
Abstract
The study sought to describe the quality-of-life impairments in newly diagnosed HIV-infected adult patients with cutaneous lesions. This was a hospital-based, cross-sectional, descriptive study of 160 newly diagnosed HIV-infected adult patients attending the HIV/AIDS clinic of University of Ilorin Teaching Hospital (UITH). Systemic random sampling technique was used in recruiting respondents for the study. The Dermatology Life Quality Index (DLQI) was used to gauge the quality-of-life impairments. The study showed high prevalence of cutaneous lesions in HIV-infected patients. Majority of the respondents (83.7%) scored more than 10 in DLQI score. This signifies that the skin lesions had large negative effects on their quality of life. The assessment of the impact of dermatoses on patients’ quality of life is important for clinical management. It is pertinent to detect patients at higher risk of experiencing worse quality of life in order to treat them holistically.
Introduction
Quality of life (QOL) attempts to measure the perceptions of individuals on their overall sense of well-being and includes aspects such as happiness and satisfaction with life as a whole.
World Health Organization has defined QOL as individuals’ perceptions of their position in life, in the context of the culture and value systems in which they live and in relation to their goals, standards, expectations, and concerns. 1 With the recent advance in clinical tests and treatments for those infected with HIV, the survival of these patients has increased and so is their QOL. Quality of life has become an important focus for researchers and health care providers. 2
In the last decade, there has been an increasing interest in assessing the QOL of patients with skin diseases as well as in the development of method of assessment. 3 ,4 The Dermatology Life Quality Index (DLQI) is one of QOL questionnaires that are specifically designed for skin diseases. 3
Skin lesions are among the most common diseases seen in primary care settings in tropical areas; hence ignoring them is not a viable option. Although mortality from skin lesions is not rife, compared with other ailments, people’s needs for effective remedies should be met for a number of important reasons. Besides, significant morbidity is caused by disfigurement, disability, or symptoms such as intractable itching, and reduction in QOL. Furthermore, basic knowledge of the simple features of diseases, whose presenting sign occurs in the skin, is lacking at the primary care level. A shortage of skills in the basic management of skin diseases is a further confounding problem. 5
This study therefore becomes relevant, due to the paucity of data on dermatology QOL impairment in HIV-infected patients in Nigeria, in general, and Kwara State in particular. Lastly, dermatology QOL measurement assessed the burden of illness and allowed assessment of the outcomes of medical treatments
Methods
This study was conducted at the lentiviral clinic of Department of Family Medicine, University of Ilorin Teaching Hospital (UITH), Ilorin, Kwara State, Nigeria. It was a descriptive, cross-sectional study carried out from May 1 to November 30, 2009. The inclusion criteria were newly diagnosed (≥18 years) HIV-infected adult patients at the lentiviral clinic, who consented to participate in the study. Individuals on highly active antiretroviral therapy (HAART) prior to presentation and those who refused to participate were excluded.
The sample size was estimated using the Cochran formula
6

Therefore:

In order to take care of nonrespondents (assuming anticipated response was 90%) then:

