
Abstract
Coccidioidomycosis causes substantial morbidity and mortality in endemic areas, and dissemination is frequent in patients with impaired cellular immunity such as AIDS. Immune reconstitution inflammatory syndrome (IRIS) is paradoxical clinical worsening after initiation of antiretroviral therapy (ART) in a patient with HIV and a simultaneous opportunistic infection (OI). Immune reconstitution inflammatory syndrome has been well described for a host of mycobacterial, viral, and fungal OIs and malignancies such as Kaposi sarcoma. To date, only 3 cases of IRIS due to coccidioidomycosis have been reported in the literature. At our institution, we report 4 cases of IRIS in HIV-infected patients with disseminated coccidioidomycosis. Unfortunately, all 4 patients died of worsening coccidioidal infection after initiating ART. The optimal timing of ART in patients with AIDS and coccidioidomycosis remains to be elucidated.
Introduction
Coccidioidomycosis can be a devastating opportunistic infection (OI) in immunocompromised hosts such as people living with HIV/AIDS. Being located in the heart of the San Joaquin Valley in Central California, our institution is a tertiary referral center for treatment of coccidioidomycosis. Fresno County has a prevalence rate of 110 per 100 000 people infected with HIV, 1 for whom our Ryan White–funded clinic provides care. An estimated 55% of these patients are of Hispanic or Latino ethnicity. California has the second highest number of HIV cases in the nation according to the surveillance data from the Centers for Disease Control and Prevention (CDC). 2 Patients who commence antiretroviral therapy (ART) with advanced immunosuppression are at risk of considerable morbidity and mortality due to immune reconstitution inflammatory syndrome (IRIS), which is a pathological inflammatory response usually directed toward microbial antigens. The main independent predictor of IRIS is a low CD4 count at initiation of HIV treatment, with a higher risk in patients with CD4 counts <50 cells/mm3. 3,4 There is a paucity of literature pertaining to the incidence of IRIS in HIV-infected patients who have coccidioidomycosis. To date, only 3 cases have been reported, 1 of which was published previously from our institution. 5
Immune reconstitution inflammatory syndrome presents as 2 distinct temporal patterns of disease: “unmasking IRIS” and “paradoxical IRIS”. 6 It typically occurs within the first 6 months of ART. In unmasking IRIS, a new OI presents with a marked inflammatory component following ART initiation. Paradoxical IRIS is clinical deterioration of a known OI for which treatment is already being provided and to which the condition at first responded but recurs or becomes acutely worse after ART initiation. Consensus case definitions have been established for IRIS secondary to cryptococcosis and tuberculosis (TB). 6 –8 For the following case series, the definition of coccidioidal IRIS required (1) a preexisting diagnosis of coccidioidomycosis, (2) improvement in antifungal therapy, (3) the development of inflammatory symptoms due to coccidioides after initiating ART, (4) immune reconstitution as evidenced by an increase in CD4 count or a decrease in HIV RNA or both, and (5) the absence of an alternate diagnosis to explain the symptoms.
The 2016 Infectious Diseases Society of America (IDSA) Clinical Practice Guideline for the Treatment of Coccidioidomycosis states that initiation of potent ART should not be delayed because of the concern about coccidioidal IRIS. 9 This is a strong recommendation, however, with a low level of supporting evidence. We review the current literature and present 4 cases of coccidioidal IRIS from our institution, all of which proved fatal.
Case 1
A 37-year-old incarcerated Caucasian female was diagnosed with HIV-1 infection in 2003 but remained ART naive since diagnosis. In 2012, she was brought from the penitentiary with fever, chills, night sweats, cough, and weight loss. Her CD4 count was 44 cells/mm3, and HIV RNA was 170 077 copies/mL. Chest radiograph findings were consistent with pneumonia, and she was diagnosed with pulmonary coccidioidomycosis based on a serum complement fixation (CF) titer of 1:128. Other microbiologic studies were negative. A lumbar puncture was performed, and cerebrospinal fluid (CSF) was positive for coccidioides antibody by immunodiffusion (ID) only. Oral fluconazole 800 mg daily was initiated for disseminated coccidioidomycosis. After 2 weeks, she improved clinically and was discharged on fluconazole 600 mg daily (the dose was decreased due to alopecia).
