
Abstract
This cross-sectional study approached emergency department (ED) patients after the treating physician’s disposition decision to measure patient understanding of whether or not they had received an HIV test during their ED encounter. Of the 300 respondents, 24 were excluded due to missing data or because they had received an ED HIV test. Mean age was 41 years, 51% were men, 61% were black, and 29% had no high school degree. There were 5.8% (95% confidence interval: 3.5%-9.4%) who erroneously reported HIV test delivery during their ED course. Our results suggest a small but significant minority of patients falsely assume that they have been tested for HIV during their ED visit. This misperception could have broad implications, leading to less frequent subsequent testing, false reassurance of HIV-negative status, and inaccuracies in surveillance estimates or surveys that depend on self-report.
Introduction
Successfully screening the US population for HIV infection is an urgent priority for individual and public health. 1 It is important for individuals to know whether or not they have been tested for HIV. Prior testing history is a logical determinant of future testing 1 -3 and an important metric in public health surveillance. 4 Error could occur in these processes if patients believe themselves to have been tested when they have not been. Patients may also engage in risky behavior differently depending on their testing history. Of particular concern would be individuals who are unknowingly HIV positive but gain false reassurance from the erroneous presumption that they were tested and found to be HIV negative.
Anecdotally, patients occasionally report to us that “everything is okay,” including their HIV status, after a medical encounter in which they are not told otherwise. This misperception is plausible, given pervasive deficiencies in health literacy with inherent confusion about medical terminology 5 and discrepancies between self-reported and perceived risk. 6 -12 However, differences between the health care that patients have actually received and care that they believe they have received have not been well explored. To our knowledge, it is unknown whether there is a significant proportion of patients who believe they have received an HIV test during a clinical encounter even though they have not.
We estimated the proportion of patients in our emergency department (ED) who report receiving an HIV test during their ED course when in fact they did not. We place this in context of the patient characteristics, knowledge, and intensity of the ED services received.
Methods
Study Design
This was a cross-sectional survey of a convenience sample of ED patients. Survey data were augmented with review of ED records and/or interview with ED providers to determine the clinical service rendered and verify the accuracy of patient self-reports. The institutional review board approved this study.
Setting
This study was conducted in the ED of an urban, tertiary, referral hospital with an annual ED census of approximately 90 000 patients. Approximately two-thirds of this population is Medicaid or self-pay, 51% are black, 43% are white, and 0.5% are Latino. For over a decade, the ED has housed an HIV counseling and testing program that uses conventional opt-in consent. 13 Patients are identified for testing on a targeted basis or when referred by clinical staff. The test positivity rate is approximately 0.7%. The program tests between 5% and 10% of the overall ED patient population annually.
Selection of Participants
Patients were identified for inclusion at the time of disposition by the treating physician. Purposive sampling was used to balance the number of patients being discharged and the number being admitted. Recruitment occurred during periods when the counselor-supported ED screening program was not in operation. During such periods, providers may discuss and/or offer HIV testing without the help of counselors, although this is uncommon. Patients were excluded if they did not have capacity for consent or were not aged between 18 and 64 years. Refusal rate was not recorded. Surveyed patients who were later found to have been tested for HIV during their course of ED care were excluded from the analysis.
Methods and Measurements
Patients were asked a series of questions on demographics, risk factors for HIV, knowledge of HIV, and which medical services they recalled receiving during their ED visit. Questions involving HIV were embedded among non-HIV-related questions and ordered so that the question about HIV test receipt occurred at the end; the survey instrument is shown in Figure 1. Immediately after survey administration, the patients’ responses about which medical services had been received were confirmed through review of patient records or discussion with medical staff.

Survey instrument.
Outcome Measures
The primary outcome measurement was whether or not the participant reported receiving an HIV test in the ED. Secondary outcomes included accuracy of patient reports of receiving medical imaging or venipuncture and self-reported HIV risks.
