. Formal training of health care workers, especially treatment supporters, may raise awareness and reduce stigma toward HIV.
For people living with HIV/AIDS (PLWHA), perceived HIV-related stigma from community members can have critical consequences to health and well-being. Perceived HIV-related stigma has been shown to be associated with lower HIV testing rates 1,2 and among PLWHA may lead to reluctance to disclose the diagnosis 3 and engage in HIV health services and care 4 –8 while adversely influencing mental health, quality of life, 4,9 –11 and adherence to antiretroviral therapy (ART). 7,12 The reach of HIV-related stigma may extend beyond HIV services and outcomes, limiting employment opportunities and factoring into reproductive health decisions. 13 –15
Stigmatizing opinions and behaviors among health care workers may have especially negative consequences for PLWHA due to the frequency with which they interact with PLWHA and to the health care workers’ perceived role as authority figures. 16 Although health care workers have traditionally been viewed as those individuals trained as health professionals, increasingly, many national HIV programs have incorporated lay individuals (eg, community health workers, peer or family treatment supporters) to strengthen support and medication adherence for PLWHA. 17 –21 Herein collectively referred to as health care workers, both health professionals and lay workers may have stigmatizing attitudes and behaviors toward PLWHA, and without proper training, their fundamental role in social support and advocacy may be undermined by these predisposing attitudes. Furthermore, these opinions and behaviors may be transmitted to other health care workers, community members, and family members of PLWHA, perpetuating a culture of HIV-related stigma. Although prior work suggests that stigmatizing attitudes among health care workers may vary by individual and health facility, 22,23 both community- and facility-based interventions to reduce stigma have been successful, 24 –26 underscoring the importance of assessing HIV-related stigma in this influential group in order to identify sites most in need of intervention. If found to be prevalent, stigmatizing opinions and behaviors among health care workers may be an indicator of high levels of stigma in the general community.
We report the psychometric properties of 2 Spanish-language scales designed to measure (1) opinions about HIV in the community and particularly among health care workers and (2) acts of stigma toward PLWHA by health care workers. We also explore differences in stigmatizing opinions toward PLWHA among 3 groups of health care workers, that is, health professionals, community health workers, and treatment supporters.
Methods
Study Setting
Peru has an HIV prevalence of 0.40%, and the majority of the estimated 65 000 cases are found in the nation’s urban capital of Lima. 27 Prior work in Lima found that fear of stigma or unwanted disclosure was a key barrier to adherence among PLWHA. 28
Study Population
This analysis was conducted using baseline data from a cluster randomized trial of directly observed combination ART. To achieve a primary trial objective of comparing social capital among community members in intervention versus control communities, we enrolled 1062 health care providers, including a diverse group of health professionals (including but not limited to physicians, nurses, social workers, psychologists, nutritionists, and pharmacists), community health workers (lay health workers appointed by the Ministry of Health), and HIV treatment supporters (a relative or a friend identified by the patient to support them in treatment adherence as a programmatic requisite to starting ART). These analyses include the baseline interview data collected from this community cohort. We excluded individuals who lacked baseline data or completed the stigma questionnaires more than 60 days after enrollment.
Scale Development
To develop the Opinions about HIV Scale, we conducted a review of existing questionnaires and selected questions that aligned with 3 domains (empathy, avoidance, and policy) from the AIDS Attitude Scale for the general public, the Tanzania HIV/AIDS Stigma Indicator Survey, and the AIDS-Related Stigma Scale. 29 –31 These domains, or ones similar, were commonly included in questionnaires designed to measure HIV-related stigma among community members. 2,32 –35 Respondents were asked to rate their level of agreement with each opinion (definitely true, I think so, I don’t know, I don’t think so, and definitely false). Each response was assigned a value from 1 to 5, with higher values indicating greater agreement with stigmatizing opinions. Because we hypothesized that some individuals might not openly discuss their own feelings of stigma, we additionally inquired about witnessed acts of stigma using an adapted version of the HIV/AIDS Stigma Instrument–Nurse (HASI-N) questionnaire developed by Uys and colleagues. 36 Respondents were asked to describe the frequency with which they had witnessed a list of stigmatizing acts by other health workers in the last 3 months (never, one or two times, several times, many times/almost always). We scored each response on a scale of 0 to 3 with higher scores representing more frequent observation of stigmatizing acts.