Two months later, she began ART as an outpatient with a fixed dose single-pill regimen of tenofovir (TDF), emtricitabine, elvitegravir, and cobicistat. At that point, her serum coccidioides CF titer had decreased to 1:64, and she showed clinical improvement. Three weeks after initiating ART, she developed fever, a diffuse erythematous rash, cough, fatigue, and weakness. The patient was hospitalized once again, and ART was discontinued due to concern for a possible drug reaction. Her CD4 count at that time had increased to 225 cells/mm3. She was found to have a positive serum TB-QuantiFeron Gold assay, and due to suspected unmasking of TB, 4-drug antitubercular therapy was initiated. Sputum cultures were repeatedly negative for acid-fast bacilli, however. The patient developed elevated liver transaminases leading to the discontinuation of anti-TB medications, and all workup for active TB infection remained negative. With supportive care, her fever, rash, and cough resolved with no new infections identified. Due to persistent transaminitis, she was discharged on an adjusted fluconazole dose of 400 mg/d.
One month after discontinuing ART, the CD4 count had declined to 73 cells/mm3, with a corresponding rebound increase in HIV RNA viral load of 1.1 million copies/mL. Antiretroviral therapy was resumed with fixed dose of TDF, emtricitabine, and efavirenz (EFV).
A month after resuming ART, she presented with anorexia, weight loss, worsening cough, fatigue, fever, and somnolence. She was hospitalized for failure to thrive. Serum coccidioides CF titer increased to 1:512, while lumbar puncture was positive for a CSF titer of 1:4, and bronchoalveolar lavage revealed coccidioides spherules on fungal staining. During this hospitalization, ART and fluconazole were both continued. Magnetic resonance imaging (MRI) of the brain was performed due to her progressive neurological deficits and showed new ring-enhancing cerebellar and cortical lesions (Figure 1). Unfortunately, a brain biopsy could not be performed as the patient had become comatose, and she expired 35 days after admission.
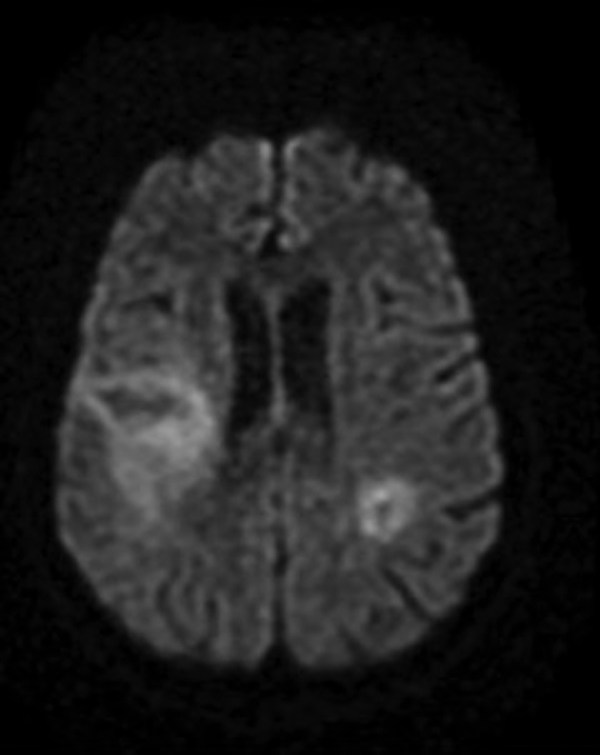
Magnetic resonance imaging (MRI) of the brain: ring-enhancing cerebellar and cortical lesions. The patient had multiple areas of restricted diffusion signal with corresponding T2 hyperintensity along the gyri of the right posterior frontoparietal lobe, right corona radiata, left and right parietal lobes, and an area of the left cerebellum with rim enhancement using gadolinium.