Primary Data Analysis
Analysis was descriptive in nature. Study data were entered and managed using REDCap (Vanderbilt University, Nashville, Tennessee). All analyses were conducted using SPSS 18.0 for Windows (SPSS Inc, Chicago, Illinois).
Results
Three hundred patients were surveyed from June through July 2010. One patient had missing information on HIV testing and was excluded from the analysis. Of the remaining 299 patients, 23 (8%) were tested for HIV during the visit and were excluded from this analysis. A total of 276 patients were included. The mean age was 41 years (standard deviation = 13 years); 144 (52%) of the 276 were men, 164 (59%) of 276 were black, and 78 (28%) of 276 reported less than a high school education (Table 1). Overall, 22 (8%) of the 276 patients reported risk factors for HIV.
Patient Characteristics and Perceptions of HIV Testing.a
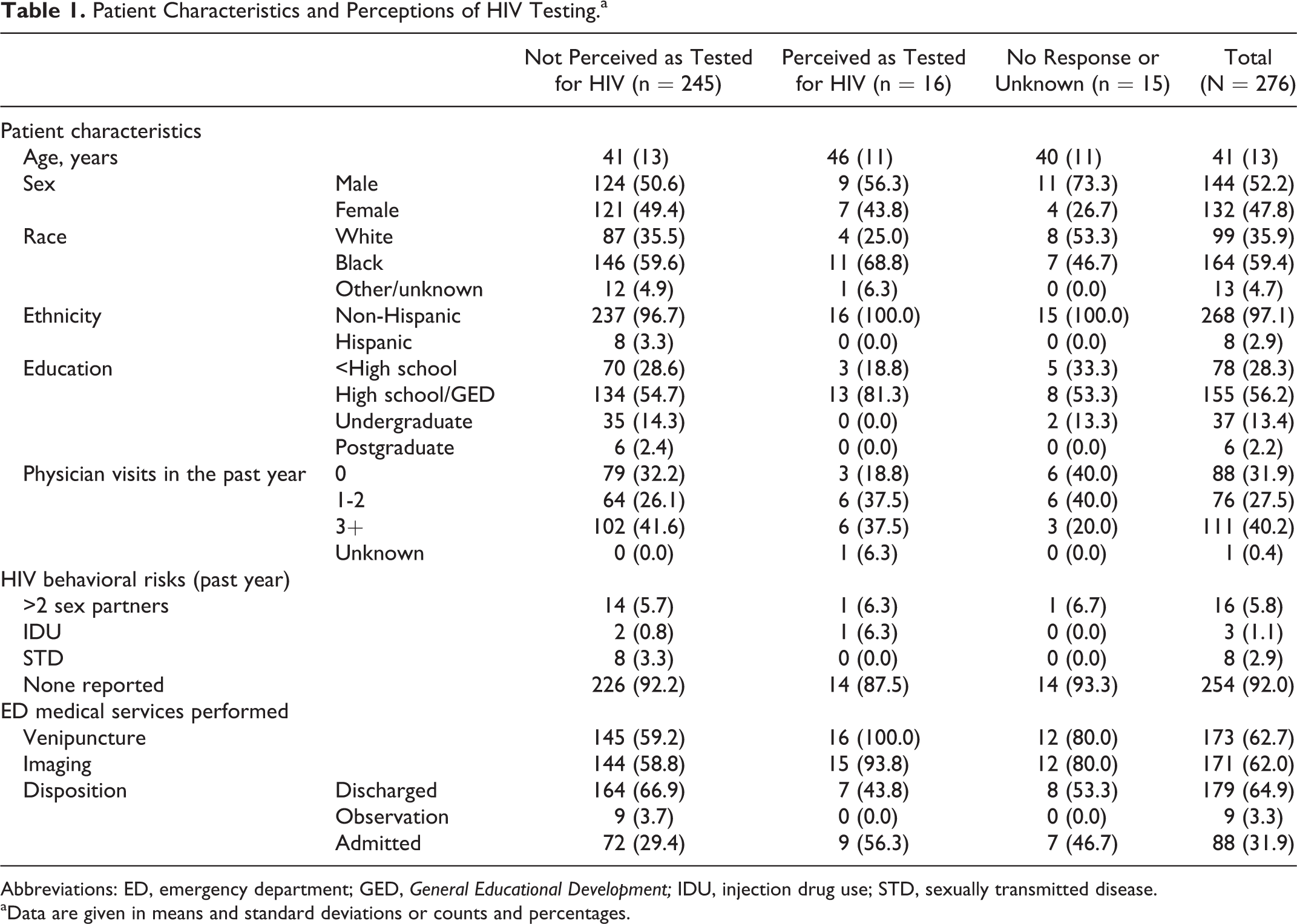
Abbreviations: ED, emergency department; GED, General Educational Development; IDU, injection drug use; STD, sexually transmitted disease.
