
Abstract
Postnatal depression (PND) is a major problem in low- and middle-income countries (LMICs). A total of 210 postpartum mothers attending primary care urban clinics were screened for PND at 6 weeks postpartum using the Edinburgh Postnatal Depression Scale (EPDS) and Diagnostic and Statistical Manual of Mental Disorders (Fourth Edition; DSM-IV) criteria for major depression. The HIV prevalence was 14.8%. Of the 210 enrolled postpartum mothers, 64 (33%) met DSM IV criteria for depression. Using trained peer counselors, mothers with PND (n = 58) were randomly assigned to either group problem-solving therapy (PST, n = 30) or amitriptyline (n = 28). Of the 58 mothers with PND, 49 (85%) completed 6 weeks of group PST (n = 27) or pharmacotherapy (n = 22). At baseline, the mean EPDS score for participants randomized to group PST was 17.3 (standard deviation [SD] 3.7), while the group randomized to amitriptyline had a mean EPDS score of 17.9 (SD 3.9; P = .581). At 6 weeks postintervention, the drop in mean EPDS score was greater in the PST group (8.22, SD 3.6) compared to the amitriptyline group (10.7, SD 2.7; P = .0097). Group PST using peer counselors is feasible, acceptable, and more effective compared to pharmacotherapy in the treatment of PND. Group PST could be integrated into maternal and child health clinics and preventing mother-to-child transmission of HIV programs in LMICs.
Introduction
Postnatal depression (PND) is highly prevalent in low- and middle-income countries (LMICs) with reported rates ranging from 16% to 35%. 1 –4 The PND can lead to adverse consequences not only on woman but also on her infant, partner, and family. 5 –7 The PND can cause impaired mother–infant interactions and problems in child’s cognitive, behavioral, and emotional development. 8 Recent studies from South Asia indicate that PND is also associated with low birth weight, malnutrition, diarrheal illness, and poor vaccine uptake rates among infants. 9 –11 Data on the burden of PND are limited in Zimbabwe. 2,12 In previous studies conducted in an urban antenatal clinic, we have documented a high burden of psychological morbidity primarily depression among HIV-infected and uninfected women during pregnancy. 2,13,14
Although antidepressants are effective in treating PND, 15 poor access to specialty mental care and antidepressant medications pose a major challenge in LMICs. 5,6 Given these considerations, simple, low-cost psychological interventions to treat PND should be evaluated in LMICs. In recent years, nonpharmacological interventions (eg, group interpersonal psychotherapy and psychoeducational groups) have been shown to be efficacious for depression in Uganda and Chile. 16 –18 However, progress has been slow in implementing cost-effective and feasible interventions to treat PND in LMICs. 5,6,19,20 The objective of this study is to determine the efficacy of group problem-solving therapy (PST) delivered by peer counselors versus pharmacotherapy for PND in a cohort of postpartum HIV-infected and uninfected women attending primary care postnatal clinics in urban Zimbabwe.
Methods
Site and Population
This study was done in 2 urban primary care clinics in Chitungwiza, a periurban community with a population of 1.5 million located on the outskirts of the city of Harare, Zimbabwe. The prevalence of HIV infection among pregnant women was 16% at the time of the study. 21 At both clinics, pregnant women are offered routine (opt-out) HIV testing. 22 A single-dose intrapartum/neonatal nevirapine (NVP) regimen is used to prevent mother-to-child transmission of HIV (PMTCT). 23
The study participants were postpartum women aged 18 years and older who attended the routine postnatal clinic 6 weeks after delivery with her baby aged 6 to 7 weeks and resided within the district. Participants were excluded if they did not reside in the local area, were unable to give informed consent, had psychosis, severe depression, and suicidal ideation.
The study protocol was approved by the institutional review board at the Medical Research Council of Zimbabwe. Permission to conduct the study was obtained from the Chitungwiza Health Department. Written informed consent was obtained from all the participants. This trial is registered at the Pan African Clinical Trial Registry, trial number: PACTR201303000485383.