We applied the questions to a small group of treatment supporters and community health workers and discarded questions with a ceiling effect. To further attenuate possible ceiling effects, we reworded some questions based on the pilot testing experience. From the adapted version of the HASI-N, we removed 2 items related specifically to inpatient care, since community health workers and treatment supporters might not have ample exposure to witness interactions within the hospital (“A nurse did not check the condition of her HIV/AIDS patient in the unit/ward and A nurse left an HIV/AIDS patient for a long time in a soiled bed”). The following four additional items were added to the scale by the local team of community health workers and nurses based on prior experience in working with PLWHA in this setting: “A health care worker revealed the HIV status of a patient with HIV/AIDS without permission;” “A health care worker denied care to a patient with HIV/AIDS;” “A health care worker refused to accept a gift from a patient with HIV/AIDS;” and “A health care worker refused to share food or beverage with a patient with HIV/AIDS.”
Data Analysis
We conducted 2 principal components analyses, 1 for the Opinions about HIV Scale and 1 for the adapted HASI-N. To determine the number of components to retain, we examined scree plots and considered the eigenvalue-one criterion and overall interpretability. 37 An item was considered to have loaded to a component if it had a factor loading of 0.45 or greater for that component. To create the final scales, we removed items that loaded to more than 1 component at 0.45 or greater and items that did not load to any factor. We assessed reliability by standardized Cronbach α coefficients.
To examine construct validity, we created factor scores for each scale and examined whether stigmatizing opinions about HIV/AIDS tended to be associated with characteristics previously shown to be associated with stigmatizing attitudes or opinions in other studies, including education level, age, gender, HIV infection, and the number of acquaintances known to have HIV/AIDS. 34,38 –42 Based on these studies, we hypothesized that lower education, older age, never having been tested for HIV, negative or unknown HIV status, and no friends or family members with HIV/AIDS could be associated with more stigmatizing opinions about HIV/AIDS in this setting. To identify associations between scale scores and hypothesized predictors, we created binary outcome variables based on the scores of each of the subscales. Individuals with a score greater than the 75th percentile for a given scale were classified as having a high stigma score. We modeled these binary outcomes in univariable and multivariable logistic regression models using generalized estimating equations with an exchangeable correlation structure, which adjusted for clustering at the health center level, the unit of randomization in the trial generating the data. Because there was little missing data, we conducted a complete case analysis.
Results
Characteristics of Participants
Of 1062 health care workers, 13 (1%) were excluded from this analysis due to missing baseline data (n = 4), a missing baseline stigma questionnaire (n = 1), or completion of baseline stigma questionnaires more than 60 days after enrollment (n = 8). The median time from enrollment to completion of the stigma questionnaire was 0 days (interquartile range: 0 to 8 days) in the 1049 health care workers included for analysis. More than half of these (52%) were health professionals and more than one-third (35%) were treatment supporters. Table 1 shows the characteristics of this cohort. Women comprised the majority of participants, and 39% had completed university. Notably, community health workers and health professionals had more years of experience in these roles relative to treatment supporters (median of 9.7 and 13.0 years versus 0.0 years, respectively). Of the health care workers, 86% reported knowing and were willing to report their HIV status, and of these, 8% reported being HIV infected. All HIV infections but 1 (99% of infections) were reported among treatment supporters, representing a prevalence of at least 20% among this group of health care workers. Eighty-three (8%) health care workers reported being HIV negative in spite of never having an HIV test.