aData are given in means and standard deviations or counts and percentages.
Of the 276 patients, 16 reported having received HIV testing (6%; 95% confidence interval: 4%-9%). Another 15 (5%) of 276 stated that they did not know whether an HIV test was performed, and 245 (89%) of 276 correctly stated that they were not tested for HIV during this visit. For context, 162 (95%) of 171 patients correctly reported they received imaging, 12 (11%) of 105 reported receiving imaging when they had not, 9 (5.3%) of 171 reported not receiving imaging when they had, and 93 (89%) of 105 correctly reported not receiving any imaging; 3 (1%) of 276 participants stated that they did not know whether imaging was performed. Similarly, when asked whether blood was drawn on this visit, 157 (91%) of 173 patients correctly reported receiving a blood draw, 16 (9%) of 173 reported not receiving a blood draw when they had, 14 (14%) of 103 reported receiving a blood draw when they had not, and 89 (86%) of 103 correctly reported not receiving a blood draw.
All 16 patients who incorrectly believed that HIV testing had been performed had a blood draw during the visit, and 15 (94%) of 16 also had imaging performed. Of these patients, 9 (56%) of 16 were admitted, compared to 72 (29%) of 276 of those who correctly reported no HIV testing. In addition, 16 (100%) of the 16 patients who incorrectly believed that HIV testing had been performed had a high school education or less, while among those correctly reporting they did not receive an HIV test, 70 (29%) of 245 had a high school education or less.
Limitations
In our study, 1 in 20 patients incorrectly believed they had an HIV test during their ED stay when they had not. This finding should be interpreted in the context of several limitations. The generalizability of our estimate depends on the degree to which the convenience sample represents the ED population as a whole. Moreover, our ED may not be generalizable to other settings. Our ED houses an HIV screening program utilizing a conventional consent process and formal HIV prevention counseling that has been operational for over a decade. The surveyed population is more likely to have been tested previously with formal notification and consent than is the case at EDs with no HIV testing program. This would tend to bias our sample toward more accurate perception of whether ED testing occurred but may also have led to a stronger than usual perception that the ED provides HIV testing. If so, this would bias our results toward a lower frequency of misperceived testing.
The survey instrument was not validated, and we cannot exclude the possibility that patients misunderstood the questions they were asked. Also, as risks were self-reported, collected data were subject to recall and response biases. We have not attempted statistical testing; not only was the study designed as a descriptive exploration, small sample sizes would limit our ability to explore associations between patient characteristics and responses with statistical rigor.
Discussion
Our study shows that a small but significant minority of ED patients falsely assume that they have been tested for HIV during their ED visit. A similar number are unsure they have been tested and may be prone to considering their prior testing history in a manner similar to those who believe inaccurately that they have been tested in the ED. Patients who have been recently tested for HIV are less likely to seek testing and less likely to consent to testing if it is offered in the future. 1 -3 Similarly, providers are presumed to be less likely to offer testing to a patient who self-reports a recent prior test. The consequence of an individual believing they have been tested when in fact they have not, then, is a reduced likelihood of future testing. The proportion of persons may be small, and the rate of positivity among these persons smaller still, but the cost of missed diagnoses are high. Beyond individual health and health systems affects, public health surveillance measures include the proportion of those who have ever been tested for HIV and portion tested in the past year. 1 Our results suggest that inaccuracies would be introduced when these metrics depend on self-report.
