
Abstract
To determine the optimal time to track patients, we evaluated the outcomes of patients traced after missing their return visits at 3 periods, 8, 30, or 90 days, at the Infectious Diseases Clinic in Kampala, Uganda. During the study period from January to December 2011, the proportion of untraceable patients was 2 (4%) after 8 days, 12 (10%) after 30 days, and 13 (15%) after 90 days. More than 75% of the patients who died had a CD4 count of <200 cells/mm3 at their last visit. In conclusion, tracking patients after 1 week of a missed return visit should be the preferred method of tracking. If resources are limited, patients with CD4 counts <200 cells/mm3 need to be targeted for tracking, as they are most at risk of dying if they interrupt treatment.
Introduction
Several studies have shown that a large proportion of patients who miss return visits remain untraceable after tracking, and they are thus considered lost to follow-up (LTFU). 1 –7 Nevertheless, more patients can be tracked, if more time is spent meticulously locating patients’ homes 8,9 or if patients are tracked within 30 days of a missed return visit. 10,11 The optimal time for tracking patients, however, remains to be determined. In this study performed at the Infectious Diseases Clinic (IDC) in Kampala, Uganda, we evaluated 3 different periods of tracing patients, namely, tracking after 8, 30, or 90 days of a missed return visit. Additionally, we determined the utility of a physical address form in facilitating patient tracking.
Materials and Methods
The Study Site
The IDC is the clinic of the Infectious Disease Institute (IDI), Makerere University College of Health Sciences. It is located at the Mulago hospital campus, the main national referral hospital in Uganda. Since 2002, the IDC has been providing free antiretroviral (ARV) drugs to eligible HIV-positive patients. 12 Patients on antiretroviral therapy (ART) visit the IDC on a monthly basis for a clinical assessment by doctors/nurses or for drug refills through pharmacy-only refill program (PRP). 13 Every 6 months, a CD4 count is performed. Daily, over 400 patients receive care at the IDC; two-thirds of them are on ART.
Progress Made in Patient Tracking
In 2007, the IDC initiated tracking of patients who were considered LTFU using patients’ or their relatives’ phone numbers, or in those cases where phone numbers were unavailable home visits were performed. However, more than 30% of the patients were untraceable because of wrong or missing telephone contacts and home addresses. 2 In the last quarter of 2007, a physical address form was introduced, which enabled in obtaining the correct contact information of the patients. This physical address form was completed at registration in the clinic and updated at the start of ART. The form contained the following information: a phone contact and ownership, the patient’s disclosure status if the phone contact was for someone else, the patient’s consent to be contacted by phone or through a home visit, and a location map to the patient’s home.
From January to December 2008, using the updated patients’ information, home visitors tracked those HIV-positive patients on ART who did not return to the clinic within 90 days after missing an appointment. Of the 209 patients, 29% were untraceable, 34.4% had self-transferred, and 36.3% were dead. The high proportion of both untraceable and dead patients raised concerns that tracking patients 90 days after a missed appointment may be too late to reduce LTFU. 14
In January 2011, we identified 4582 HIV-positive patients attending the IDC, who were aged 18 years and older, who had visited the clinic within 90 days prior to the study period, and who had a return visit planned within the next 30 days.
In a prospective study, we randomly selected 1145 (25%) of these patients. Patients who missed return visits for 7 days or more were identified using a list generated from the IDC database. Then, these patients were tracked from March 1 to March 31, 2011, after 8 days; from May 1 to June 30, 2011, after 30 days; and from September 1 to December 23, 2011, after 90 days. The number of days missed were determined from the scheduled return visit.
Using these lists, home visitors tracked the patients within 1 or 2 days. Patients were contacted using the phone numbers. Home visits were carried out if a patient could not be contacted by phone, the patient’s residence was within 20-km radius from the IDC, a map of the location to the patient’s home was available, and the patient had consented for a home visit. The home visitors noted one of following outcomes on a tracking form: the patient died, self-transferred, was planning to return, or was untraceable.
