
Abstract
A 44-year-old HIV-infected male, having a low CD4 count, was on antiretroviral therapy for the last 2 months, when he developed a skin rash. He gave a history of solitary unprotected extramarital sexual contact 6 months before onset of the rash. Dermatological examination revealed a bilaterally symmetrical, maculopapular erythematous rash involving the palms, forearms, and neck. He showed a positive sign of Buschke-Ollendorff. In the meanwhile, the CD4 count had improved to 196 cells/mm3 from the previous count of 92 cells/mm3 and the viral load had decreased. Serum venereal disease research laboratory (VDRL) test was reactor at 1:64. He was found to be positive result for treponema pallidum hemagglutination test. Skin biopsy revealed features of secondary syphilis. The rash responded well to a single injection of benzathine penicillin, resulting in the lowering of the VDRL titers. There was no evidence of neurosyphilis. This is a very rare instance of secondary syphilis manifesting as immune reconstitution syndrome in an HIV-positive patient.
Introduction
Coexistence of syphilis and HIV infection can result in several atypical manifestations of syphilis such as increased severity of clinical manifestations, rapid progression to neurosyphilis, sero-negativity, relapse despite adequate treatment, and failure of benzathine penicillin therapy. 1, 2 In HIV-infected patients, the use of antiretroviral therapy (ART) can result in the restoration of the immune responses against opportunistic pathogens, leading to a worsening of opportunistic infections ([OIs] paradoxical) or more commonly unmasking of subclinical infections (unmasking), especially during the first 3 months of therapy. This extensive inflammatory immune response is what is termed as immune reconstitution inflammatory syndrome (IRIS). It is present in about 10% to 40% of patients treated with ART for low CD4 counts. 3 First described in nontuberculous mycobacteria, it has been later described in a lot of conditions such mycobacterial tuberculosis, cryptococcosis, Pneumocystis jiroveci pneumonia, Cytomegalovirus retinitis, Kaposi sarcoma, hepatitis C virus, and hepatitis B virus infections. 4 The authors herein report a rare case of secondary syphilis manifesting as a part of IRIS.
Case Report
A 44-year-old male was diagnosed with HIV while being evaluated for weight loss and fever of 1 month duration. He gave a history of solitary unprotected extramarital sexual contact 4 months prior to the detection of HIV. All initial investigations including venereal disease research laboratory (VDRL) test were negative or within the normal limits. He was started on ART immediately after HIV detection as his CD4 count was 92 cells/mm3. The viral load was 200 000 copies/mL. Two months after he was started on ART, the patient developed a skin rash on the neck, forearms, and palms. The rash was asymptomatic and not accompanied by fever or joint pain. The solitary unprotected extramarital sexual contact 6 months ago was not followed by genital ulcer, urethral discharge, inguinal swelling, or any other associated complaints, and the patient denied any other such contact after this episode. Spouse and children of the patient were both HIV and VDRL negative.
Dermatological examination showed bilaterally symmetrical, lichenoid lesions involving palms, forearms, and neck (Figures 1 and 2). He showed a positive sign of Buschke-Ollendorff. There was no evidence of any hair loss, mucous membrane lesions, lymphadenopathy, arthralgia, or periostitis.

