
Abstract
Early use of highly active antiretroviral treatment (ART) in people living with HIV for HIV prevention has gained legitimacy but remains controversial. Nineteen French HIV experts with diverse specializations (over half of whom were clinicians) were qualitatively interviewed on their views about ART irrespective of CD4 count of more than 500 cells/mm3 for purposes of HIV prevention, which is not systematically recommended in France. Content analysis identified 2 broad categories: individual considerations (subcategories: patient health and well-being; patient preparedness and choice) and collective considerations (subcategories: HIV transmission risk; impact on the epidemic; cost). Uncertainty surrounded many experts’ considerations, and unity was lacking on key issues (eg, candidacy for early preventive treatment, expected clinical- and population-level effects). An umbrella theme labeled “Weighing the merits of early ART in the face of uncertainties” was identified. Our analyses raise doubts about the current acceptability of widespread implementation of early ART for HIV prevention in France.
Introduction
Early use of highly active antiretroviral treatment (ART) in people living with HIV for HIV prevention has gained legitimacy, and updated treatment guidelines in some resource-rich settings reflect this. 1 –3 According to many mathematical models, maximizing the public health impact of treatment as prevention (TasP) requires treating with ART all or virtually all individuals diagnosed with HIV. 4 –6 This prospect, however, raises many concerns (eg, ethical, financial, and behavioral) 7 and is at odds with medical guidelines that largely rely on CD4 counts to determine when to initiate ART. 8 Deciding “when to start” ART remains an important unresolved issue in HIV treatment, and no randomized clinical trial data are yet available on the clinical benefit of treatment when CD4 counts exceed 500 cells/mm3. 9
In France, 2009 to 2010 saw the publication of multiple official reports indicating a paradigm shift in HIV prevention, with a novel focus on HIV prevention and the integration of TasP. 10 These include a report by the French National AIDS Council on the role of treatment in fighting the HIV epidemic, 11 a report on prevention and risk reduction in high-risk groups against HIV and sexually transmitted infection (STI), 12 the 2010 French guidelines for the medical care of people with HIV, 13 and the national plan for fighting HIV/AIDS-STI, which, for the first time, adopted a combination prevention strategy of behavioral prevention, expanded HIV testing, and earlier ART, as recommended by the former reports. 14 To some extent, because of its strong emphasis on HIV testing and treatment, France is considered a setting where a natural experiment with TasP has taken place. 15 However, TasP has been the object of controversy in France, 16 and the country’s HIV medical guidelines are more cautious toward it 17 than those in the United States, for example. 2 Among asymptomatic patients, ART is recommended for those with a CD4 count between 350 and 500 cells/mm3 and, among those with more than 500 cells/mm3, the clinician’s decision to begin ART can take account of the objective of reducing the risk of sexual HIV transmission. 13 Treatment of patients with a CD4 count of more than 500 cells/mm3 is thus not systematically recommended. The government’s 2010 to 2014 national plan for HIV/AIDS-STI does propose to study the possibility of immediately and continuously treating newly diagnosed HIV-positive persons with ART. 14
In a context of growing international interest in TasP, this study’s objective was to analyze French HIV experts’ main considerations in regard to early ART for HIV prevention to better ascertain the feasibility of its broader implementation. This study adds to current research premised on the notion that a better understanding of stakeholders’ attitudes toward early ART is essential to this project. 18 –20
Methods
Participants
Diverse HIV experts were recruited to participate in a qualitative study aimed at understanding whether and how a “test and treat” strategy should be implemented in France. A sample of 19 HIV experts participated (5 women and 14 men). Expertise was defined on the basis of either contributing as an expert to the latest French recommendations for the medical care of HIV-infected persons 13 (n = 15) or being referred as a good candidate for the study by one of these experts (n = 4). Experts had worked in the HIV field for a mean of 24.6 years (standard deviation = 5.1 years). Most (16) currently worked in Paris and over half (11) were practicing clinicians. Other occupations represented include virologist (4), AIDS service organization worker (2), and researcher (3). Table 1 provides additional information on the participants. Given the sample’s high-profile membership, to protect the experts’ identities, citations provided here are accompanied by minimal information on their producers.