Data Collection
Using data abstraction forms, information was collected by trained research assistants from 3 sources: the IDC database, the medical notes, and the tracking forms. The IDC database was managed by the data manager; the medical notes were completed by doctors/nurses, while the tracking forms were completed by the home visitors. Data were double entered into EPIDATA version 3.1 statistical software (Epi-data, Norway), cleaned, edited, coded, and exported to STATA statistical software version 11 (Stata Corp, College Station, Texas) for analysis. All information were analyzed anonymously.
Statistical Analysis
To describe the characteristics of the patients who were tracked, we used counts and percentages for categorical variables and means with 95% confidence intervals or medians with interquartile ranges for continuous variables. To determine the optimal timing for patient tracking, we compared the proportion of untraceable patients’ within the 3 tracking methods, that is, after 8, 30, and 90 days.
We used Kruskal-Wallis test for median CD4 counts and Pearson chi-square test or Fisher exact test for cell frequencies of less than 5 for proportion. We used 2-tailed tests and an α level of .05 for all our analyses. Since our sample size was small, our comparisons were limited to bivariate analysis.
Finally, to determine the utility of a physical address form in facilitating patient tracking, we compared the proportion of untraceable and traceable patients with completed physical address forms using the Pearson chi-square test or Fisher exact test for cell frequencies of less than 5.
Ethics
The study was approved by the IDI Scientific Review Committee and the Institutional Review Boards for School of Medicine, Makerere University College of Health Sciences, and the Uganda National Council for Science and Technology.
Results
From March to December 2011, a total of 256 patients missed their return visits for at least 7 days. Of these, 117 (45.7%) patients resumed care spontaneously before tracking started and 139 (54.3%) patients were tracked. The following are the tracking details of the 139 patients: 51 (96%) patients were tracked after 8 days, 45 (39%) patients after 30 days, and 43 (49%) patients after 90 days.
The proportion of untraceable patients was 2 (4%, which is the least) in the group tracked after 8 days, whereas the proportion of untraceable patients in the other groups were 12 (10%) after 30 days and 13 (15%) after 90 days (Figure 1).

Flowchart describing sample selection and outcome of tracking methods at a large HIV/AIDS clinic in Kampala, Uganda. *PTR indicates planning to return.
The characteristics of the patients tracked are shown in Table 1. At ART initiation, 81 (58%) patients belonged to World Health Organization disease stage III or IV. In all, 13 (9.3%) patients at ART initiation and 62 (44%) at last visit had a CD4 count ≥350 cells/mm3.
Sociodemographic and Clinical Characteristics of Study Participants.

Abbreviations: ART, antiretroviral therapy; d4T, stavudine; LPV/r, lopinavir/ritonavir; WHO, World Health Organization; ZDV, zidovudine.
The characteristics of patients based on the tracking outcome are shown in Table 2. One hundred twelve patients (80%) were traceable. Among those traceable, 38 (27%) patients had self-transferred to other treatment centers, 18 (13%) patients were dead, and 56 (40%) patients reported that they were planning to return to the IDC. Of those who reported that they were planning to return, 52 (93%) came back within 120 days. In all, 11 (40%) of the untraceable patients and 11 (61%) of the dead patients had been on ART for less than 6 months. Fourteen (77%) patients who died had a CD4 count <200 cells/mm3 at their last visit. Of the traceable patients and untraceable patients, 91 (81%) patients and 16 (59%) patients, respectively, had a completed physical address form in their files (P = 0.001; Table 3).
Characteristics of Tracked Patients: Bivariate Analysis.

Abbreviations: ART, antiretroviral therapy; d4T, stavudine; ZDV, zidovudine; 3TC, lamivudine; NVP, nevirapine; LP/r, lopinavir/ritonavir; EFV, efavirenz; IQR, interquartile range; PTR, planning to return.
aTraceable includes patients who were successfully tracked: dead, self-transferred, or PTR.
bFisher exact test.
Evaluation of Information on the Physical Address Form Using the Patient Tracking Outcome: Bivariate Analysis.
