
Abstract
The purpose of this study was to evaluate the prevalence of depressive symptoms and associated variables among people living with HIV/AIDS (PLWHA) in a specialized treatment center in a city located in southern Brazil. A cross-sectional study was conducted using the Beck Depression Inventory to assess the presence of depressive symptoms. The prevalence of depressive symptoms was 53.5% among the surveyed population, which supports the idea that depressive symptoms are more common among PLWHA, mainly if compared with the general population. It was observed that 57.7% of the study participants were with depressive symptoms and did not take any psychiatric medication and 100% did not undergo psychotherapy, which indicates undertreatment. There was no statistically significant difference in the mean CD4 count between patients with depressive symptoms (484.1 ± 353) and patients without depressive symptoms (528.4 ± 263). Further actions should be taken to improve the care for PLWHA. The interface between psychology, psychiatry, and internal medicine is of utmost importance to provide a more humanized care, in which the psychosocial, psychological, and psychiatric aspects are not neglected.
Introduction
The estimated prevalence of major depressive disorder in the general population is approximately 10% to 25% for women and from 5% to 12% for men. Projections indicate that by the year 2020, major depression will be the second largest cause of disability and death worldwide. 1
Epidemiological studies of depression in clinical diseases are even more worrying, since depression occurs frequently among patients with diabetic patients, 2 after acute myocardial infarction, 3 and in individuals with cancer. 4 Prevalence rates of depression in PLWHA vary between 20% and 79%, depending on the population studied, the period investigated, and the tools used to define the patients. 5 –7 The assessment of depression symptoms in individuals living with HIV/AIDS must be done carefully and should take into account the stages of the disease, because some debilitating physical symptoms can fudge depression indicators. 8 Likewise, attention should be paid to the fact that some antiretroviral (ARV) drugs can cause symptoms similar to those found in depression. 9 There is also the HIV-associated dementia that may be misdiagnosed as depression, so the differential diagnosis must be performed. 10,11
This study aimed to assess the prevalence of depressive symptoms among PLWHA and the factors associated with this condition.
Methods
A cross-sectional study was conducted between March and May 2011 in a reference service assisting PLWHA in a city in Southern Brazil. The study enrolled patients aged 18 years or older who were living with HIV/AIDS. Those who had a diagnosis of dementia and those who did not agree to participate by signing the consent form were excluded. The Mini-Mental State Examination was used for dementia detection. 12 A questionnaire was administered to detect the abuse of alcohol or drugs, 1 and the Beck Depression Inventory (BDI) was used to assess the presence of depressive symptoms. 13
For the collection of other variables, the medical records of patients were consulted on the day of blood collection for CD4 count and viral load determination in peripheral blood. The variables studied included the degree of depressive symptoms (minimal, mild, moderate, and severe), gender, age, ethnicity, household income, educational level of participants, time elapsed since HIV diagnosis, CD4 count in peripheral blood, beginning of ARV treatment, disease stage, continuous use of psychiatric medications, and others.
The research project was submitted to and approved by the Human Research Ethics Committee at the University of Southern Santa Catarina (UNISUL, Brazil) under the code number 11.067.4.01.III.
The results were summarized as absolute numbers and percentages and means and standard deviations (SDs), and the independent variables were compared between individuals with depressive symptoms and individuals without them, using the chi-square test at the 5% significance level.
Results
In total, 249 individuals attended for a CD4 count and viral load measurement during the surveyed period, of whom 212 agreed to participate. From these, 9 patients were excluded, because they had dementia, accounting for a 4.2% loss (Figure 1).

Flowchart showing the number of people surveyed and exclusions. The data compiled by author.
The age of participants ranged between 18 and 74 years, mean age was 42.4 (SD ± 11.1) years, 109 (53.7%) were male, and 167 (82.3%) were caucasians. With regard to marital status, 66 (32.5%) were married, 12 (5.9%) were divorced, 8 (3.9%) informed that they were separated, 99 (48.8%) were single, and 17 (8.4%) were widowed. Marital status was not reported by 1 (0.5%) participant. With regard to household income, 31 (15.2%) reported an income less than a minimum wage (US$ 334), 135 (66.5%) said they earned between 1 and 3 minimum wages, and 30 (14.8%) earned more than 3 minimum wages. Most participants (32.5%) had incomplete primary education.
In all, 26 (12.8%) participants had CD4 count lower than 200 cells/mm3 and 177 (87.2%) had a count ≥200 cells/mm3. CD4 count ranged from 21 to 2493 cells/mm3, with a mean of 507 cells/mm3 (SD ± 314.7). With regard to the viral load, 129 (63.5%) participants had a viral load ≤50 copies/mL, and 74 (36.5%) had a viral load greater than 50 copies/mL. Viral load count ranged from 50 to 397 946 copies/mL, with a mean of 11 017.6 (SD ± 40 377.7) copies/mL.