Measures
All eligible mothers were screened with the 10-item Edinburgh Postnatal Depression scale (EPDS) using trained primary care peer counselors. 14 These peer counselors are people living with HIV/AIDS who provide community education and mobilization for PMTCT in Chitungwiza, Zimbabwe. 24 The EPDS scale has been validated in our setting for screening depression and has sensitivity of 88% and specificity of 87%, with a positive predictive value of 74% and a negative predictive value of 94%. 14 Depression was defined by a cutoff EPDS score of 11 or above. 14 All study participants were subsequently subjected to mental status examination by 2 psychiatrists who were blinded to the participant’s EDPS test results. The diagnosis of postpartum depression was confirmed by Diagnostic and Statistical Manual of Mental Disorders (Fourth Edition; DSM-IV) criteria for major depression. 25
Randomization and Primary Outcome Measure
Postpartum mothers meeting criteria for major depression according to DSM-IV were randomly assigned to group PST (delivered by trained primary care counselors) or pharmacotherapy with amitriptyline using computer-generated random numbers. The duration of treatment was 6 weeks. The primary outcome measure was the EPDS scores after 6 weeks of treatment.
The Group PST Intervention
Group PST was delivered by 6 trained peer counselors in a private setting in the antenatal clinic. Before implementation, peer counselors attended a 2-day training workshop conducted by 2 psychiatrists (DC and WM) on screening “Kufungisisa” (depression in the local language, Shona) using Shona version of the EPDS scale. 14 The peer counselors were HIV-infected women who previously participated in a PMTCT program at our site, currently enrolled in support groups, and had disclosed their positive HIV status to partner or family member.
Originally published by Maynors-Wallis, 26 the efficacy of group PST for treatment of anxiety and depression has been proposed for local use in Zimbabwe using primary health care workers. In our study, group format and content were modeled after a 7-step management plan for depression published by Abbas et al in 1994. 27 The content provided information about symptoms and causes of depression, available treatment options, guidelines on “asking questions,” “listening and talking,” assessment of suicidal risk, involvement of culturally appropriate family members in problem solving, exploring community resources and support systems, and follow-up. 27 All issues were discussed with examples relevant to the postpartum period. Table 1 shows the group PST intervention protocol used for mothers in their postnatal period.
Structure of Group Problem-Solving Therapy Delivered by Primary Care Counselors in Zimbabwea.
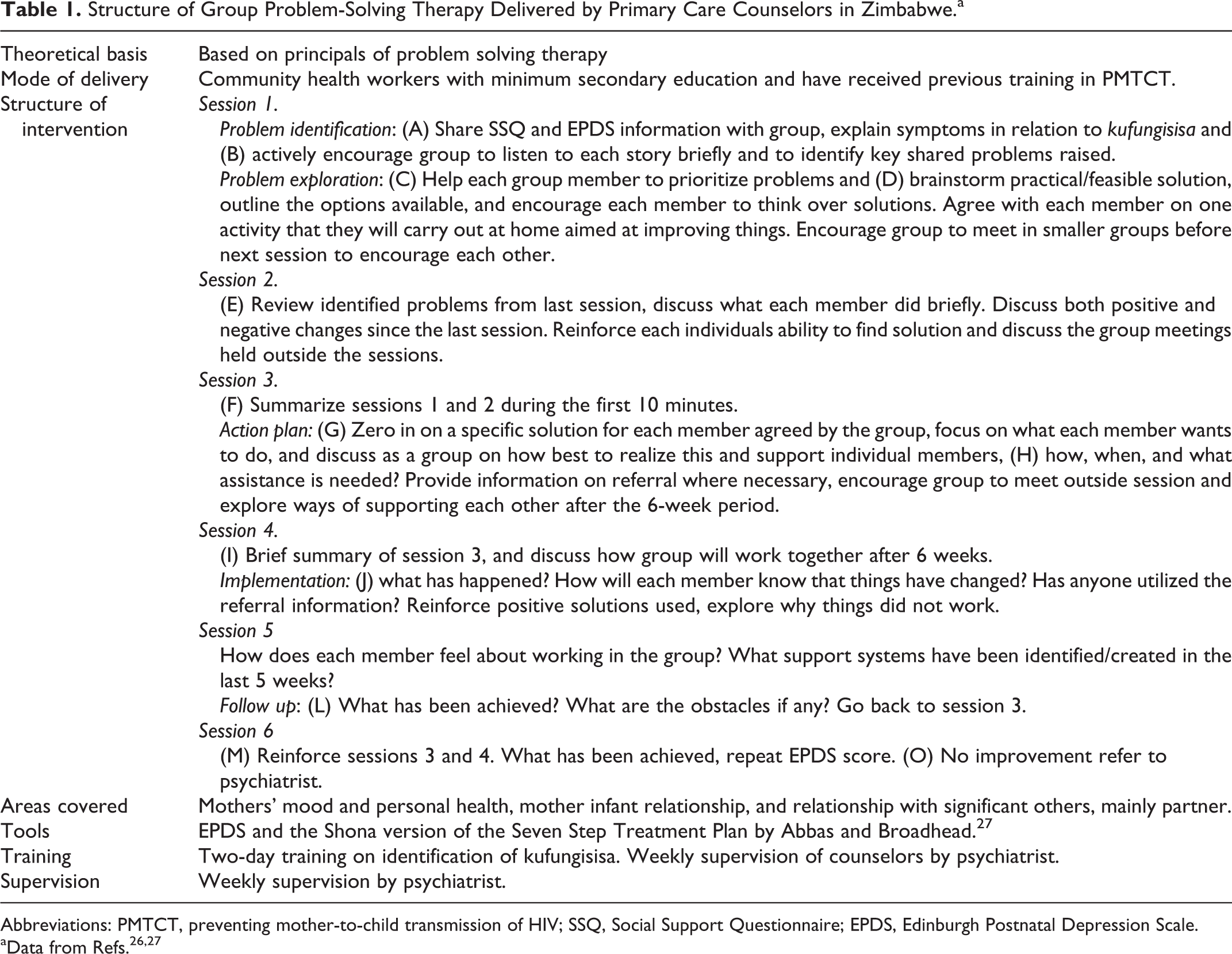
Abbreviations: PMTCT, preventing mother-to-child transmission of HIV; SSQ, Social Support Questionnaire; EPDS, Edinburgh Postnatal Depression Scale.