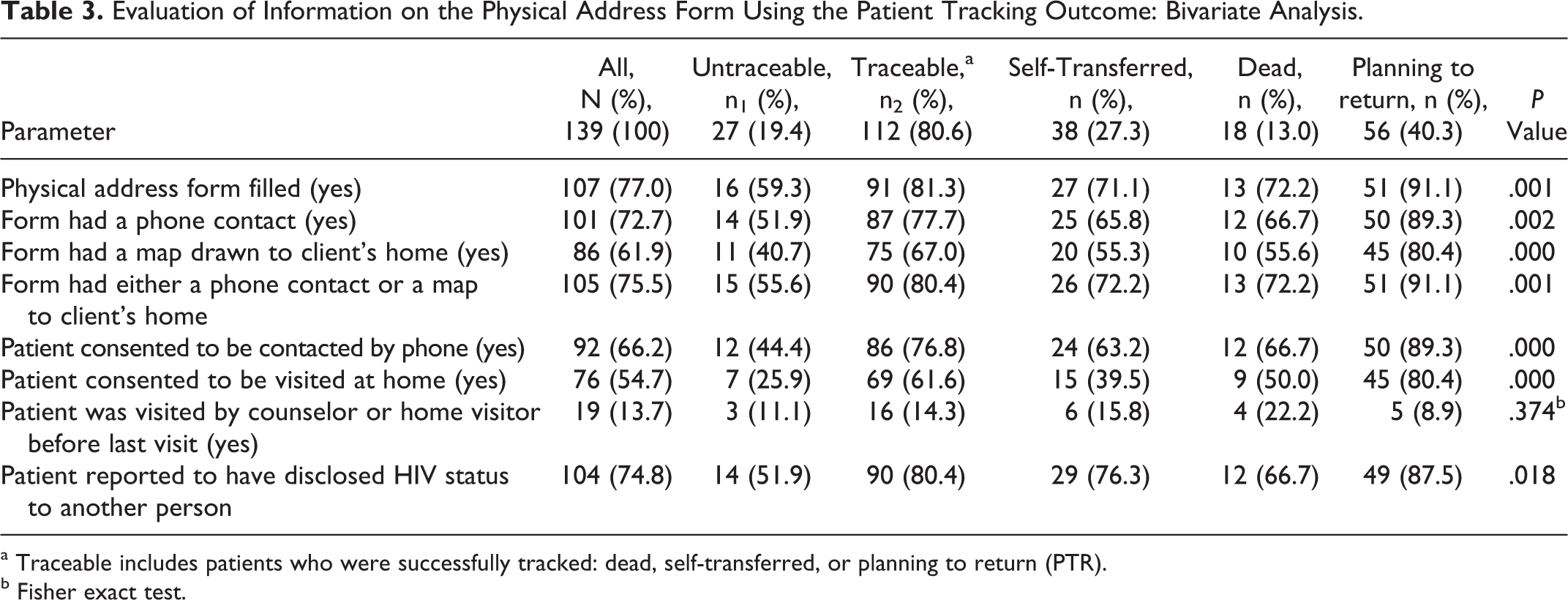
a Traceable includes patients who were successfully tracked: dead, self-transferred, or planning to return (PTR).
b Fisher exact test.
Discussion
The main objective of our study was to determine the best time to track patients on ART who missed their return visits. We found that tracking patients after 1 week of a missed return visit is the preferred way because it allowed us to trace 90% of the patients still alive.
By tracking patients early, treatment interruptions can be avoided. Moreover, in patients on a nonnucleoside reverse transcriptase inhibitor regimen, this decreases the risk of developing resistance. However, early tracking may not be cost effective as one may have to trace many patients, and some of them may still have enough ARV drugs and are planning to return spontaneously to the clinic. In our study, 83% of the patients tracked after 8 days were planning to return to the IDC.