With regard to the time elapsed since HIV diagnosis, the length ranged from 1 to 26 years, with a mean length of 7.2 years (SD ± 5.4). Regarding the disease stage, 93 (45.8%) were in stage 1 of the disease, 84 (41.4%) were in stage 2, and 26 (12.8%) were in stage 3. In all, 154 (75.9%) participants reported that they were taking antiretroviral therapy (ART). The length of time under treatment ranged from 1 to 20 years, with a mean of 5.9 years (SD ± 4.4). Regarding the symptoms indicative of depression as assessed by BDI, 109 (53.7%) participants were classified with depressive symptoms, and 94 (46.3%) as without them. The BDI scores ranged between 0 and 52, with a mean score of 16.6 (SD ± 14). The distribution of the participants according to the BDI scores is shown in Table 1.
Distribution of the Study Participants According to BDI Scores.

Abbreviation: BDI, Beck Depression Inventory.
With regard to the use of psychiatric medications, 146 (71.9%) participants did not use any of them. None of the surveyed patients reported that they were undergoing some type of psychotherapy. In relation to psychoactive drug abuse, 27 (13.3%) patients fulfilled the criteria for substance abuse. With respect to other medications, 127 (62.6%) patients did not use any medications, 73 (36%) used some, and 3 (1.5%) did not respond.
Table 2 shows the distribution of data according to the presence or absence of depressive symptoms.
Distribution of Variables According to the Presence or Absence of Depressive Symptoms.
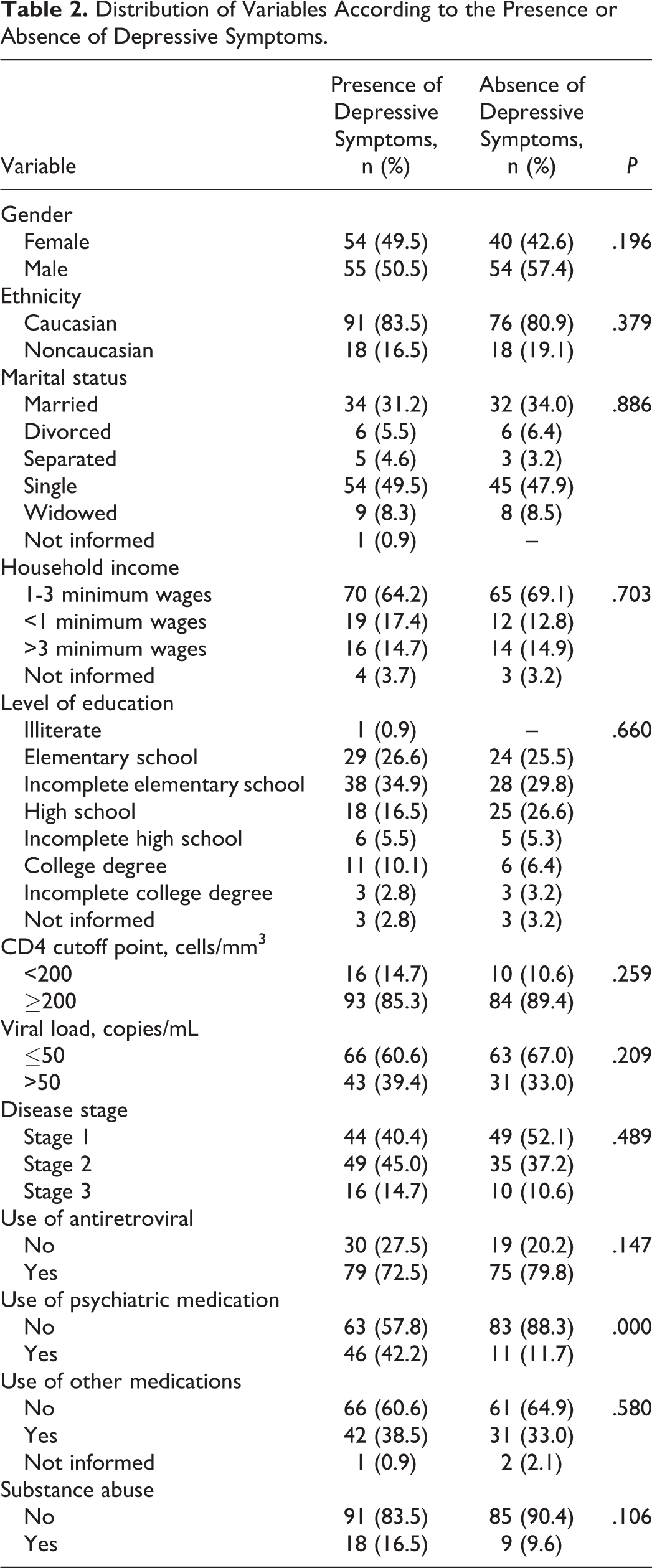
There was no statistically significant difference in the mean CD4 count between patients with depressive symptoms (484.1 ± 353) and patients without depressive symptoms (528.4 ± 263; P = .160).