Characteristics of the Sample of French HIV Experts.a
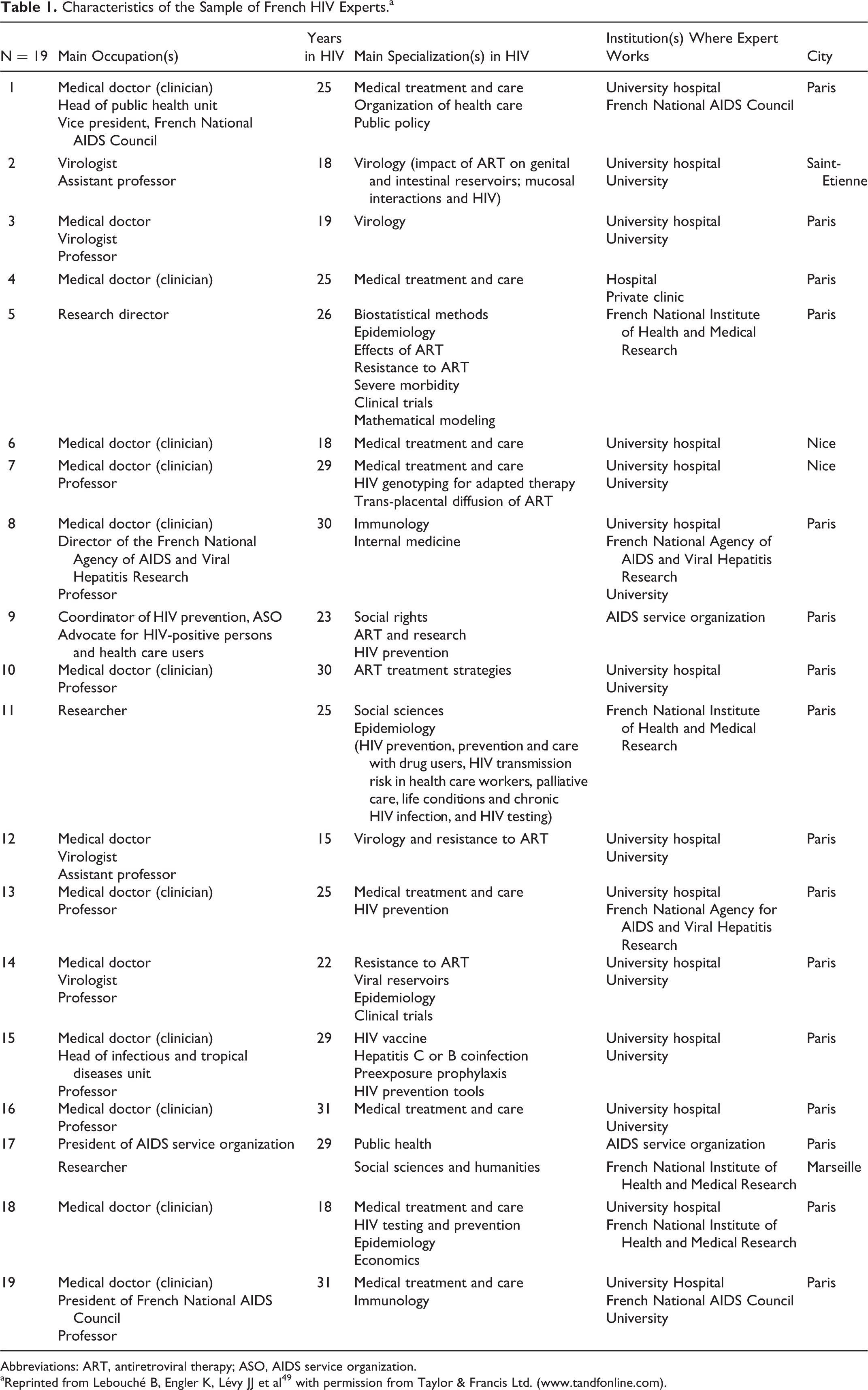
Abbreviations: ART, antiretroviral therapy; ASO, AIDS service organization.
aReprinted from Lebouché B, Engler K, Lévy JJ et al49 with permission from Taylor & Francis Ltd. (www.tandfonline.com).