Case 2
A 41-year-old African American male was diagnosed with HIV in 2012 but was nonadherent to ART. In 2013, he was hospitalized with cutaneous abscesses on the face and nose, and biopsy demonstrated coccidioides spherules (Figure 2). Fluconazole was initiated but the patient was noncompliant with this as well. In 2015, he presented to the hospital with a severe frontal headache, fever, and confusion. His CD4 count was <20 cells/mm3 and HIV RNA was 23 489 copies/mL. The CSF showed a high opening pressure (380 mm H2O) and coccidioides CF titer of 1:2, with a corresponding serum CF titer of 1:8. Computed tomography (CT) scan of the head was significant for ventriculomegaly with communicating hydrocephalus. The CT chest showed multiple small nodules within the lung apices. Fluconazole 1000 mg/d was initiated. His hospital course was complicated by persistently elevated intracranial pressure requiring daily therapeutic lumbar punctures and eventually placement of a ventriculoperitoneal shunt. Intravenous liposomal amphotericin B was substituted for oral fluconazole. The patient’s mentation and headaches improved, and his skin lesions decreased in size.

Cutaneous abscesses on the face and nose. Biopsy demonstrated coccidioides spherules.
After three weeks of antifungal therapy, ART was initiated with TDF, emtricitabine, dolutegravir, darunavir, and cobicistat. Eight days later, the patient became confused and somnolent with nausea, vomiting, and developed seizures. He was intubated, and repeat CT of the chest showed worsening diffuse nodular opacities. Brain MRI showed bilateral multifocal infarcts, intraventricular hemorrhage, and diffuse cerebritis. Cultures from bronchoscopy grew Coccidioides immitis. All other infectious workup was negative. The CSF coccidioidal CF titer was repeated and was 1:4; CSF culture grew C immitis. The serum CF titer increased to 1:32. His facial lesions, which had significantly improved with antifungal treatment alone, now worsened and paradoxically increased in size. His condition deteriorated rapidly and he expired 2 weeks after ART initiation.
Case 3
A 27-year-old Hispanic male was diagnosed with HIV infection in 2013 and refused ART. When he returned to care in 2015, his CD4 count was 149 cells/mm3 with HIV RNA 126 028 copies/mL. He presented to the hospital with 2 weeks of fever, fatigue, and productive cough. Initial CT of the chest showed diffuse bilateral reticulonodular and interstitial opacities with serum coccidioides CF titer of 1:256. Sputum fungal cultures and blood cultures drawn on admission both grew C immitis. Other infectious workup including CSF analysis was negative. Oral fluconazole was initiated; however, within 4 days the patient developed marked transaminitis and liposomal amphotericin B was substituted. Despite 3 weeks of antifungal treatment, his hypoxia did not improve. Imaging of the chest, abdomen, and pelvis demonstrated extensive micronodular opacities in the lungs with a miliary pattern, hepatosplenomegaly, and innumerable nodules in the spleen.
After 21 days of amphotericin B, skin biopsy of a violaceous forearm lesion was performed, which was consistent with Kaposi sarcoma. The patient had similar lesions on his torso and feet, and a serum human herpes virus 8 (HHV-8) DNA of 8028 copies/mL. Antiretroviral therapy with darunavir, ritonavir (RTV), abacavir (ABC), and lamivudine (3TC) was initiated at this time.
One month later while on ART, the CD4 count was 255 cells/mm3 with HIV RNA <20 copies/mL. The patient remained hospitalized due to steady respiratory decompensation, and bronchoscopy revealed diffuse flat erythematous lesions in the airways consistent with pulmonary Kaposi sarcoma. Bronchial lavage fluid was positive for C immitis by Grocott’s methenamine silver (GMS) stain and by fungal culture; immunostaining showed that it was also positive for HHV-8. A liver biopsy performed to workup the nodules seen on imaging demonstrated granulomatous portal inflammation with numerous spherules of C immitis and was negative for HHV-8 (Figure 3). Coccidioides immitis spherules were also found on bone marrow biopsy (Figure 4). Coccidioides serum titer by quantitative ID was 1:128 and HHV-8 DNA increased to 400 000 copies/mL.