In all, 3 groups, 2 consisting of 9 mothers and 1 with 10 mothers, were facilitated by 3 peer counselors supervised by the psychiatrist (DC) engaged in the intervention. Each group met twice weekly for 6 weeks, with every session lasting for 60 minutes. Attendance for group sessions was very high (95%); 1 woman had a week of interruption of therapy due to issues with her partner.
The peer counselors met weekly to discuss their experiences and received ongoing supervision and feedback from the psychiatrist (DC). Patients with psychosis, severe depression, and suicidal ideation were referred to a specialized psychiatric unit located at Harare Central Hospital for treatment.
Intervention with Pharmacotherapy
Amitriptyline was prescribed by the primary care nurse as part of her routine clinic work. All women underwent a physical examination including measurement of blood pressure and examination of the cardiovascular system. Women were then informed of the effects of amitriptyline and how it would help in the treatment of kufungisisa (depression). An initial starting dose of 50 mg to be taken at night was provided. Amitriptyline was increased by 25 mg after every 3 days depending on the symptoms. Potential adverse effects of the drug were explained to the study participants. They were advised to visit the clinic nurse every week for evaluation of their progress. The group under the supervision of a peer counselor talked about education on PMTCT including safe breastfeeding practices and the importance of exclusive breastfeeding. Each session lasted 20 to 30 minutes, and they were then given their medication.
Statistical Analysis
The data were analyzed using the SAS Statistical Analysis System, version 9.0 (SAS Institute, Cary, North Carolina). Descriptive statistics (including means, standard deviations [SDs], frequencies, and percentage) were calculated for the sociodemographic variables. Group comparison was performed using chi-square test, t test, and odds ratio (95% confidence interval). Stepwise logistic regression was used to evaluate independent associations. All tests were 2-tailed, and a P value of <.05 was considered statistically significant.
Results
Figure 1 depicts the trial profile. A total of 64 postpartum women met DSM-IV criteria for depression and were enrolled in the study; 6 met criteria for severe depression and were referred to a psychiatric hospital where they were commenced on both antidepressant medication and psychotherapy and excluded from the study.

Trial Profile. PND indicates postnatal depression; PST, problem-solving therapy.
Using trained primary care counselors, mothers with PND (n = 58) were randomized to either group PST (n = 30) or amitriptyline pharmacotherapy (n = 28) for a period of 6 weeks. Of the 58 postpartum mothers who received the intervention, 49 (85%) completed 6 weeks of treatment with group PST (n = 27) or pharmacotherapy (n = 22). Overall, 9 (15%) women were lost to follow-up at 6 weeks including 3 (10%) from group PST and 6 (21%) from the pharmacotherapy group, respectively.
