
Abstract
A retrospective cohort study was conducted and 129 patients with a diagnosis of HIV infection for more than 10 years were identified. Half the patients were men and mean (standard deviation, SD) age at HIV diagnosis was 33.2 (9.2) years. One third had a diagnosis of AIDS at cohort entry with median (interquartile range, IQR) CD4 counts of 259 (112-430) cells/mm3. All received antiretroviral therapy with median (IQR) current CD4 counts of 502 (363-607) cells/mm3 and 95% had HIV RNA <50 copies/mL. For adverse events, 28% experienced drug resistance, 27% experienced hospitalization, 59% had dyslipidemia, 35% had creatinine >1.0 mg/dL, and 5% had glucose >126 mg/dL. In conclusion, immunological and virological responses can be achieved among patients with a diagnosis of HIV infection for more than 10 years even in a resource-limited setting. Adverse events are common. Preparation for monitoring and management of these adverse events is a crucial part of successful long-term HIV care.
Introduction
HIV infection can be accounted as one of the chronic infectious diseases requiring long-term therapy with antiretroviral (ARV) drugs. The use of effective antiretroviral therapy (ART) or highly active antiretroviral therapy (HAART) has significantly prolonged the time between HIV diagnosis and progression to AIDS, including death, in both developed countries 1 and in developing countries. 2 –4 A study from India showed that the mean duration of survival from serodiagnosis was 92 months and ART improved the odds of survival by approximately 5 times. 4
Some patients may experience any adverse events, such as HIV drug resistance and hospitalization, along the course of HIV infection and HIV treatment. Furthermore, metabolic syndrome, a condition characterized by the clustering of alterations in lipid metabolism, glucose metabolism, and blood pressure, 5 is more common in HIV-infected individuals compared with the general population. 6,7 Several studies reported the possibility of late toxicity of ARV drugs such as renal dysfunction, 8 dyslipidemia, and cardiovascular disease. 9,10
It is estimated that 90% of HIV-infected persons worldwide live in developing countries. Since 2004, the number of people receiving therapy has increased substantially, and in 2010, exceeded 5 million people in low- and middle-income countries. 11 In 2009, the Joint United Nations Programme on HIV/AIDS (UNAIDS) reported a 30% increase in the number of people receiving treatment in a single year. 11 Few reports with regard to the clinical characteristics of HIV-infected patients who survive after the diagnosis of HIV infection for more than 10 years in developing countries or resource-limited settings in the HAART era have been published. Knowledge among various populations is crucial in order to estimate the extent of the epidemic, the treatment outcomes as well as its complications, and to evaluate intervention. We aimed to determine the clinical characteristics and adverse events occurring among patients in Thailand, who survive for more than 10 years after the diagnosis of HIV infection.
Patients and Methods
A retrospective cohort study was conducted at Ramathibodi Hospital (a 1000-bed university hospital in Bangkok, Thailand). Adult patients with age
The following variables were collected: (1) the clinical characteristics including gender, age, route of HIV acquisition, health insurance, opportunistic infections, AIDS-defining illness, the Centers for Disease Control and Prevention (CDC) stage, 12 underlying condition, and ART, and (2) laboratory-related data including complete blood count, blood chemistry, CD4 counts, and HIV RNA at cohort entry and current visit, including hepatitis B virus, and hepatitis C virus profile at any time point.
Statistical Analysis
Mean (standard deviations, SD) or median values (interquartile range, IQR) and frequency were used to describe the patients’ characteristics for continuous and categorical data, respectively. Chi-square test or Fisher exact test was used to compare the categorical variables. Wilcoxon signed rank test was used to compare the difference or change in CD4 counts and HIV RNA between 2 time points. Logistic regression was used to determine the factors associated with adverse events. Its 95% confidence interval (CI) was also estimated. Variables with P values <.10 were considered in a multivariate logistic regression model after assessment of multicollinearity of variance inflation factors. Variables were selected into a multiple logistic regression model with forward selection and ones that attained a level of significance were retained in the model. A P value <.05 was considered statistically significant. All statistical analyses were performed using Stata statistical software version 10.0 (Stata Statistical Software: Release 10.0, Stata Corporation, College Station, Texas, 2007).