Thus, an estimated sample size of 160 was used for the study. Systematic random sampling was used in recruiting respondents into the study. On average 2 new HIV-infected adult patients were referred daily from family medicine outpatient’s clinic as obtained from the record department. Weekly average attendances of 14 new HIV-infected adult patients were interviewed to obtain the total sample size of 160 in 6 months.
The sampling interval was therefore 336/160 = 2:1. On every clinic day, each folder was assigned a number code from 01 to 14. The starting point was randomly selected by simple balloting, whereby a paper was picked from folded pieces of paper bearing number 01 to 14. Therefore, every second folder was chosen for the study until the required sample was obtained for the week. This procedure was repeated every week until the required total sample size was obtained.
Ethical approval was obtained from the ethical review committee of UITH before commencement of the study.
Participants were recruited at the lentiviral clinic of the Department of Family Medicine, UITH, Ilorin. An informed consent was obtained from the participants after giving adequate information about the study. An interviewer-administered questionnaire was used, with provision for interpreter in local dialect, in those without formal education.
The QOL was measured using a specific questionnaire for skin diseases: the DLQI, which was the first questionnaire developed for assessing health-related QOL, specific to dermatology. It was developed by Finlay and Khan in 1994. 3 As required by Finlay and Khan, a specific authorization for its use was obtained by the authors. The DLQI grades the QOL by giving a score to each domain. The domains assessed by the DLQI are the following: physical symptoms and feelings (questions 1 and 2), (b) daily activities (questions 3 and 4), (c) leisure (questions 5 and 6), (d) work/school (question 7), (e) personal relationships (questions 8 and 9), and (f) treatment (question 10). The patients should answer the questions keeping in mind the obstacles faced during the previous week. The scores on the questionnaire range from 0 to 30. The higher the score is, the poorer the QOL. Results from 0 to 1 mean no effect on the patient’s QOL, scores of 2 to 5 mean a small effect, scores of 6 to 10, mean a moderate effect, scores of 11 to 20 correspond to a great effect, and scores of 21 to 30 mean a very important effect of the disease on the patients’ QOL. The questionnaire was applied to each patient during individual interviews carried out by trained interviewers.
Results
Table 1 below shows the sociodemographic characteristics of the respondents. Of the 160 participants studied, 120 (75%) were female while 40 (25%) were male. The male–female ratio was 1:3. A greater number of the respondents were Muslims 111 (69%) compared to Christians 47 (30%). Most of the respondents (120 [76%]) were of Yoruba extraction. Predominantly, 108 (68%) lived in an urban setting. The majority (63 [39%]) of the respondents had primary education, while 41 (26%) had secondary education. In all, 28 (17%) had tertiary education and the remaining had no formal education. Majority (104 [65%]) were in social class V. These comprised the unemployed, students, and those involved in unskilled occupations.
Sociodemographic Characteristics of Respondents.

Table 2 shows the spectrum and frequencies of skin disorders among the respondents. The most prevalent skin disorder was pruritic papular eruption in 39 (33.9%) while seborrheic dermatitis in 20 (17.4%), herpes zoster in 12 (10.4%), xerosis and ichthyosis in 6 (5.2%), tinea manuum/unguium in 6 (5.2%), scabies in 3 (2.6%) of the clinical manifestation. Kaposi sarcoma in 2 (1.8%) was the least commonly reported in the study
Spectrum of Skin Lesions among the Respondents.

n = Number of respondents affected by variable.
N = study population.
% = n/N x 100.
Table 3 shows the effects of skin lesions on the QOL of the respondents. Skin lesions had negative impacts on the QOL of 112 patients (96.5%). In all, 60 patients (51.3%) had a very large effect; 45 patients (39.1%) had extremely large effect while 7 patients (6.1%) had moderate effect. No effect on the QOL was found in 4 patients (3.5%). It was concluded therefore that there was profound QOL impairment, which was statistically significant (P < .001).
Effects of Skin Lesions on the Quality of Life of the Respondents.

χ 2 = 1.370, df = 3, P < .001.
Symptoms Associated with Skin Rash
Figure 1 shows symptoms associated with skin lesions in the participants (clinical evaluation of the dermatology of life quality index), 64% of those with mucocutaneous lesions complained of itching sometimes with painful rash. The lesions were a source of embarrassment (80%) to the patients, with (60%) affectation of their social or leisure activities. In all, 67 patients (58%) were prevented from doing their normal working or studying. In 65% of the respondents, the lesions created problems with their partners, close friends, and relatives. A total of 55 respondents (48%) agreed that the skin lesions influenced their sexual activities.