Characteristics of the Health Care Workers.a

Abbreviation: IQR, inter quartile range.
a N = 1049, unless otherwise noted.
bOne health professional also reported working as community health worker, therefore, the total number of responses is 1050.
Opinions about HIV Scale
Principal components analyses of the 13 items selected for the Opinions about HIV Scale revealed a 3-factor structure according to the scree plot and the eigenvalue-one criteria. The 3 components aligned with the domains of empathy, avoidance, and policy identified a priori. We iteratively removed from the final scale the following items that did not load to a single component: “For most people who have HIV/AIDS, they have themselves to blame,” “People who have HIV/AIDS are dirty,” and “I think a woman who gives birth to an HIV-positive baby should be denounced.” We also removed “I would feel uncomfortable if I learned a friend has HIV/AIDS” which had similarly low loadings (0.47 and 0.41) on 2 components. The factor loadings for the 9 items retained in the final scale are shown in Table 2.
Health Care Workers’ Opinions about HIV/AIDS.a

aFactor analyses included 1022 individuals with responses to all questions.
We observed heterogeneity in the level of health care worker agreement with each of the 9 situations presented in the final version of the Opinions about HIV Scale. Three items mapping to the policy subscale were associated with the highest percentages of respondents agreeing with stigmatizing opinions. Specifically, 36% of health care workers responded “I think so” or “definitely true” for the statement “If my child’s classmate has HIV, I have the right to know,” and 20% of health care workers responded in this way for the statements “It is risky for people who have HIV/AIDS to work with children” and “There are times when it is necessary for people with HIV/AIDS to have restrictions on their freedom.” Respondents demonstrated the greatest level of disagreement with the statements on the empathy subscale, with more than 92% of respondents answering definitely false or I don’t think so to the 2 stigmatizing opinions comprising this subscale.
Observations of Enacted Stigma (Adapted Version of the HASI-N)
Examination of the scree plot, and the eigenvalue-one criteria indicated that the 12 observations of enacted stigma corresponded to a 2-factor structure. The 2 components corresponded to acts of discrimination related to the clinical care provided to patients and refusal to exchange food or gifts with patients (Table 3). One item (“A health care worker made an HIV/AIDS patient do things for himself/herself to avoid touching him/her”) was removed due to loadings of 0.45 or greater on both components, and a second item (“A health care worker revealed the diagnosis of an HIV/AIDS patient without the permission of that patient”) was removed for having loadings that were both low and similar for the 2 components (0.49 and 0.43). The factor loadings for the 10 final items are shown in Table 3. Acts of stigma by other health care workers during the 3 months prior to interview were commonly reported, with 47% of respondents reporting at least 1 of the 10 acts included in the final scale. The most commonly reported acts, described by nearly 30% of respondents, were providing poor quality of care to PLWHA and keeping a distance when talking to PLWHA.
Health Care Workers’ Observations of Stigmatizing Acts by Other Health Care Workers against People Living with HIV/AIDS.a

aFactor analyses included 1037 individuals with responses to all questions.
Reliability
The Opinions about HIV Scale showed good reliability overall (Cronbach α of .72), while the shorter subscales of avoidance, empathy, and policy demonstrated lower but acceptable reliability (Cronbach α of .60, .69, and .63, respectively). The reliability of the adapted HASI-N scale was excellent with an α coefficient of .90 for all 10 items and αs of .90 for the 7-item discrimination related to clinical care scale and 0.75 for the 3-item refusal to exchange scale.
Construct Validity
In both univariable and multivariable analysis, education level was a consistent correlate of stigmatizing opinions and of the reported acts of stigmatizing behavior by other health workers (Tables 4 and 5). Having an education level higher than high school was associated with lower scores (ie, less stigmatizing opinions) on 2 of the 3 Opinions about HIV subscales (avoidance, empathy) and was positively associated with higher scores (i.e., more observation of acts of stigma by other health care workers) on the adapted HASI-N. We hypothesized that individuals with an HIV diagnosis would have less stigmatizing opinions than those with HIV-negative or unknown status. We only observed this to be true for the Opinions about HIV avoidance subscale. Having HIV infection was strongly and statistically significantly associated with lower scores on this scale.