The Interview
Interviews, led by Bertrand Lebouché in French, were conducted from February to July 2011, following a semistructured format. They examined experts’ opinion of test and treat, how testing and treatment should proceed in this context, and barriers to its implementation. Interviews lasted, on average, for 64 minutes and were audio recorded. Interviewees provided written consent, following an explanation of the study and of what participation entailed.
Ethics Approval
Ethics approval for the study was obtained from a Research Ethics Board of the McGill University Health Centre, Montreal, Quebec, and in Lyon, France, from the Comité de Protection des Personnes of Hôtel-Dieu hospital.
Qualitative Analysis
The audio recorded interviews were transcribed verbatim, entered into the software Atlas-ti (5.2), and analyzed with content analysis. 21 The interview material was initially divided into 20 broad and minimally interpreted content areas 22 with Atlas.ti. The content area pertaining to the decision to treat people living with HIV early with ART for prevention was analyzed for this article. Analysis of this content produced a hierarchy of categories (2), subcategories (5), and codes (16), which were fine-tuned and continuously verified against the original transcripts. An underlying theme was found to cut across these constructs. 22 The analyses and their component interview excerpts were discussed and agreed upon by the research team. The person responsible for analysis (Kim Engler) had minimal information on the interview participants and was not present at the interviews.
Results
On the decision to treat people living with HIV early for prevention, experts’ main considerations could be grouped into 2 broad categories: considering the individual (subcategories: patient health and well-being; patient preparedness and choice), illustrated in Table 2, and considering the collective (subcategories: HIV transmission risk; impact on the epidemic; cost), illustrated in Table 3.
Experts’ Individual Considerations for Treatment as Prevention: Subcategories, Codes, and Example Citations.a

a All citations presented are translations agreed upon by Bertrand Lebouché and Kim Engler.
Experts’ Collective Considerations for Treatment as Prevention: Subcategories, Codes, and Example Citations.

a All citations presented are translations agreed upon by Bertrand Lebouché and Kim Engler.
Considering the Individual in ART for Prevention
Patient health and well-being
Most experts addressed considerations related to patient health and well-being (16; 84%). Six codes compose this subcategory of individual considerations. Experts advanced that “arguments” supported the possibility of individual clinical gains from early ART, which, for some, were either sufficient reason to treat early or becoming more and more numerous (eg, inflammation theory, normalization of CD4 counts, reduction/elimination of viral load, improvement in quality of life). Only 1 expert stated that there were “scientific proofs” of these gains. Experts also mentioned the unknown or potentially negative effects of having a replicating and/or expanding virus in the absence of treatment. A second issue often emphasized was that ARTs have improved (eg, they are less toxic, offer lower probabilities of resistance, are better tolerated, easier to take, and cause less lipodystrophy). Two experts spoke of the possibility of medical breakthroughs via early ART (ie, converting HIV type 1 into an ancestral retrovirus; eradicating HIV reservoirs) and 2 others highlighted ART’s role in the reduction of patients’ fears and risk of infecting their partner/partners, providing well-being-enhancing reassurance through its impact on viral load and infectiousness.
Experts also provided reasons for not treating early, pointing to the unknown, unproven (or not sufficiently so), or not unanimously accepted interest of early ART in terms of individual clinical benefits (eg, on inflammation and its associated complications, morbidity) as well as the potential deleterious effects of ART, particularly, in the long term (eg, toxicity, reduced efficacy after decades of use).
Patient preparedness and choice
Patient preparedness and choice was the second most important subcategory of individual-focused considerations. Over half (11; 58%) of the experts mentioned this issue and, many, in regard to the often discounted assumption that individuals would not be ready for, accept, or want early treatment for prevention. Four codes compose this subcategory.