Symptoms associated with skin lesions in the Participants (clinical evaluation of the Dermatology Life Quality Index).
Figure 2 shows the prevalence of skin lesions associated with HIV infection in the study. Of the 160, 115 had skin disorders. This gave an overall prevalence rate of 72%.
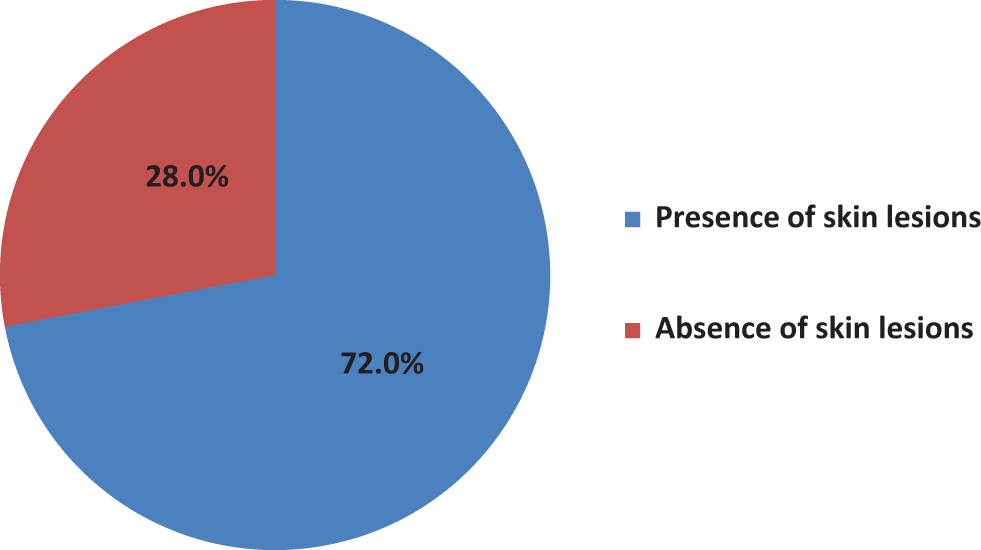
Prevalence of skin lesions in the participants.
Discussion
Skin diseases occurred in 72% of the newly diagnosed HIV-infected adults, attending the lentiviral clinic of the Department of Family Medicine, UITH.
The most frequently occurring skin lesion was pruritic papular eruption, with a prevalence of 33.9%. This confirms previous conclusions from other studies, of a high prevalence of pruritic papular eruption in the tropics and especially in Africa. 8,9
The common symptoms presented by the respondents were itching associated with rash 74 (64%). This is consistent with the general observations of Benjamin and Joel 10 that majority of the patients had pruritus (86 [75%]) and rash (90 [78%]). The rash and pruritus had significant effects on the QOL impairment on the patient.
In 92 (80%) of the patients, the mucocutaneous lesions were source of embarrassment. It affected not only their social activities (69 [60%]) but their sexual activities (55 [48%]) as well as relationship with partners, close friends, and relatives (75 [65%]). This is similar to Yanik et al 11 study on psychosocial impact of cutaneous lesions, where 77 (67%) had significant life impairment. It was also similar to Raju et al, 12 where there was considerable QOL impairment.
The study confirms that dermatological problems can result in psychosocial effects that seriously affect patients’ lives. More than a cosmetic nuisance, skin disease can cause anxiety and other psychological problems that affect patients’ lives in ways comparable to arthritis or other disabling illnesses.
Physicians caring for people living with HIV/AIDS should be familiar with the diagnosis and management of common mucocutaneous lesions in this population because prompt and appropriate management of these conditions will reduce morbidity and help improve QOL. It is important for physicians to create a positive mind-set in those living with the disease, because dermatology problems can result in psychological effects that seriously affect patients’ lives. Finally, the management of HIV disease should be multidisciplinary and holistic in approach.
Footnotes
Acknowledgments
I am extremely grateful to my mentor and trainer, Professor Olaniyi Onayemi of the Department of Dermatology and Venereology, Obafemi Awolowo University Teaching Hospital Complex (O.A.U.T.H.C) Ile-ife and to the Head of Dermatology & Venereology, Dr (Mrs) O. A. Olasode. I am also grateful to Dr Alabi K.M, Head of Department of Family Medicine and Dr Ayinmode L.O, Consultant Family Physicians, University of Ilorin Teaching hospital (UITH). I owe a debt of gratitude to Dr Aderibigbe S.A Consultant Physician, Department of Epidemiology and Community Health, University of Ilorin Teaching Hospital.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.