Liver biopsy hematoxylin and eosin stain, 40× magnification. Granulomatous portal inflammation with numerous spherules of Coccidioides immitis.

Coccidioides immitis spherules in bone marrow biopsy, Grocott’s methenamine silver (GMS) stain.
Due to clinical deterioration, the patient was deemed a poor candidate for systemic chemotherapy of Kaposi sarcoma. He developed hypercapnic hypoxemic respiratory failure requiring intubation and mechanical ventilation. Despite 3 months of antifungal therapy, the patient expired 1 month after the initiation of ART.
Case 4
A 43-year-old Hispanic male was diagnosed with HIV in 2014, with a CD4 count <20 cells/mm3 at presentation. He discontinued his ART regimen of fixed-dose EFV, emtricitabine, and TDF after less than 1 year. He returned to care with symptoms of community-acquired pneumonia in 2015 and was hospitalized with a CD4 count of 21 cells/mm3 and HIV RNA of 239 624 copies/mL. Coccidioides serology was repeatedly negative, but due to the finding of mediastinal lymphadenopathy and dense consolidation of the lingula on CT of the chest, the patient underwent bronchoscopy. Bronchoalveolar lavage fungal culture grew C immitis, thus fluconazole 400 mg/d was commenced. When blood cultures drawn on admission grew C immitis, fluconazole was changed to liposomal amphotericin B.
He had a good clinical response to 4 weeks of intravenous amphotericin, after which oral fluconazole 600 mg/d was resumed. Antiretroviral therapy was simultaneously initiated at this time, with fixed-dose ABC, 3TC, and dolutegravir. The patient’s condition improved, and he was discharged home.
Ten days later, he returned to the hospital with fever, hypotension, night sweats, and worsened productive cough. Repeat CD4 count was 22 cells/mm3, while HIV RNA decreased to 74 copies/mL. Fluconazole and ART were continued, and laboratory investigation was negative for any other infectious etiology. Chest CT demonstrated progression of innumerable pulmonary nodules, while coccidioides serology remained negative. A diagnosis of IRIS was made as the patient improved with supportive care and was able to return home after 1-week hospitalization. However, 5 days later, the patient had a cardiopulmonary arrest at home and expired despite attempts to resuscitate.
Discussion
Paradoxical IRIS in HIV infection is the clinical worsening of a known infection of inflammatory condition after initiation of ART. 6,7 The underlying illness could be due to mycobacterial, fungal, or viral infection or malignancy. There is no single commonly held definition of IRIS, but common aspects include temporal association with ART, unusual clinical manifestations, an unexpected clinical course, exclusion of alternative explanations, evidence of immune restoration, histopathological appearance of unexpectedly florid cell–mediated response, and a preceding fall in plasma HIV-1 load. 6,7,10 –12 Paradoxical IRIS is a diagnosis of exclusion, as a patient’s deterioration after ART requires that a new OI be ruled out and only the known preexisting condition is present.
In all the 4 cases presented here (summarized in Table 1), clinical improvement occurred with antifungal treatment of coccidioidomycosis, and all 4 deteriorated after initiation of ART. At reevaluation, no new infections were found. Clinical signs and symptoms and radiologic findings showed marked inflammation at the time of clinical worsening. Patient 3 was diagnosed with Kaposi sarcoma at the time of IRIS presentation, and in his case, it is possible that the pulmonary IRIS was due to both KS and coccidioidomycosis.