Special attention should be given to patients who have just started ART. A large proportion of the untraceable and the dead had been on ART for less than 6 months. Patients are vulnerable during early treatment period because of toxicity, less established adherence, and residual immunosuppression. 1,3,4 It is justifiable that ART programs should trace these LTFU patients more aggressively than those who are stable on treatment.
If resources are limited, the patients’ CD4 count could be used to establish tracking priorities. More than 75% of our patients who died had a CD4 count <200 cells/mm3 at their last visit, mandating tracking patients with a low CD4 count a priority.
Providing patients with enough drug supply should be another priority to avoid treatment interruptions. Patients with a high CD4 count prefer to visit the treatment center less frequently. 15 Therefore, these patients should also receive a sufficient supply of drugs to avoid running out of drugs.
By tracing patients after 30 days, 20% of them were either untraceable or dead. A small proportion of patients are planning to return to the clinic. Therefore, tracking after 30 days is generally too late. By tracking patients after 90 days instead of 30 days, we found only a slightly higher proportion of untraceable and dead patients (22%). The reason for this unexpected result is that the tracking lists only contained patients with unknown outcomes. Patients who were officially transferred or known to be dead did not appear on the list. It is possible that some of patients’ outcomes in these categories were entered in the database.
The proportions of untraceable patients reported by previous studies vary from 4.8% to 45.7% (Table 4). 4,5,7,8,11,14,16 –18 Several factors may explain these differences and also provide guidance on what needs to be done to improve the tracking of patients. These factors include presence of a regular tracking system using an electronic database that can quickly identify patients, 11,16 a short period between a missed return visit and the date of tracking, 10,11,16 availability of updated contact addresses, patients having consented for tracking, 18 use of trackers/home visitors with a good understanding of the tracking process, 6,8,9,11 the time spent in trying to contact the patient, 8 –11 and whether the patient resides within a localized catchment area. 8,10,16 Home visits may be impossible if a patient resides very far from the clinic or relocates to an unknown location.7,17 Although programs with better access to resources, both financial and human, may have better tracking systems, all facilities can update patients’ contact addresses on a regular basis.
Tracking Methods of Patients on ART after a Missed Appointment in Resource-Poor Settings.
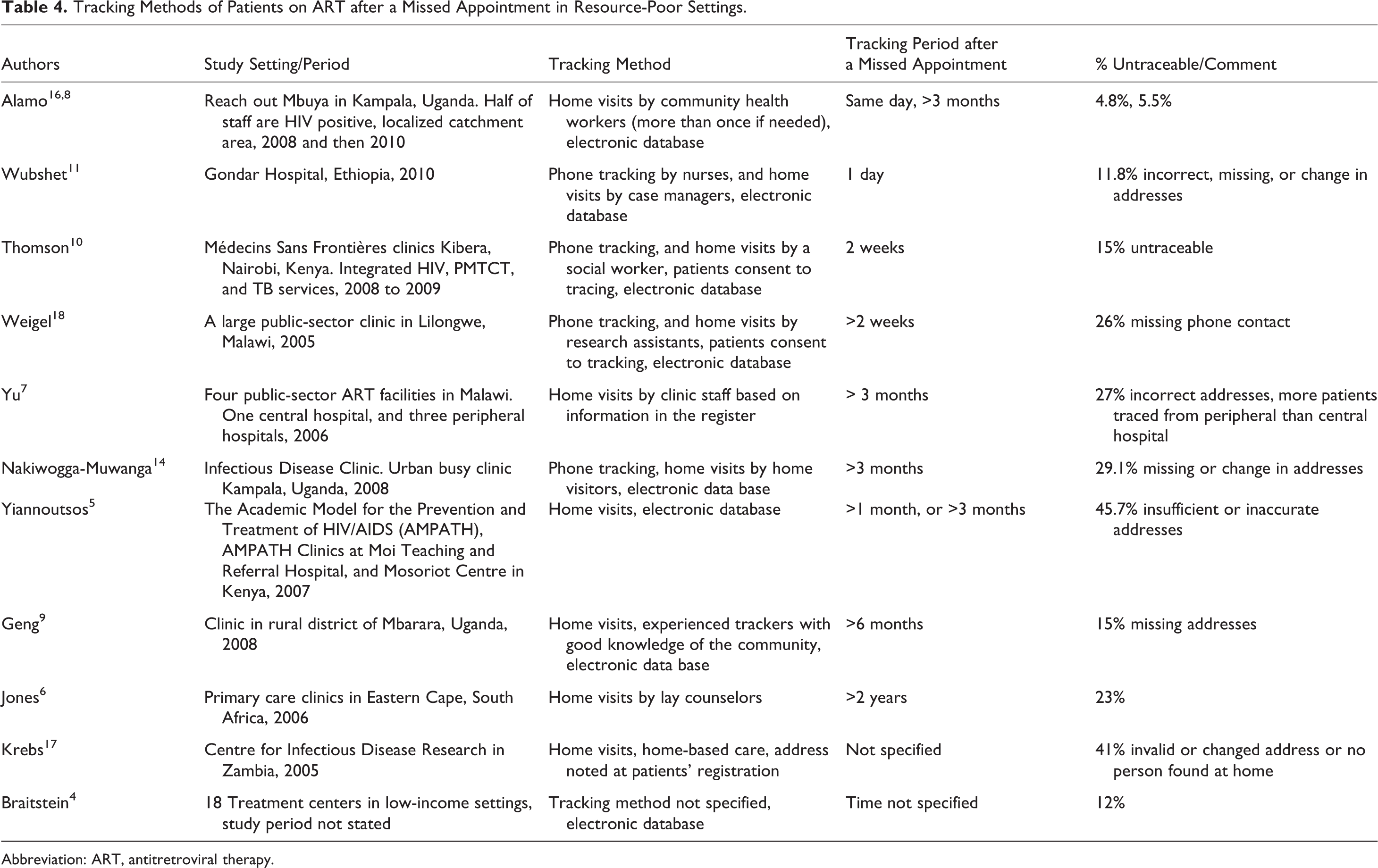