Other researchers have suggested that patients show a small increase in risky behavior after receiving a negative HIV test result, possibly believing that there are no negative consequences of prior at-risk behavior 4 or that ongoing at-risk behavior is free of risk. This inappropriate reassurance is even more troubling if the patient was not in fact tested. The impact of our results is pressing even if 1 patient who misperceived that they had an HIV test with negative results was, in fact, unknowingly HIV positive. Many HIV infections go undetected, but we contend that being undetected and believing that one’s serostatus is known to be negative is particularly concerning.
Beyond various health effects, inaccurate recall of HIV test receipt has policy implications for informed consent. Conventional consent for HIV testing is associated with a number of protections to ensure that individuals are informed and willing to engage in testing. Even the current US Centers for Disease Control and Prevention recommendations are consistent with a level of consent protection that goes beyond many usual medical tests. For example, HIV testing still requires that the patient be aware of the test and their right to refuse. Patients who assumed they were tested when they had not might be accepting of an opt-out approach to HIV testing. If a significant proportion of the remaining population feels similarly, then the need for exceptionalism in HIV testing may continue to wane. Alternatively, our results might prompt some to argue for a renewed emphasis on explicit consent methods to ensure that patients know with certainty whether they have been offered a test and whether or not they have accepted it. Regardless of the consent mechanism used, our data show that there is a need for patients to better understand the services they have received during a given ED encounter so that they are able to act on truth, not perception.
It is concerning, but not unexpected, that patients often misunderstand the medical care they have received. In our study, patients who falsely perceived they had been tested frequently had low educational levels and were minorities known to be at risk of decreased health literacy. 14,15 The extent to which diminished health literacy is associated with inaccurate perceptions of clinical services provided during an encounter is not well elucidated, but this may contribute to our findings. Misperceptions may also be exaggerated in the ED setting due to the acuity of illness, the pace of activity, and the number of tests being run in parallel. In our study, all patients who misperceived receiving an HIV test received a relatively intensive ED evaluation including venipuncture and in most cases medical imaging. This suggests that receiving 1 medical service might influence the perception of receiving other medical services. It is possible that patients are equating blood sampling for the purpose of evaluating an existing complaint with comprehensive screening for disease, including for HIV. This possibility is consistent with our prior study showing that in women undergoing a pelvic examination to diagnose a current complaint, there was a common misperception that they had also received a pap smear. 5 The implication is that patients may believe that evaluation for 1 complaint entails comprehensive evaluation for all possible complaints. This notion warrants further study as the consequences to individual health behavior may be significant.
Conclusion
A small but significant minority of ED patients believe that they have been tested for HIV during their ED visit when they have not. This misperception could lead patients to seek or accept testing less frequently, mistakenly assume they are HIV negative, and provide inaccurate self-report when surveyed for surveillance estimates. When screening itself is not possible, informing patients that no prevention measures occurred during the visit might avert inappropriate behavior. Beyond HIV testing, there is a need to address patient misperceptions about the provision of prevention and screening during a health encounter; reducing such misperceptions could benefit both individual and public health by eliminating false reassurance and consequent behavior change.
Footnotes
Authors’ Note
Results of this study were presented in a poster session at the 2010 National Summit on HIV Diagnosis, Prevention and Access to Care on November 18, 2010.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded in part by the National Institute for Allergy and Infectious Disease (K23 AI068453) and by an Institutional Clinical and Translational Science Award, NIH/NCRR Grant Number 5UL1RR026314-02.