The issue of patient demand was mainly broached to underscore that patients are indeed demanding treatment for prevention. Experts described cases of individuals seeking treatment, because they wanted peace of mind, had difficulty with/were not practicing safer sex, did not want to infect their partners, and/or wanted to limit their infectiousness. Experts contributing to this subcategory did not agree, however, on the extent of demand for preventive ART, generating a range of characterizations from “a lot” to “marginal.”
Deciding for patients either by forcing, imposing, or not honoring the right to refuse ART for prevention or, conversely, by not allowing freedom of choice by not informing patients about it was emphasized as unacceptable or unethical by some experts. Often, these aspects of patient choice were raised against the notion that a test and treat strategy would require universal treatment, if not, treating patients against their will.
Patient acceptance of preventive ART was especially broached in terms of the role of doctors in facilitating it. Experts proposed that provided the clinician was convinced of its advantages and/or adequately explained these to their patient, acceptance would generally be forthcoming. That acceptance might vary depending on the patient (eg, perhaps more likely if they are part of a sero-different couple) was pointed out by 1 expert.
Finally, a few (3) experts discussed patient readiness in regard to preventive ART, presenting it as either the best condition in which to initiate treatment, as possibly requiring time to develop, or, in its absence, as a reason not to begin treatment.
Considering the Collective in ART for Prevention
Another central analytical category in experts’ discussion of early ART for prevention was collective considerations. Its subcategories are (sexual) HIV transmission risk, impact on the epidemic, and cost.
HIV transmission risk
Regarding HIV transmission risk (15; 78.9%), composed of 2 codes, many experts acknowledged ART’s potential to reduce the risk of sexual transmission to partners and explained that current French recommendations permitted ART for those with a CD4 count of more than 500 cells/mm3 if there was risk of transmission or unprotected sexual behavior (among other reasons to initiate treatment at this stage). Experts diverged, however, in their interpretation of risk in terms of the features of those who would be appropriate candidates for preventive ART due to their transmission risk. Several mentioned sero-different couples (where 1 partner is HIV positive and the other is HIV negative) as candidates for preventive ART (5), particularly if they were not using protection systematically. Other characteristics associated with candidature for preventive ART, which could be combined, were being a sex worker, of foreign origin, a gay man, having multiple partners, using sex venues, engaging in unprotected sex, and simply being HIV positive. Interestingly, behavioral features associated with suboptimal candidature for preventive ART included 2 of these: engaging in unprotected sex (ie, arguing that prevention overall is unlikely to succeed in this context) and having multiple partners (arguing that individuals part of a sero-different couple are more appropriate candidates). Two experts underscored that homosexual/gay men with many partners or who did not practice safer sex were not well integrated into the French recommendations on transmission risk, which might partially explain these contradictions.
Experts also disagreed on prevention’s sufficiency as a reason to treat. Some emphasized that individual considerations had priority over those of the collective, with the HIV-positive person’s health taking precedence over benefits for partner or population health. In this context, HIV prevention as an indication for treatment was allowed as long as clinical gains were also likely or as “the cherry on the cake,” as 2 experts stated. Conversely, others were favorable to treating patients early with ART for the sole purpose of protecting partners.
Impact on the epidemic
The subcategory, impact on the epidemic (17; 89.5%), has 3 component codes and relates, in part, to the perceived likelihood of positive impacts of early ART (alone or within a test and treat strategy) on the HIV epidemic and public health. Experts varied on this issue. A positive impact on the epidemic, often discussed in terms of “collective benefit,” was deemed probable to certain by 7 experts. Positive impacts were characterized in terms of a reduction in the propagation, diffusion, incidence, or transmission of HIV and/or in the prevalence or circulation of resistant strains of the virus. For 5 experts, positive effects were unknown, as yet, poorly defined, or in need of further investigation, and others (4) believed that significant positive impacts on the HIV epidemic were unlikely Utopian.