Results
A total of 129 patients were identified. Of these, 65 (50.4%) patients were men with a mean (SD) age at HIV diagnosis was 33.2 (9.2) years. Median (IQR) duration of HIV diagnosis was 12.6 (10.9-14.6) years and ranged from 10.0 to 21.2 years. Mean (SD) age at current visit was 46.2 (9.3) years and ranged from 27.8 to 76.7 years. Most patients (92.2%) had heterosexual risk. Approximately 75% of them had at least one form of health insurance. Thirty-one (24%) patients had other underlying conditions of which hypertension (6.2%) and diabetes mellitus (5.4%) were the most common. Prevalence of hepatitis B virus and hepatitis C virus coinfection were 10.1% and 8.5%, respectively. Clinical characteristics and laboratory investigations of the patients with a diagnosis of HIV infection for more than 10 years are summarized in Table 1.
Clinical Characteristics and Laboratory Investigations of 129 Patients with a Diagnosis of HIV Infection for More Than 10 Years
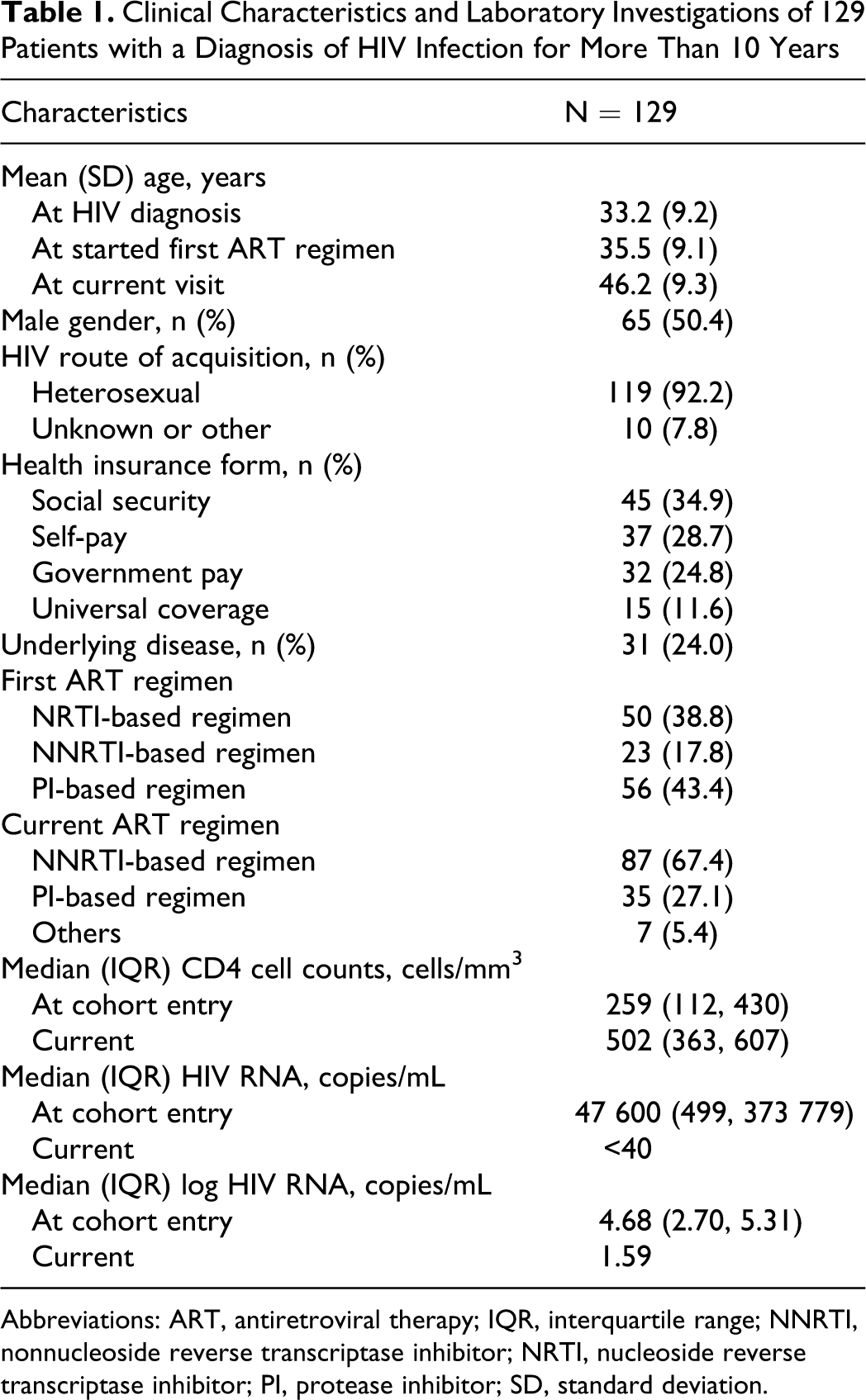
Abbreviations: ART, antiretroviral therapy; IQR, interquartile range; NNRTI, nonnucleoside reverse transcriptase inhibitor; NRTI, nucleoside reverse transcriptase inhibitor; PI, protease inhibitor; SD, standard deviation.