Associations between Previously Reported Correlates of Stigma and Health Care Workers’ Observations of Stigmatizing Acts by Other Health Care Workers (Adapted HASI-N).a
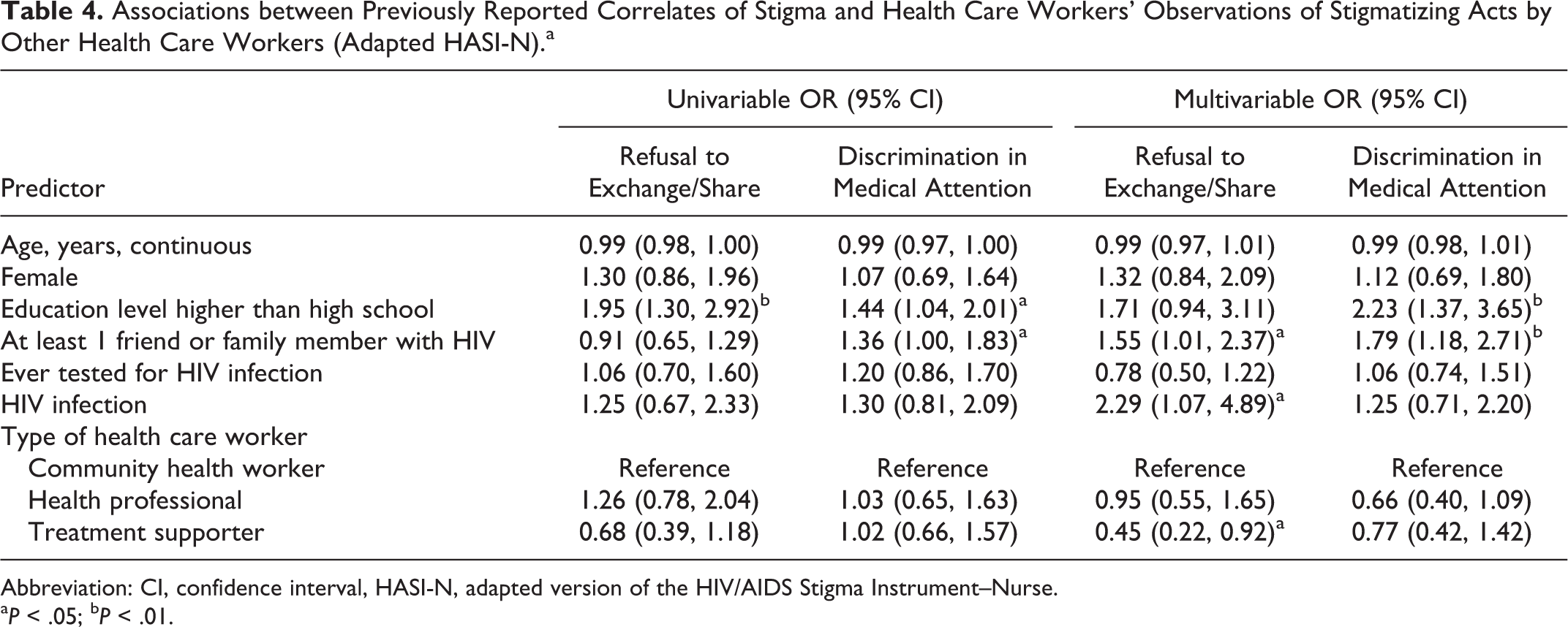
Abbreviation: CI, confidence interval, HASI-N, adapted version of the HIV/AIDS Stigma Instrument–Nurse.
a P < .05; b P < .01.