Demographic Characteristics
All study participants were black Zimbabwean women with a mean age of 25 years; 19 (33%) women were primiparous, 39 (67%) women were married, 16 (28%) women were in a cohabiting relationship, and 3 (5%) women were single. All enrolled participants had received some level of education with the majority, 42 (72%), having achieved secondary education. The majority of women, 52 (89%), were unemployed. The demographic and baseline characteristics of the enrolled participants in the group PST and pharmacotherapy group were similar (Table 2).
Characteristics of Enrolled Participants in the Problem-Solving and Pharmacotherapy Groups.

Abbreviations: SD, standard deviation.
HIV Serostatus
Of the 58 mothers with PND, 14 (24%) were HIV positive, 35 (60%) were HIV negative, and 9 (15%) were of unknown serostatus. Of the 6 women with severe depression who were excluded from the study, 3 were HIV positive, 1 was HIV negative, and 2 were of unknown HIV status.
The EPDS Scores (Pre- and Postintervention)
The mean EPDS scores at baseline and postintervention is depicted in Table 3. At baseline, the mean EPDS score for participants randomized to group PST (n = 27) was 17.3 (SD 3.7), while the group randomized to pharmacotherapy with amitriptyline (n = 22) had a mean EPDS score of 17.9 (SD 3.9), and this difference in scores between the 2 groups were not statistically significant (P = .581). In contrast, after the 6-week intervention, the drop in the mean EPDS score was greater in the PST group (8.22, SD 3.6) compared to the pharmacotherapy group (10.7, SD 2.7), and this difference was statistically significant (P = .0097). A descriptive subanalysis regarding the effect of the group PST intervention, stratified by HIV serostatus, did not reveal any statistically significant differences between the 2 groups (Table 4).
Mean EPDS Scores of Participants Receiving Group Therapy versus Pharmacotherapy.
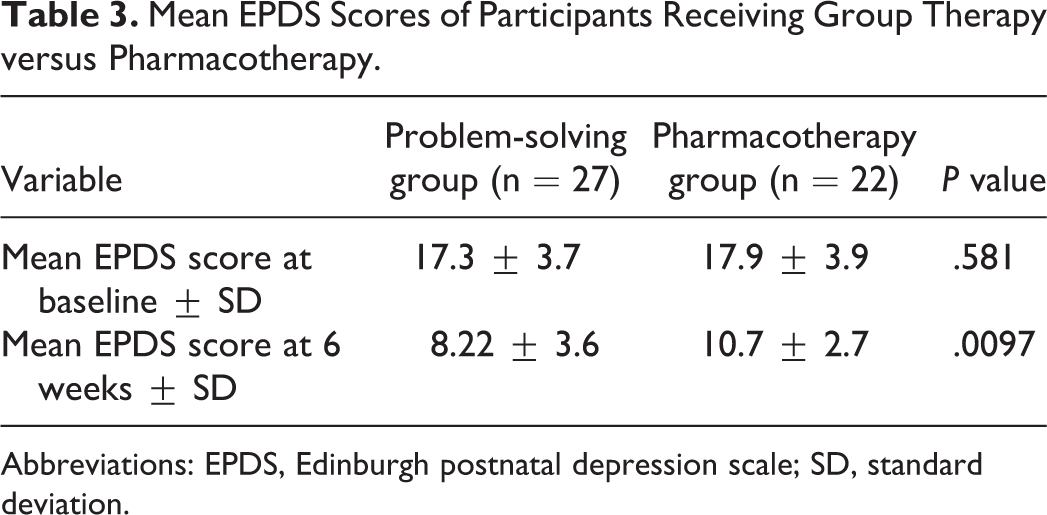
Abbreviations: EPDS, Edinburgh postnatal depression scale; SD, standard deviation.
Effect of Group Psychotherapy Intervention Stratified by HIV Status (n = 26)a.

Abbreviations: EPDS, Edinburgh Postnatal Depression Scale; SD, standard deviation.
aOne participant with unknown HIV status was excluded from the analysis.