By the 1993 CDC classification, 94 (72.9%) patients, 20 (15.5%) patients, and 15 (11.6%) patients were diagnosed as stage A, B, and C, respectively. Among 15 patients with CDC stage C, 1 patient had stage C1, 4 patients had stage C2, and 10 patients had stage C3. Forty-two (32.6%) patients had a diagnosis of AIDS. Of the 110 patients who had CD4 counts at cohort entry, the median (IQR) CD4 was 259 (112, 430) cells/mm 3 . Median (IQR) HIV RNA at cohort entry was 4.68 (2.70, 5.31) copies/mL.
All patients were receiving HAART during the study data collection period. A mean (SD) age at the start of the first ART regimen was 35.5 (9.1) years. A median (IQR) duration of the first ART regimen and the current regimen was 15.6 (5.8, 54.8) months and 33.9 (16.7, 68.9) months, respectively. Eight (6.2%) patients were receiving the current regimen which was the same as the first regimen. Protease inhibitor (PI)-based regimen was prescribed as the first regimen in 43.3%, followed by nucleoside reverse transcriptase inhibitor (NRTI)-based regimen (eg, NRTI monotherapy or dual NRTIs) in 38.8% and non-NRTI (NNRTI)-based regimen in 17.8%. The NNRTI-based regimen was the most commonly prescribed current regimen (67.4%), followed by PI-based regimen (27.1%) and others (5.4%). There was a significant difference between a proportion of patients receiving NNRTI-based regimen as the first regimen and those receiving as the current regimen (17.8% vs 67.4%, P < .001). Current median (IQR) CD4 count was 502 (363, 607) cells/mm 3 and 95% had HIV RNA <50 copies/mL. Overall median (IQR) change in CD4 count was 241 (45, 425) cells/mm 3 , P < .001 (Figure 1). Overall median (IQR) change in HIV RNA was −3.05 (−1.11, −3.66) copies/mL, P < .001 (Figure 2).