Associations between Previously Reported Predictors of Stigma and Opinions about HIV in Health Care Workers.a
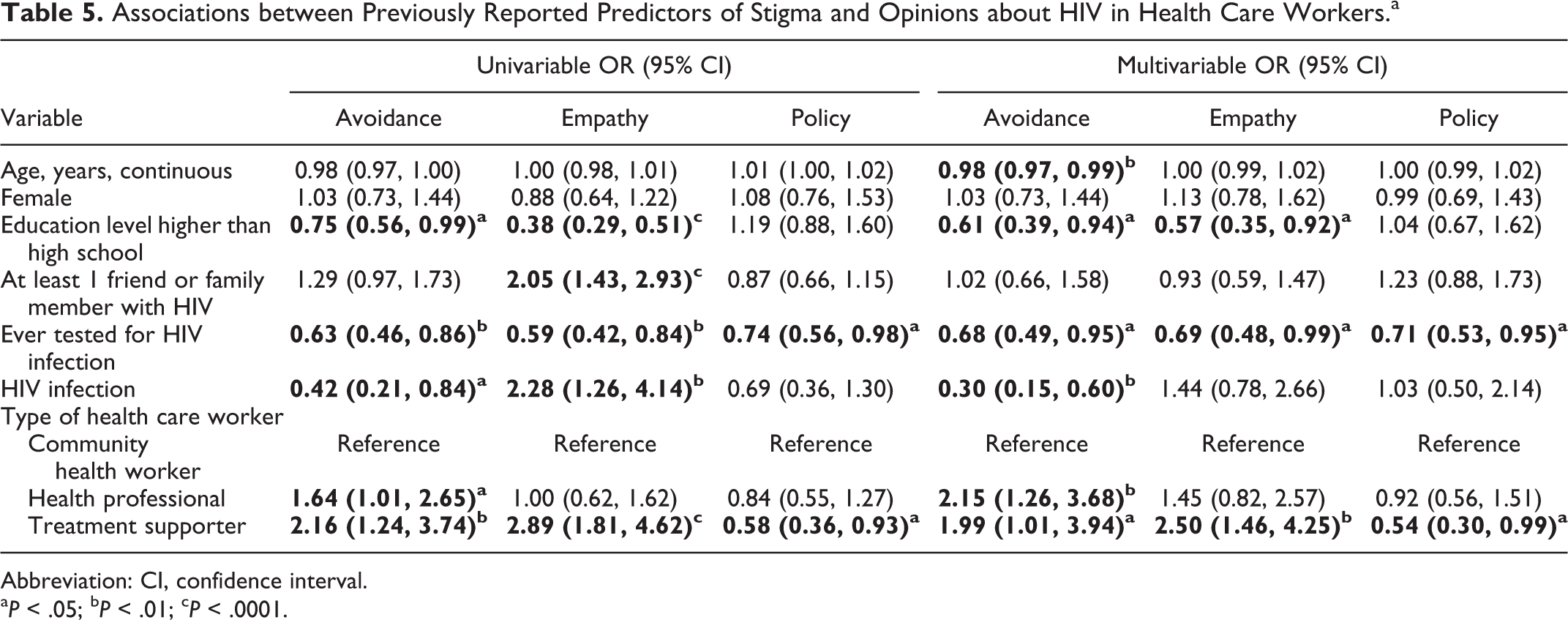
Abbreviation: CI, confidence interval. a P < .05; b P < .01; c P < .0001.
Relative to community health workers, treatment supporters were more likely to have stigmatizing opinions related to avoidance and empathy but less likely to have stigmatizing opinions regarding policies related to HIV/AIDS. They also less frequently reported witnessing acts of stigma by other health care workers related to the refusal to share or exchange items such as food. Health professionals were more likely than community health workers to have stigmatizing opinions related to avoidance. English- and Spanish-Language versions of the final scales are provided in the Appendix A.