Discussion
This preliminary study demonstrated that group PST was more effective than pharmacotherapy in the treatment of PND among women found to be depressed 6 to 8 weeks after childbirth. Our results indicate that primary health care centers in Zimbabwe and other LMICs may consider using primary care counselors to address PND through simple structured “talk therapy.” 28 Since EPDS can be introduced in the primary health care setting to effectively screen and detect antenatal/postnatal depression, 14 it is important to have a cost-effective intervention to address the issue of PND in LMICs. The role of PST in treating depression is well established in the resource-rich settings. 29,30 With the current unavailability and the prohibitively high cost of the standard first-line treatment for depression (eg, amitriptyline) and potential safety concerns regarding the use of antidepressants during pregnancy, group PST (or as it is more casually referred in Chitungwiza—“talk therapy”) can be an effective intervention at minimal cost to the clinic.
In our study, the prevalence of PND was high (33%) compared to other settings likely due to pervasive socioeconomic hardships and political instability in Zimbabwe that has a direct impact on health and service provision. 31 This is further supported by the positive results resulting from the group PST in our study in an attempt to address common sociofamily upheavals being faced by the mothers. Previous studies have indicated that nonspecific factors can influence the outcome of group intervention. 32 The active component of group PST is unclear and warrants further research. 28
Given the high prevalence of perinatal common mental disorders (CMD) in LMICs, randomized controlled trials to study the efficacy and cost effectiveness of psychotherapeutic interventions for PND are warranted. 16 In recent years, a number of randomized controlled trials evaluating group interventions for CMD conducted in LMICs have shown promising results. 17 –20,28 In rural Uganda, group psychotherapy was found to be efficacious in reducing depression and dysfunction. 18 A recent cluster randomized trial from rural Pakistan showed that a cognitive behavioral intervention, adapted to the local setting and delivered by trained community-based health workers, was very effective in treating PND among mothers. 19 The intervention also conferred health benefits for the infants such as improved immunization rates, reduced frequency of diarrhea, and both parents spending more time playing with their infants. 19 In Chile, a psychoeducational group intervention was effective in treating depression in low-income women attending primary care clinics. 20 In a more recent report from South Africa, brief PST in a booklet/workshop format was effective, feasible, and acceptable for deprived individuals with CMD. 28
Our pilot study shows that it is feasible to treat PND in primary care clinics using trained primary care peer counselors. 2 In addition, the psychological intervention was successfully integrated into routine postnatal primary care activities and linked to existing PMTCT program. However, regular and reliable training and supervision are essential for the success of community health worker-based programs. 24 There is a severe shortage of specialized mental health professionals in most LMICs. 33 In one report, Zimbabwe was reported to have fewer than 10 psychiatrists for 10 million individuals. 27 Therefore, strengthening the existing maternal and child health systems to deliver simple low-cost perinatal mental health interventions using existing capacities and programs (such as PMTCT and HIV/AIDS treatment program) is critical in LMICs. 34
Our study has several limitations. The study was conducted in an urban setting, so findings are most likely not generalized to the rural population of new mothers. Our study is also limited by a relatively small sample size. The study design was not rigorous to demonstrate effectiveness of the 2 interventions, and there was no long-term follow-up. It is possible that the improvement in depressive symptoms after group PST may have resulted from spontaneous remission, although most of our participants presented with recent life events as triggers that were discussed within the context of the group PST. Finally, the peer counselors who screened mothers for PND in our setting were highly motivated, well trained, and received supervision.
Given the high prevalence of PND in our setting, we recommend that screening for PND and provision of group PST should be part of routine perinatal care in Zimbabwe. A recent study from urban Zimbabwe found that locally adapted PST delivered by primary health care workers can alleviate symptoms of depression and CMD. 35 The role of task shifting using primary care counselors in the detection and management of PND in LMICs must be explored in larger studies. Our study provides useful pilot data in preparation for future research in this field. Future randomized controlled trials should evaluate the efficacy of low-cost interventions such as group PST in treating PND in LMICs.
Footnotes
Authors’ Note
The project was reviewed by Institutional Review Board and Human Subjects Committees at University of Zimbabwe College of Health Sciences, and Wake Forest School of Medicine, Winston-Salem, NC, USA
Acknowledgments
The authors wish to thank Dr Micah Simoyi (Chitungwiza Health Department, ZW), nursing staff and peer counselors (Seke North and St Mary’s clinics, Chitungwiza, ZW), UZ-UCSF Collaborative Program in Women's Health, Departments of Psychiatry, Pediatrics and Community Medicine, University of Zimbabwe, Zimbabwe Ministry of Health and Child Welfare, and all the mothers who participated in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.