Abbreviation: ART, antitretroviral therapy.
We found that the use of a physical address form can facilitate the tracking of patients. Indeed, 81.3% of the traceable patients had a completed physical address form compared to 59% of the untraceable patients. In our study, physical address forms were completed when patients first registered at the clinic and were updated at ART initiation. One explanation why certain patients with completed physical address forms were not traced is that home visitors did not try enough to contact them. For example, they only tracked patients during working days.
We suggest that another study should be carried out, which randomly assigns patients to the different tracking periods. Patients in the different groups should have identical counseling process. Patients’ addresses/phone numbers should be complete at the time of study enrollment. The information on time and cost of finding a patient should be documented. A large sample size should be used to allow for multivariable analysis so as to identify independent factors associated with tracking periods.
Our study has several limitations. It was an observational study; stronger evidence could have come from a randomized controlled trial. Another limitation is that it was not possible to ascertain the quantity of drugs the patients received at their last visit, and the study home visitors never inquired whether patients at the time of tracking still had drugs left.
In summary, this study demonstrates that tracking after 1 week of missed return visit is more likely to successfully contact patients. In order to determine the optimal time to track patients, different factors need to be taken into account. Does the patient still have ARV drugs? Is he or she at risk of developing an opportunistic infection? Our study shows that early tracking has the advantage of finding more patients and to find them alive. If resources are limited, then patients with CD4 count <200 cells/mm3 need to be targeted for tracking because they are most at risk of dying if they interrupt treatment. Moreover, health facilities need to ensure that complete address and contact information are collected at the time of registration and that this information is regularly updated during the follow-up of the patient.
Footnotes
Acknowledgments
We would like to thank all the patients and staff for all their contributions toward the conduct of the study. We would also like to thank the Belgian Technical Cooperation (BTC), Gilead, San Francisco, and Infectious Diseases Institute for financial support. Special thanks to Agnes Kiragga, Richard Orama, Barbara Castelnuovo, and Racheal Musomba for their contribution in the streamlining of the tracking process at the IDC.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.