Tables 3 and 4 show the distribution of the participants according to the use of ARV therapy, viral load, TCD4 count, and the presence or absence of depressive symptoms.
Distribution of Participants According to the Use of ARV, Viral Load, and the Presence or Absence of Depressive Symptoms.

Abbreviation: ARV, antiretroviral.
a P = .441.
b P = .815.
Distribution of Participants According to the Use of ARV, TCD4 Counts, and the Presence or Absence of Depressive Symptoms.

Abbreviation: ARV, antiretroviral.
a P = .492.
b P = .159.
Discussion
Prevalence of depressive symptoms in this population was found to be 53.5%, which supports the idea that depression is more common in PLWHA, mainly if compared with the general population. The prevalence of depression in PLWHA ranges from 20% to 79%. According to several studies, this difference can often be attributed to the population studied, surveyed period, and tools used to identify cases of depression. 5,7
In this study, there was no statistically significant association between the presence of depressive symptoms and gender. Epidemiological data in the general population show that depression is more common in women than in men. 1,14 Justo and Calil 15 hypothesize that the causes for this difference can be related to hormonal and sociocultural aspects. No data were found in the literature that discussed the possible causes for the differences in findings in this specific population compared to those found in the general population. Perhaps in this case, living with HIV/AIDS could have an equal impact on the triggering of depressive episode, both in men and in women.
If we compare the higher rates of depression in individuals with other clinical pathologies than in those living with HIV/AIDS, we will also see that the former is significantly more numerous than the latter. High rates of depression are observed in diabetic patients, 2 in patients with postmyocardial infarction, 3 and in persons with cancer. 4 So, it is evident that the diagnostic investigation of depression in people with HIV/AIDS should not be neglected.
There are studies showing that depression is a risk factor for nonadherence to ART and that antidepressant treatment improves adherence rates. As a consequence, the increase in TCD4 is stimulated. 16 –18
All patients diagnosed with depressive disorder should be treated with psychotherapy and/or psychotropic medications, including depression symptoms in PLWHA. 19 In the present study, 57.8% of the patients with depression symptoms neither used psychiatric medication nor underwent psychotherapy.
In this study, no statistically significant differences were found in TCD4 counts and viral load between individuals with depressive symptoms and individuals without them. Published studies are controversial when examining these conditions. Some authors report that patients with lower TCD4 counts have a higher percentage of depression 17,20 ; however, Lyketsos et al did not observe this finding. 21
Studies show that ART increases TCD4 counts, 17 and most (76%) individuals in this study were taking ARV drugs. However, the present study found no statistically significant difference between individuals with depressive symptoms and individuals without them, even when examining TCD4 counts in participants who were not receiving ART. Although there are reports of higher evolution in disease progression among depressed patients, 17,22,23 in this study there was no association between the disease stage and the use of ART in patients with and without depressive symptoms. This was a cross-sectional study, which generates, by definition, just 1 observation. Cohort studies and control confounding variables could contribute better to the elucidation of these controversies.
In this study, there was no association between these variables ethnicity, marital status, household income, education, and presence or absence of depressive symptoms. Research evaluating the prevalence of depression and associated characteristics in the general population, 24 and PLWHA, 25 did not show an association between these variables and the presence or absence of depression.
Time elapsed since HIV/AIDS diagnosis was not significant for increasing the prevalence of depressive symptoms. Assessment of predicting factors for depression in PLWHA showed that the incidence of depression in individuals who had a psychiatric history prior to infection, particularly a history of depression, and HIV-related symptoms, independently of the time elapsed since diagnosis, was higher than in other groups. 20
In epidemiological studies performed with drug addicts in the general population, there are significant prevalence rates of other psychiatric disorders. 26 The present study found no statistically significant differences of depressive symptoms between drug users and nonusers. This finding may indicate that individuals, when infected, stop doing drugs. The decrease in cocaine use in individuals after receiving a diagnosis of the disease is described in the literature. 27
In conclusion, further actions should be taken to improve the care for PLWHA. The interface between psychology, psychiatry, and clinical medicine is of utmost importance to provide a more humanized care, in which the psychosocial, psychological, and psychiatric aspects are not neglected.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.