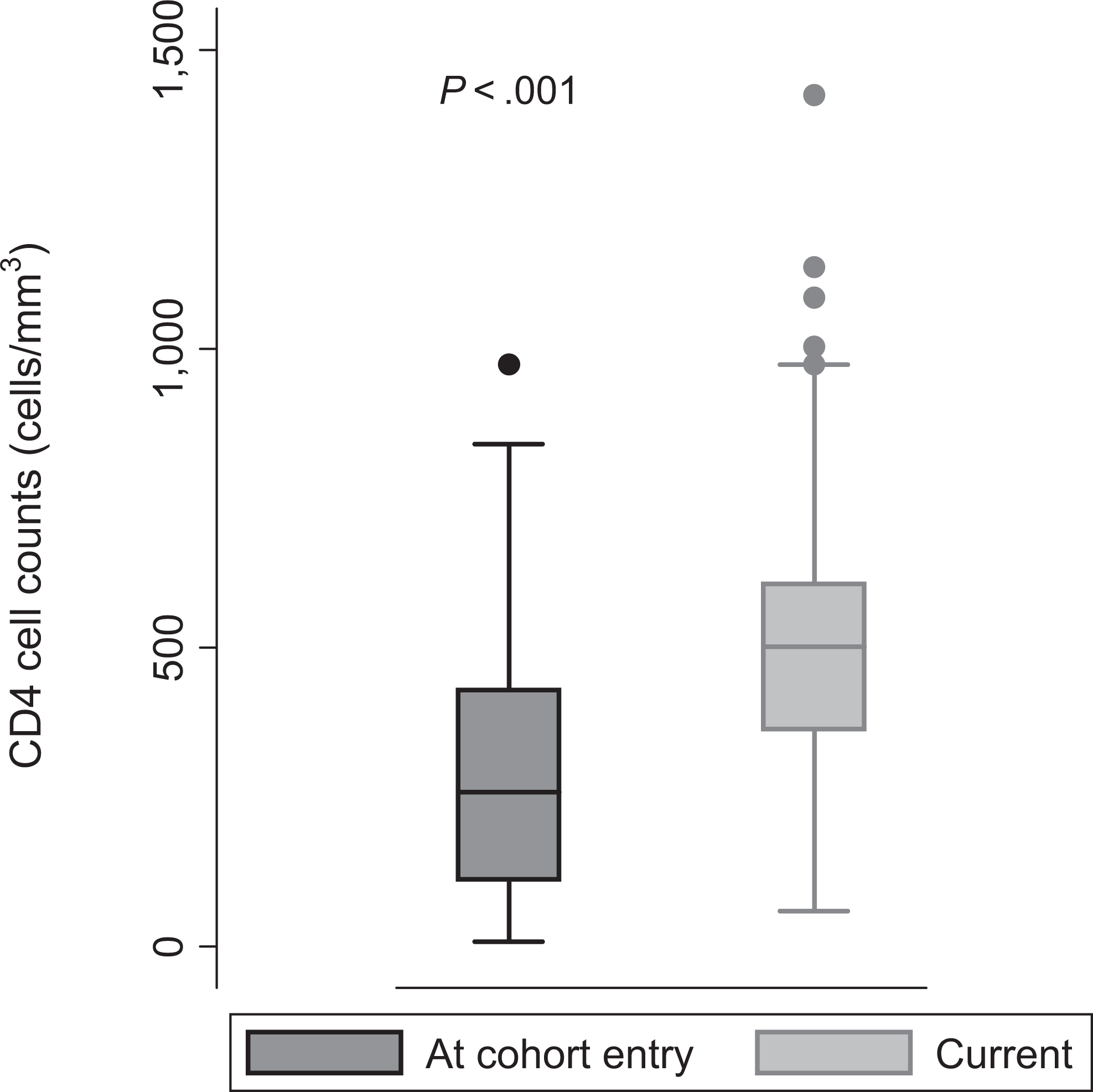
Distribution of CD4 counts at cohort entry and current CD4 counts

Distribution of HIV RNA at cohort entry and current
A total of 36 (27.9%) patients experienced HIV drug resistance, and 35 (27.1%) patients experienced at least 1 hospitalization. By univariate logistic regression, only CDC stage at cohort entry (OR 1.20, 95% CI 1.02, 1.41, P = .029) was associated with hospitalization. According to the current laboratory results, 76 (58.9%) patients had at least 1 lipid value abnormality (total cholesterol, triglyceride, high-density lipoprotein cholesterol [HDL-C], and high-density lipoprotein cholesterol [LDL-C), 45 (34.9%) patients had creatinine >1.0 mg/dL, and 7 (5.4%) patients had glucose level >126 mg/dL. Overall, 90 (69.8%) patients had at least one of these metabolic laboratory value abnormalities. Changes in metabolic parameters are shown in Table 2. By multivariate logistic regression, male gender (OR 3.96; 95% CI 1.37, 11.39, P = .011) and any metabolic laboratory value abnormalities at cohort entry (OR 2.85; 95% CI 1.01, 8.07, p=0.048) were associated with the current metabolic laboratory value abnormalities.