The duration of antifungal therapy prior to ART initiation ranged from 21 to 60 days. Signs and symptoms of IRIS occurred from 8 to 30 days after ART was started (Table 2). Two patients had increases in the CD4 count, and 2 had decreases in their HIV RNA measured at the time of IRIS manifestation. Two patients had persistently negative serology for coccidioidomycosis despite fungemia and pneumonia, reflecting profound immunosuppression. In the previous case report of coccidioidal IRIS from our institution (case 5 in Tables 1 and 2), the patient presented with pneumonia, and ART was begun 41 days after antifungal therapy with fluconazole. 5 The patient’s CD4 count improved from 30 to 154 cells/mm3, while his HIV viral load dropped to <50 copies/mL. Twenty-seven months after initiating ART, IRIS manifested as superior vena cava syndrome. In this case series, none of the patients were given corticosteroids as IRIS was not readily recognized and other OIs had to be ruled out.
Criteria for Immune Reconstitution Inflammatory Syndrome in HIV-Infected Patients With Preexisting Coccidioidomycosis.

Abbreviation: ART, antiretroviral therapy.
aImmune reconstitution: an increase in CD4 count, decrease in HIV viral load, or both.
bSee Reference 5.
Summary of cases.
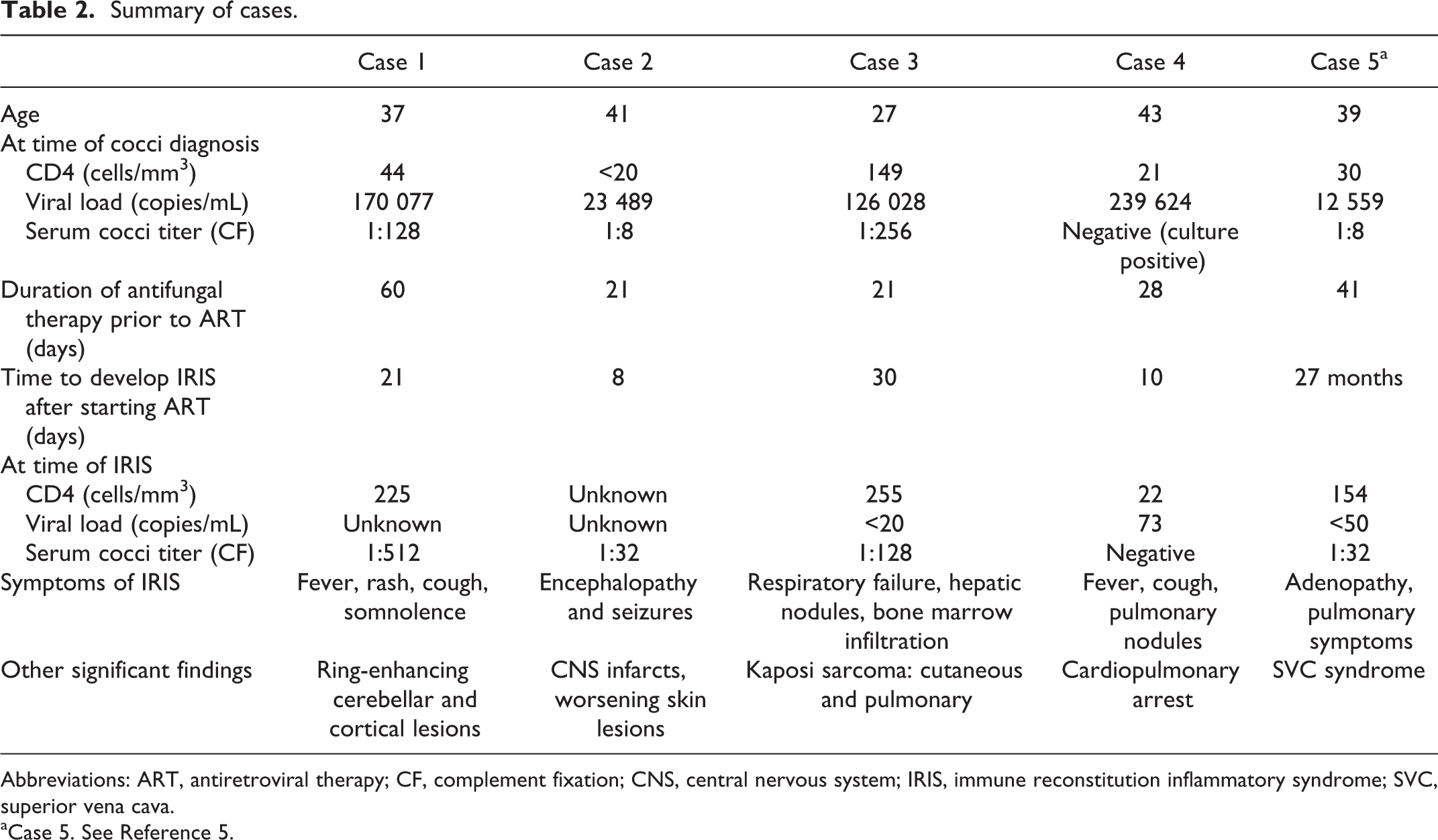
Abbreviations: ART, antiretroviral therapy; CF, complement fixation; CNS, central nervous system; IRIS, immune reconstitution inflammatory syndrome; SVC, superior vena cava.
aCase 5. See Reference 5.
Although IRIS is most common within the first 90 days of ART for a wide range of opportunistic pathogens, including cryptococcal meningitis, Shelburne et al noted a range up to 2 years, 12 while Skiest et al reported 3 years. 13 Only 1 other case of IRIS-associated coccidioidal meningitis has been published to date, in which a 59-year-old African American male in Atlanta presented with headache, photophobia, and nuchal rigidity 2 months after initiating ART with a rise in CD4 count from 45 to 163 cells/mm3. The patient died in 7 days after hospitalization despite empiric antifungal therapy with voriconazole. Coccidioides spherules with characteristic granulomas were found in the brain and lungs postmortem. 