A, Skin lesions over the dorsum of hand and extensors of forearm. B, Close up of lichenoid form of lesions on forearm.
A, Skin lesions on the dorsum of hand. B, Characteristic involvement of the palms by secondary syphilis lesions.
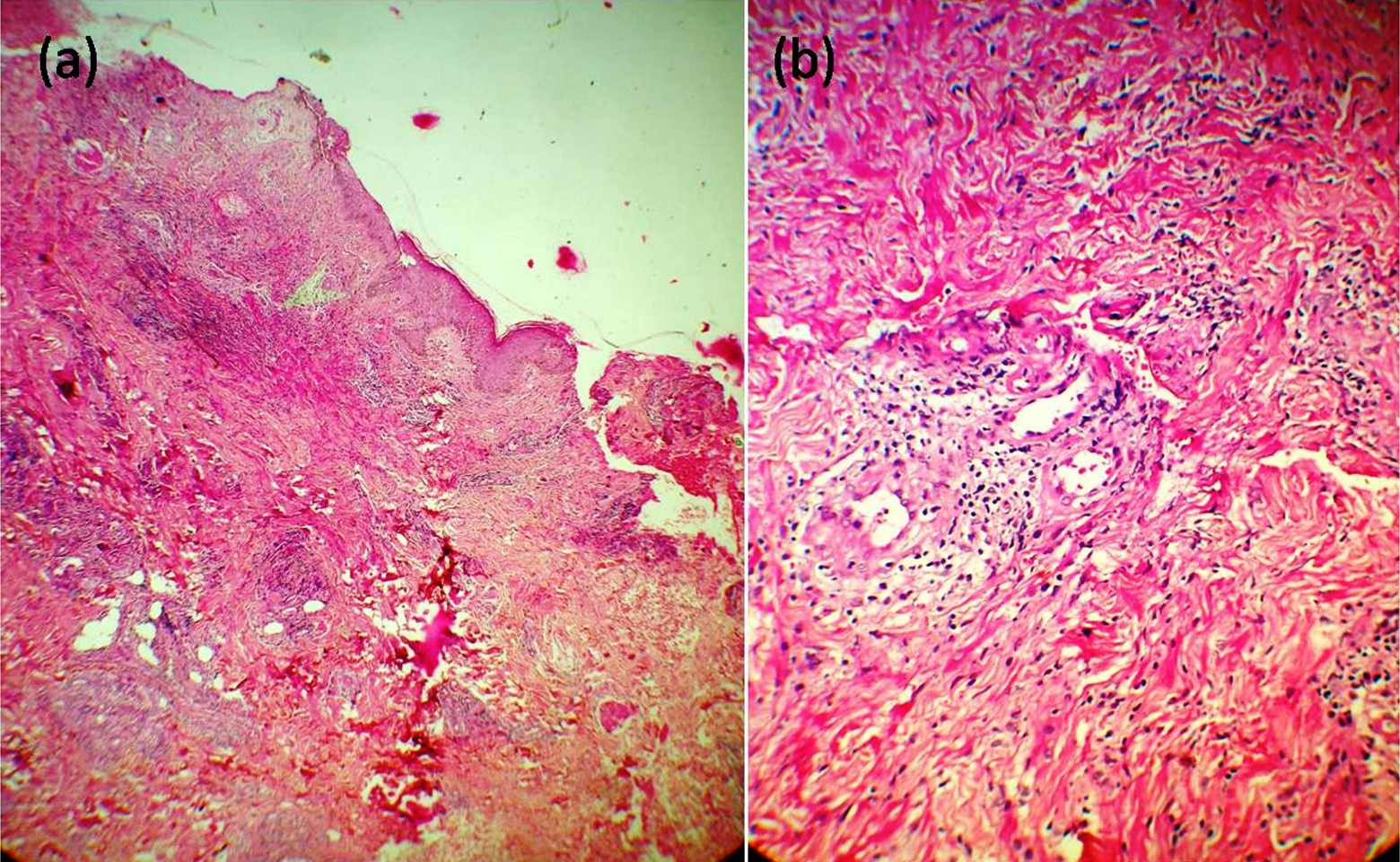
Investigations revealed normal hematological and biochemical parameters. His current CD4 count was 196 cells/mm3 and the viral load was 10 000 copies/mL. Serum was first reported as negative for VDRL. However, when the prozone phenomenon was observed, it was found to be positive at 1:64 dilution. Treponema pallidum hemagglutination (TPHA) test was also found to be positive. Skin biopsy revealed features of acanthosis with psoriasiform hyperplasia, basal cell vacuolation, and perivascular infiltration of lymphocytes and plasma cells along with periadnexal infiltrate which was consistent with secondary syphilis (Figures 3 and 4). Cerebrospinal fluid (CSF) examination was found to be normal with VDRL CSF negativity. Based on the clinical features, skin biopsy, and VDRL report, he was diagnosed with secondary syphilis and managed with a single dose of 2.4 mega units of benzathine penicillin. Skin rash gradually started fading after 2 weeks of therapy and completely regressed in 4 weeks. Serum VDRL test done after 4 months of treatment showed positivity in 1:16 dilution and was negative after 6 months of treatment. The TPHA test continued to remain positive.

Histopathology from the skin lesions showing (A) acanthosis, psoriasiform hyperplasia with granulomatous and perivascular infiltrate in the dermis (hematoxylin and eosin [H&E] stain ×10); (B) neutrophil hidradenitis like periadnexal reaction (H&E stain ×40).

Histopathology from the skin lesions showing (A) perivascular and periadnexal infiltrate (hematoxylin and eosin [H&E] stain ×40x); (B) plasma cell in the center of the field (H&E stain ×100)].
Discussion
Immune reconstitution inflammatory syndrome is defined as abrupt clinical worsening or new presentation of an OI with either a concomitant reduction by at least 1 log of HIV-1 ribonucleic acid (RNA) levels or 2 of the following 3 minor criteria: (a) increase in CD4 count after ART, (b) increase in immune response specific to a pathogen, or (c) spontaneous resolution of the disease. 5 In addition, the definition includes exclusion of conditions due to (i) the expected clinical course of OI after initiation of ART, (ii) drug toxicity, (iii) other infections or inflammatory conditions, (iv) withdrawal of a previously effective treatment modality, and (v) failure of ART. The patient met the above criteria of the definition of IRIS as well as exclusion criteria.
The 4 major risk factors for IRIS are (i) low CD4 count during ART initiation, (ii) high level of virologic and immunologic response to ART, (iii) high antigenic load of specific OI during ART initiation, and (iv) early initiation of ART after an OI. The patient had 2 definite risk factors for the development of IRIS, with a probable high antigenic load.
Secondary syphilis can present as early as 7 days after the primary chancre; but in most cases, it occurs within 4 to 10 weeks. Eighteen percent of men presenting with secondary syphilis may have no history of primary chancre. In this case, the manifestations of secondary syphilis occurred 6 months after the single unprotected sexual contact, with absolutely no history of other contacts in the intervening period. This confirms the unmasking of syphilis in its secondary form by the reconstitution of immunity in the HIV-positive patient after the start of ART. The patient had a lichenoid form of secondary syphilis, which is a common form in HIV-infected patients. 6 The patient could have been in either prolonged seroconversion phase of HIV or a rapid progressive phase when his initial CD4 counts were done. The patient did not have any other concomitant infection, change in ART, or constitutional illness at the time of presentation.
Although various infections have been mentioned as manifestations of IRIS, syphilis has very rarely been mentioned in this regard. Neurosyphilis occurring as IRIS has been mentioned in one previous report. 7 Two cases of eye involvement in syphilis occurring as probably a manifestation of IRIS has also been reported before. 8, 9 A solitary case of a probable secondary syphilis manifesting as IRIs has been reported previously in literature. 10 Hence, this is a very rare instance of secondary syphilis presenting as IRIS in an HIV-positive patient.
Another lesson learnt from the patient was that we should do VDRL testing with prozone and TPHA in all HIV-positive patients to not to miss a diagnosis of syphilis, though they may have still have been negative in this case.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.