Specific potential barriers to early treatment’s successful impact on the epidemic were mentioned by several experts (7). These related primarily to issues of early treatment acceptance (alone or as part of a test and treat strategy), adherence (eg, the selection of people into treatment who are refractory to HIV prevention; if people are poorly treated, there is a risk of emerging mutation; difficulties in maintaining long-term adherence), behavioral modifications as a result of the strategy (eg, increases in sexual risk practices); the possible role of primo infections in maintaining the epidemic; and potential blips in viral load (eg, provoked by STI). Experts could mention the possibility of group differences in potential barriers and their being problematic, specifically, in the population of gay men. Hence, some less favorable expectations about early treatment’s impact on the epidemic referred to the HIV epidemic in gay men or men who have sex with men (MSM). Other impediments to treatment’s impact on the epidemic concerned a view of HIV testing as the priority (9). Several experts pointed out that, under French guidelines, only a small minority of current patients are not treated and could be considered strictly for early preventive treatment (eg, “peanuts”). For some, this was directly related to inadequate testing to uncover more HIV-positive individuals at earlier stages of infection. Many experts more generally advanced that increasing the availability of testing was a greater priority than early treatment for dealing with the epidemic.
Cost
The final subcategory of collective considerations was cost, briefly broached by 3 (15.8%) experts and related to either the unknown or the non-cost-effectiveness of preventive ART (eg, when compared to the price of condoms).
Weighing the Merits of Early ART for Prevention in the Face of Uncertainties
How experts typically discussed the above considerations is best described as a weighing of the merits of ART for prevention in the face of uncertainties. Several experts spoke directly of a “problem,” “measure,” “balance,” “opposition,” or “appreciation” (or other variation) of “benefits–risks” in regard to early preventive ART whether for the individual, the collective, or both.
Experts varied in terms of how they resolved this weighing. Experts could believe, for example, in both individual and collective benefits; they could be more convinced of the individual than the collective benefits, or they could be more convinced of the collective than the individual benefit. Constant, however, is the consideration of multiple individual and/or collective factors as well as recognition of uncertainties in regard to early ART.
Uncertainty, as used here, is not meant to necessarily connote something negative or antonymic to hope. 23 Experts could claim to be favorable to widespread early ART (or treatment irrespective of CD4 count) despite recognition of uncertainties. Uncertainty refers to both possible limitations and positive potentials of early ART for the individual and the collective, particularly in terms of health, and to factors that may intervene or interfere with early ART use (eg, patient preparedness and choice, potential barriers). Uncertainties were indicated in myriad ways throughout the interviews, for example, through talk of risks, mention of lacking knowledge/research, and what can be termed experts’ “modality choices,” indicating something less than assertion. 24 Markers of modality include such terms as probably, potential, maybe, may, could, should, and possibly and several labels given to our analytical codes contain such terms.
Discussion
Our qualitative analyses suggest that for most French HIV experts in this study, the decision to treat early or universally for prevention is not a simple one. Multiple and complex individual and collective factors are considered and, regularly, the rapport between them. The interviews underscore what has been advanced by others that moving forward with treatment as prevention means keeping in mind both the individual and the societal good. 25 Experts’ many uncertainties, however, suggest that the benefits on both levels remain a matter of debate.
Patient Centeredness
On an individual level, a prominent consideration for experts was patient health and well-being, which centered on the different clinical implications of ART or its absence. Despite the potential benefit to public health of early or universal ART, the health and well-being of people living with HIV is clearly at the forefront of concerns. 2 For example, in a study by Kurth et al 18 on ART-prescribing clinicians’ attitudes toward early ART, although almost all (94.5%) respondents agreed that it can slow the spread of HIV in a community, the vast majority (92.0%) initiated ART for the patients’ own health and based on their readiness to take it.