14 In the patients described here, both pulmonary and CNS inflammation were severe enough to lead to the patient’s death. Two cases reports of IRIS presenting as coccidioidal lymphadenopathy resulted in marked morbidity. 5,15 One cohort study of head and neck manifestations of IRIS among Mexican HIV-infected patients found Kaposi sarcoma to be the leading cause, with the majority of patients manifesting symptoms within the first 2 months. 16
The pathogenesis of IRIS is not well-defined, but it is believed that CD4 recovery with ART generates exuberant responses that result in the inflammatory reaction. A low pre-ART CD4 count and high viral load have been associated with higher risk of developing IRIS. The other primary risk factor for the development of IRIS is the duration of treatment of the underlying infection prior to initiation of ART. For cryptococcal meningitis, studies have demonstrated that it is important to wait to complete 5 weeks of antifungal treatment prior to initiating ART. The delay in initiating ART has been shown to decrease IRIS-associated mortality. 17 Based on the mortality seen in our patients where ART was initiated after 21 days of antifungal therapy (median 28 days), we hypothesize that delaying ART to complete a longer duration of antifungal treatment first, as is done for cryptococcal meningitis, could reduce the risk of severe IRIS in patients with AIDS and coccidioidomycosis.
The optimal timing of ART in patients with AIDS and coccidioidomycosis remains to be elucidated. From these cases, we are unable to draw a conclusion regarding the optimal timing of ART after diagnosis of coccidioidomycosis. Onset of IRIS varied from 1 week to 1 month except in the case of the patient with lymphadenitis causing superior vena cava syndrome 27 months after being on ART. As mentioned earlier, our hospital in the San Joaquin Valley is a tertiary referral center for treatment of coccidioidomycosis. We have had experience with other patients coinfected with HIV and coccidioidomycosis who did not develop IRIS when given ART. However, we would suggest that some degree of caution would be prudent despite IDSA’s current guidelines for treatment of coccidioidomycosis in HIV-infected patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.