Discussion
To our knowledge only 2 prior Spanish-language scales have been developed to measure HIV-related stigma in community members, and none to date have evaluated HIV-related stigma across a broad spectrum of lay and professional health care workers (including family or friend treatment supporters). A principal benefit of the scales presented here is that, with 10 or fewer items each, they are shorter than existing Spanish-language scales. One comprehensive scale developed by Varas-Díaz and Neilands in Puerto Rico to assess HIV-related stigma among health workers considers 11 HIV/AIDS stigma dimensions. 43,44 With more than 50 items in the scale’s final version, it may be challenging to implement it in some settings. Similarly, Ugarte and colleagues developed and validated 2 additional Spanish-language scales in Nicaragua to measure HIV-related discrimination actions and HIV-related stigma attitudes 40 ; these scales had 15 and 18 items, respectively.
Although shorter scales have the advantage of time and resource efficiency, one disadvantage is that they may tend to be less reliable than scales with a larger number of items. 37 This was evident by the α coefficients observed for the Opinions about HIV subscales, which were on the lower end of acceptability. When considered together, however, the 9 scale items demonstrated good reliability with a Cronbach α of .72. Our goal of creating scales with distinct subscales resulted in the elimination of a number of initial candidate items from the Opinions about HIV Scale. Although the final empathy and avoidance subscales only had 2 items each, they nonetheless were associated with factors such as lower education and no prior HIV testing, which have previously been shown to be associated with stigmatizing opinions.
Analysis of data derived from the scales suggests that acts and opinions of stigma persist among health care workers in this setting, and therefore, interventions addressing community-level stigma may be critical to achieving desirable HIV testing rates and optimal HIV outcomes. Interestingly, relative to community health workers, treatment supporters were more likely to report stigmatizing opinions. This may be due to the fact that treatment supporters tended to be relatively new to this role, have lower health literacy regarding HIV, and could potentially have greater concerns regarding their personal safety, given their proximity to the PLWHA. On the other hand, given that treatment supporters are selected by the PLWHA themselves to be a confidant and supporter, stigmatizing attitudes toward HIV could profoundly interfere in these individuals’ ability to provide effective support. Formal training or education of treatment supporters to raise awareness and reduce stigma toward HIV could improve the effectiveness of this programmatic role. Even among community health workers and health professionals, who generally receive education related to HIV and modes of transmission, the persistence of stigmatizing acts and attitudes reflects the need to reinforce this training once these workers actually begin to work with PLWHAs. This observation is consistent with conclusions drawn by Brown and colleagues on the basis of a review of 22 HIV/AIDS stigma reduction interventions. They concluded that information alone is not sufficient to change attitudes or behavior toward PLWHA but that information in combination with contact with PLWHA offers promise. 26 Furthermore, the messenger and source of HIV-related information may matter. One multisite cluster randomized trial from Peru found that HIV information delivered by respected individuals in the context of casual conversation had long-term benefits in HIV stigma reduction in community members. 45 A similar trial from China found that popular opinion leaders at country hospitals were effective in reducing HIV-related stigma in health care workers. 25
Conclusions
We offer 2 Spanish-language scales that could be used to identify populations with high levels of stigmatizing opinions and behaviors toward PLWHA, those that could benefit from tailored interventions designed to reduce stigma. We believe that the performance of the scale is likely generalizeable to other health care workers in urban Latin America and may also have utility among community members other than health care workers. Although important progress has been made worldwide in the rollout of life-saving ART for PLWHA, further efforts to reduce stigma will likely be critical to achieve optimal levels of HIV testing, retention in care, and adherence to treatment.
Footnotes
Appendix A
Acknowledgements
We acknowledge and thank Lirio Silverio and Olga Saldaña for their support with data entry and data management.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Mental Health at the U.S. National Institute of Health under Grant R01MH08355.