The subcategory of patient health and well-being also included ART’s ability to reassure and lessen patients’ fears of transmitting the virus. A survey among the UK MSM found that 37.3% worry about passing on HIV to their partners, and that these worries are more common among men not on ART. 26 As others have highlighted, transmission fears, a motivator for the production of the controversial Swiss Statement, can interfere with the ability of people living with HIV to achieve aspects of a “normal” sex life, 27 including sexual pleasure, sexual intimacy, and procreation, if desired. 28 Hence, early ART could play a significant role in improving the sexual health and sexual well-being of people living with HIV.
As to patient preparedness and choice, the second subcategory of individual considerations, while discussions of universal treatment have been criticized for not attending to patient readiness, 9 in contrast, experts interviewed in our study spoke directly not only of patient readiness but especially of the patient demand, acceptance, and decision in regard to early ART. Indeed, several experts wanted to see French patients have greater decisional power in regard to ART for prevention and, for some, patient choice was served by clinicians’ informing HIV-positive individuals about the preventive potential of ART. Such a shift in decisional power has occurred, for example, in the British HIV Association’s latest draft guidelines for ART among adults, 1 which recommend that clinicians present to all patients the evidence that ART lowers the risk of transmission and that willing patients with CD4 count exceeding 350 cells/mm3 be accorded preventive treatment.
Variable Views on Early ART’s Collective Issues
Experts’ collective considerations were of 3 types. One, HIV transmission risk, contained heterogeneous views that spoke to the dilemma for experts of identifying appropriate candidates for early preventive ART (ie, Who is a transmission risk for others?) and whether HIV risk and the protection of others is reason enough to start the treatment early. HIV-positive individuals in sero-different couples were, on several occasions, presented as prototypical candidates for preventive ART. Experts disagreed on other profiles, including male homosexuality/gay identity and having multiple partners. This may be because little information on the preventive effect of ART in people living with HIV exists beyond sero-different couples and mother-to-child transmission, 29 and preventive ART’s legitimacy in these contexts is well established.
In France, where 47% of new infections in 2010 occurred in MSM, a group in which new infections rose between 2003 and 2010, 30 our findings on transmission risk suggest that there is a need for more deliberation to guide identification of target populations or candidates for early ART for HIV prevention. The literature has begun to explore strategies to identify priority groups to optimize the impact of early TasP (eg, expanding ART based on epidemiological impact, clinical impact, affordability/cost-effectiveness, feasibility, and acceptability). 31 In France, more research on specific populations with HIV, including MSM, that provides empirical data on key behaviors (eg, ART uptake and adherence, sexual practices), would be helpful to estimate the preventive benefits of early ART.
The expected impact of early ART on the epidemic, another collective consideration, also had a range of views, with many experts identifying potential barriers to positive benefits. This parallels the current equivocal evidence base on the population-level effect of treatment as prevention in high-income countries. 32 Furthermore, several of the experts interviewed favored improving HIV screening over early treatment (eg, to reduce the number of undiagnosed HIV-infected people, to detect them earlier) as a means of addressing the epidemic, a notion supported by others. 32,33 In France, it is estimated that 29 000 individuals have an undiagnosed HIV infection, 34 and although treatment is recommended in patients with a CD4 count of less than 500 cells/mm3, 30% of the new HIV diagnoses are among people living with HIV in a late stage of the disease (AIDS or less than 200 cells/mm3). 35 Improving this situation seems an important prerequisite of successful TasP in France. 36
Uncertainty
Experts’ uncertainties (expressed risk, potentials, unknowns, etc) surrounding early ART for HIV prevention is a key observation of this study. Although managing uncertainty and weighing benefits–risks is a recognized part of HIV medical practice, 3,37 many agree, for example, that the magnitude of long-term therapeutic benefits of ART at higher CD4 counts is uncertain. 31 Tellingly, in a survey of Australian ART prescribers, only 4.6% most strongly recommended ART initiation irrespective of CD4 count. 20 Quite possibly, no sooner than 2015 will results of the international and multisite Strategic Timing of AntiRetroviral Treatment (START) randomized trial be available on the clinical interest (risks and benefits) of treatment for HIV-infected people with CD4 counts of more than 500 cells/mm3. 38