Metabolic Laboratory Values among 129 Patients with a Diagnosis of HIV Infection for More Than 10 Years

Abbreviations: IQR, interquartile range; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol.
Discussion
To the best of our knowledge, we believe that this study conducted in the HARRT era is one of the longest cohorts of HIV-infected patients in developing countries. Approximately 50% of the HIV-infected patients were men with the mean age of 33 years at diagnosis. We demonstrated that HIV-infected patients who were currently receiving HAART can survive for more than 10 years after the diagnosis of HIV infection. Furthermore, 21.7% of the patients survived for more than 15 years and the longest duration of survival in our cohort was over 20 years.
During the long-term survival period, we found a favorable outcome of HIV treatment, both immunological and virological responses, as that in the previous report among Thai patients, with and without tuberculosis coinfection, who initiated HAART. 13 Cumulative incidence of HIV drug resistance in this study was much higher compared to that of the first-line regimen in Thai patients, which is approximately 3% to 10%. 13,14 This may be explained by much longer follow-up time. The current median CD4 counts of our patients was quite high and roughly 50% of the patients has CD4 counts more than 500 cells/mm 3 , with the significant change from cohort entry. Overall, our patients could achieve the objectives of HAART even in a resource-limited setting which included restoration of immunological response with maximal duration of HIV RNA suppression. 15
In Thailand, there was a shift in the pattern of ART for more than a decade, due to the availability of drugs. The reasons that PI-based regimen and NRTI-based regimen were mainly used as first-line regimen were: 1) zidovudine (ZDV) was the first drug available in Thailand around 1989, and 2) PIs have been available in Thailand since 1998 which is 2 years earlier than NNRTIs. The proportion of HIV-infected patients using NNRTI-based regimens for the current regimen increased significantly overtime. This is because a generic, low-cost, fixed-dose combination pill of stavudine (d4T), lamivudine (3TC), and nevirapine (NVP) has been widely used for scaling up HIV/AIDS treatment as HAART since 2002. 16 In addition, the cost of NNRTI-based regimen is much cheaper in Thailand and other developing countries. Less than 10% of our patients still took the same ART regimen as that at cohort entry. Moderate rate of change or discontinuation of ART was also reported in western Kenya, which primarily was due to drug toxicity, older age, and advanced disease. 17
With improved survival, morbidity and mortality among HIV-infected patients in care has shifted away from opportunistic illness toward an array of other, often chronic, medical conditions. 1 All the ARV drugs have their own adverse effects that can range from mild to life-threatening severity and from immediate to long-term toxicity. In this study, during the long-term period of HIV infection with HAART, we commonly found adverse events associated with chronic medical condition, especially metabolic laboratory value abnormalities such as lipid and glucose level. This fact has raised the concern that HIV-infected patients in the long term may be at increased risk of metabolic diseases or cardiovascular disease, as has recently been described in previous studies. 9,10,18 –20
We acknowledge the limitations of the study. There were some missing data and this was not unexpected in view of the nature of a retrospective study with long duration of follow-up. Second, it was a small sample size study, which might affect statistical analysis. Third, we did a cross-sectional study and enrolled patients who were still followed up at the clinic, which might lead to survival bias. Last, the study was conducted in a university hospital setting, which might not reflect the whole picture of the HIV/AIDS situation in Thailand and/or other resource-limited settings. Generalization of the results to other settings should be considered carefully in view of different characteristics of the populations, medical practices, and infrastructures.
In conclusion, favorable treatment outcomes for HIV treatment, both immunological and virological responses, can be achieved even in a resource-limited setting. Nevertheless, adverse events, such as HIV drug resistance, hospitalization, and metabolic laboratory value abnormalities are quite common among patients with a diagnosis of HIV infection for more than 10 years. Preparation for monitoring and management of these adverse events is a crucial part of successful long-term HIV care.
Footnotes
Acknowledgments
The authors would like to thank the staff of the Department of Medicine, Faculty of Medicine Ramathibodi Hospital, Mahidol University, for taking care of the patients. Assistance from the medical chart service staff is duly noted.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.