Despite uncertainties, several of our study’s experts were ultimately favorable to early ART to treatment, irrespective of CD4 count, or to moving forward with a test and treat strategy. High-profile proponents of these approaches have themselves acknowledged important uncertainties. For example, Montaner 39(p209) has stated that “unequivocal answers are urgently needed” (eg, as to the utility of universal treatment), while Cohen 40(p1323) has urged pause and reflection, given that “The protection provided from ART is not absolute and is not absolutely predictable.” Having established that ART dramatically decreases HIV transmission in sero-different, mainly heterosexual couples in a clinical trial setting, 41 a current objective of HPTN 052 is indeed to examine the durability of this protective effect of ART. 42
The capacity of scientific evidence to eliminate uncertainty when assessing health risks is, however, partially limited by the unpredictability of people’s health behaviors. 43 Whether people would accept and adhere to preventive ART or modify their sexual practices (risk compensation) as a result of it were questions raised by the experts and deemed potential barriers to a successful public health impact of preventive ART on the HIV epidemic. These speak to concerns about the “real-world” implementation and repercussions of TasP, beyond clinical trial contexts and optimistic modeling, and the results of ecological studies on indicators of antiretroviral use and community viral load have been mixed in this regard. 44
Limitations
This study has limitations. The sample is one of convenience and is not necessarily representative of the full range of French expertise on HIV or of experts within each area of expertise. It likely overrepresents high-profile experts in the field, HIV clinicians (57.9% of the sample), and experts working in Paris (84.2% of the sample). Paris is disproportionately affected by the HIV epidemic. The number of new HIV cases in the Île-de-France region, consisting largely of the Paris metropolitan area, was over twice that of the national average in 2009 (24.3 versus 10.1 per 100 000 inhabitants), and 49% of 2010’s reported AIDS cases in France were tied to the region. 45 Furthermore, medical expertise, in general, is more highly concentrated in this region, containing, for example, a greater than average density of doctors (ie, 362.4 versus 306.2 doctors per 100 000 inhabitants). 46 Our findings must thus be weighed in relation to these sample biases. Other limitations of our study include the possibility that experts’ views may have changed in regard to TasP, given developments in HIV knowledge since February 2011, when interviewing began. Nevertheless, many issues raised by participants remain pertinent to discussions of TasP, and this study adds to a budding area of investigation concerned with different stakeholders’ attitudes toward early ART. 18,47
Conclusion
This interview-based study with French HIV experts offers an uncommon qualitative perspective on TasP and the issues it raises for individuals and the collective. It showcases the complexity of French experts’ considerations when weighing the merits of early ART for prevention, and uncertainties about this approach, whether invested with promise or precariousness. Our findings raise doubts about the general acceptability and immediate feasibility of widespread implementation of TasP in France, based on early or universal ART in people living with HIV. This seems consistent with the delayed revisions of HIV treatment guidelines in France, 17 which are now expected in the summer of 2013. 48 The range of concerns expressed by experts also points to TasP needing to be part of a comprehensive HIV-prevention program (eg, with expanded HIV testing, supports for ART adherence, sexual, and risk behavior interventions).
Footnotes
Acknowledgments
We wish to acknowledge the sponsor of this study, the Research Institute of the McGill University Health Centre. Warm thanks are extended to the study participants.
Authors’ Note
Merck Dhome Chibret France provided approximately 60 000 Euros to the McGill University Health Centre Research Institute (study sponsor) of which a portion went toward the funding of the study leading to the contribution. Merck Dhome Chibret France also paid the first author approximately 1000 Euros to promote the study's findings at the French national day of continuing education for doctors (ie, Dépister pour traiter: du diagnostic précoce au traitement à long terme, February 14, 2013, Pavillon Vendôme, Paris).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was made possible by a post-doctoral fellowship awarded to B.L. by the CIHR Canadian HIV Trials Network and an unrestricted educational fund provided by Merck Dhome Chibret France also to B.L.